
Abstract
Introduction:
Conventionally, confirmation of clinically significant prostate cancer (csPCa) (Gleason grade group ≥ 2) involves an initial multiparametric magnetic resonance imaging (mpMRI) followed by biopsy. Prostate biopsy incurs inherent risks of infection, bleeding, patient discomfort, and a 6-week delay before robot-assisted laparoscopic radical prostatectomy (RALP). We explored the feasibility of immediate RALP in men with PIRADS 5 lesions without preceding biopsy.
Methodology:
After obtaining institutional review board approval, a prospective analysis was conducted on 235 patients with PIRADS 5 lesions on mpMRI from December 2018 to February 2023. Patients were divided into 2 groups as follows: Group NoBiopsy (biopsy not done before RALP, cases, n = 118) and Group YesBiopsy (biopsy done before RALP, controls, n = 117). Baseline preoperative, intraoperative, and postoperative parameters were analyzed. Functional outcomes were monitored at 1, 3-, 6-, 9-, and 12-months follow-up post-RALP. Statistical analysis was performed using SPSS and STATA.
Results:
Ninety-five percent of cases and 87.17% controls had csPCa on final pathology post-RALP. Multivariable analysis did not find significant association between biopsy status and csPCa. Abnormal digital rectal examination (DRE), family history, preoperative PSA, and MRI lesion volume predicted csPCa. Significant differences were observed in console time (NoBiopsy vs. YesBiopsy, 60 ± 10 vs. 70 ± 9 minutes, p < 0.001) and estimated blood loss (80 ± 20 vs. 100 ± 30 mL, p < 0.01) between groups. At 6 months post-RALP, 96% of men in Group NoBiopsy were continent, compared with 88% of men in Group YesBiopsy (p < 0.04). All men in the study cohort were continent (0 pads) at 12 months post-RALP. Ninety-eight percent of cases and 92% of controls at 9 months and 12 months, respectively, were able to have penetrative sex with or without PDE-5 inhibitors post-RALP.
Conclusion:
RALP without antecedent prostate biopsy in men with PIRADS 5 lesions demonstrated substantial csPCa detection rates and superior functional outcomes, warranting further validation.
Introduction
With the changing landscape of recommendations against Prostate Cancer (PCa) screening, the incidence of clinically significant prostate cancer (csPCa) is increasing. 1,2 According to the National Cancer Institute (NCI), every American man has a lifetime risk of 11.6% of developing csPCa (Gleason 3 + 4 = 7, Gleason Grade Group 2 or higher). 3 This necessitates early detection and precise diagnosis for optimal treatment outcomes. Multiparametric magnetic resonance imaging (mpMRI) has emerged as a valuable tool, with a diagnostic accuracy of 95%, in detecting and characterizing PCa lesions. 4 –6 The Prostate Imaging Reporting and Data System (PIRADS v2) is a standardized system that utilizes mpMRI findings, with PIRADS 5 lesions indicating a high likelihood of csPCa. 7
Traditionally, confirming csPCa involved magnetic resonance imaging (MRI) followed by a biopsy. However, biopsies come with inherent risks such as infection, bleeding, anatomical distortion, and patient discomfort. 8,9 Robot-assisted laparoscopic prostatectomy (RALP) has become the gold standard for treating csPCa, offering benefits such as improved surgical precision, reduced blood loss, shorter hospital stays, and faster recovery times. 10
Numerous studies have investigated the effectiveness of diagnostic modalities such as prostate-specific membrane antigen positron emission tomography (PSMA PET), mpMRI, prostate-specific antigen density (PSAD), and prostate-specific antigen (PSA), both independently and in combination for diagnosing csPCa, with the aim of avoiding biopsy and directly proceeding with RALP. 11 –15 Given conflicting results on the performance of these diagnostic modalities and the associated risks of prostate biopsy, we sought to investigate whether men with PIRADS 5 lesions could be treated immediately by RALP. 8,9,11,12
Patients and Methods
After obtaining institutional review board ethical approval, 235 patients with PIRADS 5 lesions on mpMRI from a total pool of 1440 consecutive patients undergoing RALP were identified. (Fig. 1) Among these 235 patients, 118 had not undergone a biopsy before RALP (cases in Group NoBiopsy), whereas the remaining 117 had received a biopsy before RALP (controls in Group YesBiopsy). All patients were operated upon by a single high-volume surgeon at our institution between December 2018 and February 2023. The inclusion criteria included men with PIRADS 5 lesions on mpMRI having one or more of the following: a strong family history of PCa (≥ one 1st and/or ≥ two 2nd degree relatives), high PSA velocity, low free PSA, and abnormal digital rectal examination (DRE) coinciding with the location of PIRADS 5 lesions.
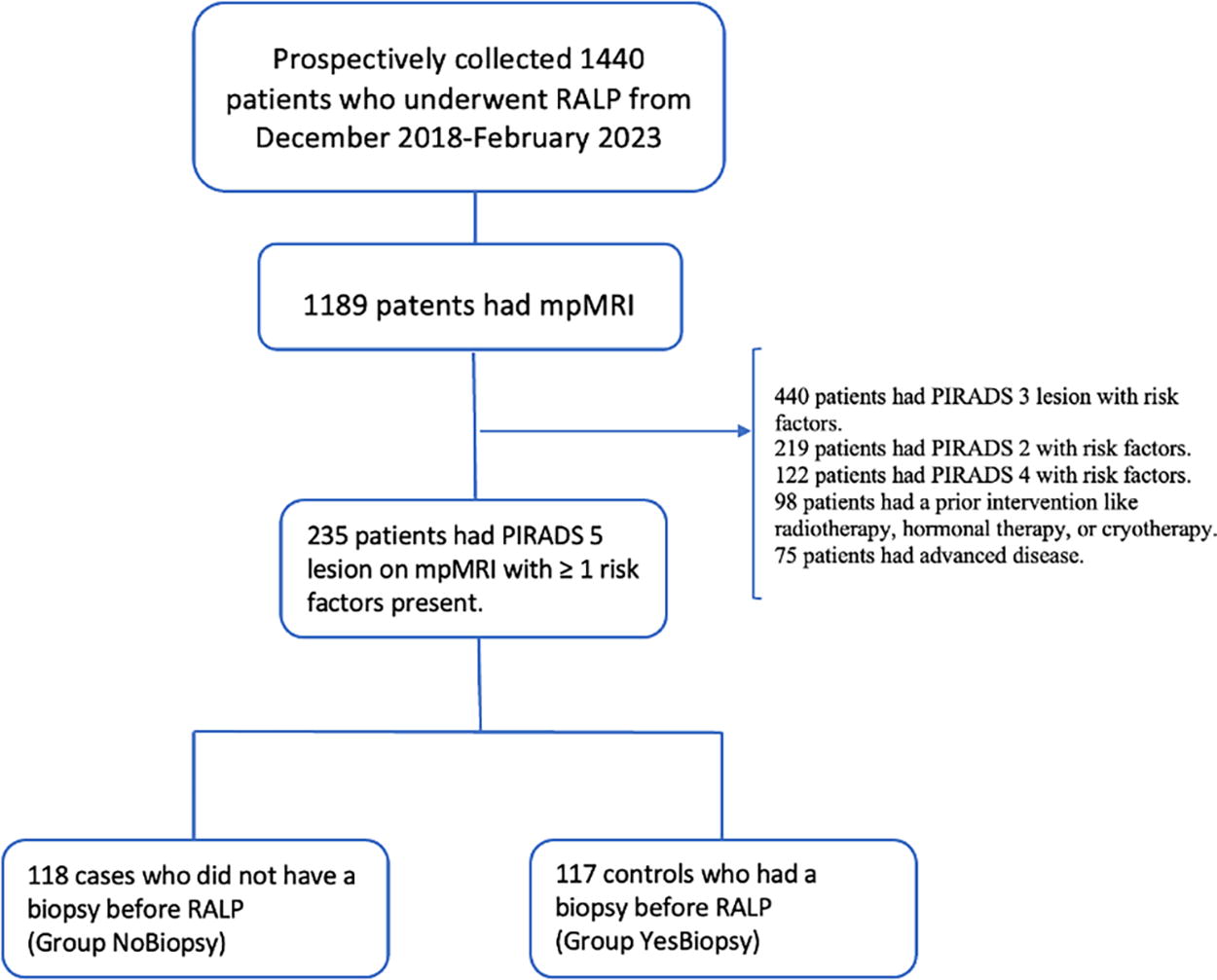
Flowchart Demonstrating the Study Cohort and Selection Criteria.
All men were counseled on the clinical significance of PIRADS 5 mpMRI lesions. Men in the NoBiopsy group underwent an informed consent process, including the risks, benefits, and alternatives of proceeding directly to surgery without prior biopsy. This included counseling on the possibility of a negative final pathology. Men in the YesBiopsy group underwent a similar informed consent process detailing the risks of prostate biopsy.
Preoperatively, the assessed parameters included age, DRE, PSA level, Biopsy Gleason Grade Group (GGG), MRI lesion zone (peripheral zone (PZ), transitional zone (TZ), or spanning both PZ and TZ), MRI lesion volume, MRI lesion location (apex, base, midgland, or spanning two or all of these regions), MRI apparent diffusion coefficient (ADC) size, family history, and smoking history. Postoperatively, we assessed console time, estimated blood loss (EBL), prostate volume, GGG, nerve sparing (NS) performed or not, presence of positive surgical margins (PSMs), extraprostatic extension (EPE), seminal vesicle invasion (SVI), lymphovascular invasion (LVI), and pathologic stage. All patients underwent follow-up assessments at 1, 3, 6, 9, and 12 months, during which their functional outcomes were documented at each clinic visit. The term “continent” was assigned to patients who did not require any pads, whereas any other degree of pad usage was categorized as experiencing differing levels of “incontinence.” Erectile function was evaluated based on the ability to have penetrative sex with or without PDE5 inhibitors.
Descriptive statistics was used to describe distribution, comparison of the baseline characteristics of both the groups, and frequency of data (Table 1). Continuous variables were analyzed using the independent t-test. Categorical data were compared using Chi-square or Fisher’s exact tests, whereas Mann–Whitney U tests were used for nonparametric variables (Tables 2 and 3). The hypothesis testing was two-sided and considered statistically significant at p-value < 0.05, 95% confidence interval. Univariate logistic regression analysis was conducted to unveil the odds ratios and corresponding p-values, elucidating the association of each variable with csPCa (Supplementary Table S1). A multinomial regression analysis, incorporating all significant variables identified in the univariable analysis, was performed to investigate the potential predictors associated with csPCa (Table 4). Intraoperative and postoperative outcomes were assessed for potential differences in oncologic and functional results. All analyses were performed using SPSS v.29.0.1.0 software (IBM, Chicago, IL, USA) and STATA version 14 (Stata Corp LLP, College Station, TX, USA) software.
Baseline Preoperative Characteristics of the Study Cohort
TZ, transitional zone; PZ, peripheral zone; GGG, gleason grade group; ADC, apparent diffusion coefficient; csPCa, clinically significant prostate cancer; PSA, prostate-specific antigen; MRI, magnetic resonance imaging; DRE, digital rectal examination.
Intraoperative and Postoperative Characteristics of the Study Cohort
EBL, estimated blood loss; NS, nerve sparing; EPE, extraprostatic extension; PNI, perineural invasion; SVI, seminal vesicle invasion; LVI, lymphovascular invasion; PSM, positive surgical margin; GGG, gleason grade group.
Functional Outcomes at 1, 3, 6, 9, and 12 Months Follow-Up Post-RALP
RALP, robot-assisted laparoscopic radical prostatectomy.
Multinomial Logistic Regression Analysis for the Study Cohort
DRE, digital rectal examination.
Results
The demographic and clinical characteristics of the study population are summarized in Table 1.
The mean age of patients in the YesBiopsy group was 66.74 ± 9.69 years, whereas those in the NoBiopsy group had a mean age of 63.84 ± 9.04 years. Sixty-nine (58.97%) patients in the YesBiopsy group had an abnormal DRE, compared with 88 (74.58%) patients in the NoBiopsy group. The majority of lesions were found in PZ on mpMRI, with 96 (82.05%) and 98 (83.05%) lesions in the YesBiopsy group and NoBiopsy group, respectively. The mean lesion volume on mpMRI was significantly higher in the YesBiopsy group (46.4 ± 70 cm3) compared with the NoBiopsy group (26.2 ± 30.3 cm3) (p = 0.005).
Console time was notably higher in YesBiopsy group compared with NoBiopsy (70 minutes vs. 60 minutes, p < 0.001). Prior biopsy was associated with significantly increased EBL compared with NoBiopsy patients (100 mL vs. 80 mL, p < 0.01). NS rate was higher in men with no prior biopsy (n = 115, 99%) compared with the control group (n = 108, 92%) (Table 2). No significant difference was observed in the prevalence of unilateral (p = 0.06) and bilateral NS (p = 0.5). Postoperative mean prostate volume was found to be significantly higher in the YesBiopsy group (64.2 ± 31.3 cm3) compared with the NoBiopsy group (49.7 ± 19.1 cm3). Notably, a larger proportion of patients in the NoBiopsy group had a postoperative GGG of 2 (47.46%) compared with the YesBiopsy group (33.33%). Figure 2 shows that 95% of men in the NoBiopsy group had csPCa on final pathology, whereas 5% had GGG1 disease. In the YesBiopsy group, 85% of men were found to have csPCa, whereas 15% had GGG1 disease.
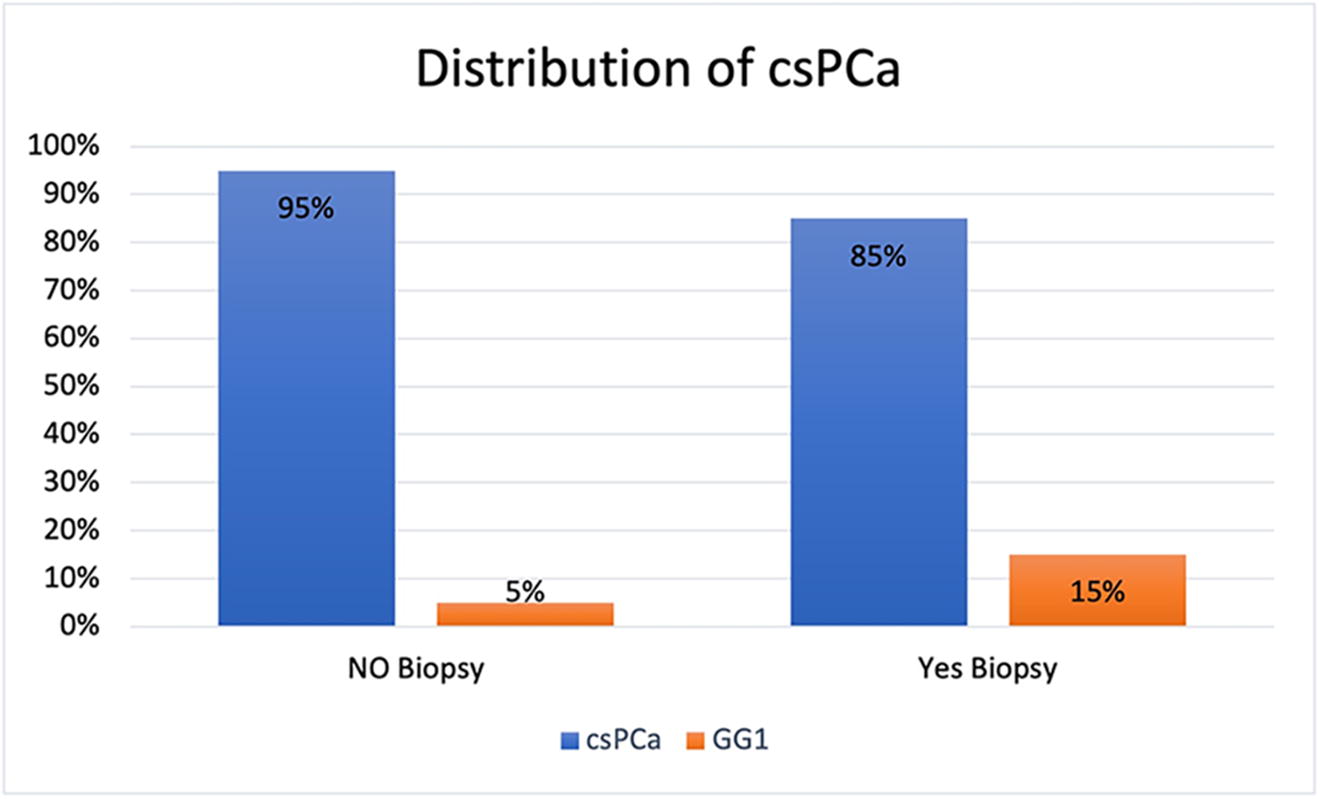
Graph Demonstrating the Distribution of csPCa in NoBiopsy Group (Cases) and YesBiopsy Group (Controls).
On univariate analysis, age, preoperative PSA, DRE, family history, biopsy status, and lesion location on MRI (lesion expanding to apex, base, and midgland) were significantly associated with csPCa (Supplementary Table S1). The multinomial regression model revealed that biopsy status holds a significant association with postoperative GGG1 compared to higher Gleason grades (Table 4). In GGG1, the coefficient for Biopsy status was 1.39. This indicates that the presence of a biopsy is associated with a substantial increase in the log odds of being GGG1 compared with GGG2. The p-value (0.014) suggests that this effect was statistically significant. The model’s overall significance was confirmed by a chi-squared test (chi-square coefficient of 97.60, with a corresponding p-value of <0.01), indicating that the predictors collectively influence the outcome. Predictors like age, preoperative PSA, DRE, family history, biopsy status, and lesion location on MRI overall did not have a significant association with postoperative GGG. However, preoperative PSA and DRE were found to be significant predictors for higher postoperative GGG, specifically for GGG5 disease (Table 4).
One month after treatment, continence was observed in 64% of patients in the NoBiopsy group, significantly surpassing the 54% observed in the YesBiopsy group (p < 0.01). Subsequently, at the 3-month (p < 0.01), 6-month (p < 0.01), 9-month, and 12-month intervals (p = 0.07), continence rates were 89%, 96%, 99%, and 100% in the NoBiopsy group, whereas in the YesBiopsy group, the rates were 75%, 88%, 96%, and 99%, respectively. Moreover, at the 1-month follow-up, 89% of cases in the NoBiopsy group were able to achieve erections, compared with 77% in the control group (p = 0.02) (Table 3). This was a sustained improvement through 12 months of follow-up.
Discussion
We found that biopsy status does not significantly predict csPCa in men with PIRADS 5 lesions on mpMRI. The collective impact of preoperative PSA, age, DRE findings, family history, and lesion location on mpMRI influences csPCa prediction.
Recent advancements in mpMRI technology have markedly enhanced the accuracy of PCa detection. A systematic review and meta-analysis demonstrated that PIRADS v2 exhibits a high positive predictive value (PPV) for csPCa detection. 4 The MRI-FIRST study, a prospective multicenter effort involving biopsy-naive patients, underscored the high sensitivity and specificity of mpMRI in detecting csPCa, emphasizing its potential to improve the diagnostic pathway for suspected PCa. 16 The landmark multi-institutional study (PROMIS trial) demonstrates that 18% more cases of csPCa might be detected with mpMRI compared with the standard pathway of transrectal ultrasound (TRUS) biopsy for all. 5 Hence, these recent studies have consistently shown that mpMRI has high sensitivity and specificity in detecting csPCa. 5,16,17
American Urological Association (AUA) guidelines recommend MRI-guided or systematic TRUS biopsy for biopsy-naive patients who have a suspicious lesion on MRI. 18 However, biopsy is an invasive procedure associated with potential complications, patient anxiety, and discomfort. It has been studied that TRUS biopsy results in periprostatic inflammation which may turn into hematoma and edema. 9 This prolongs the time to surgery by 4–6 weeks and can generate unnecessary anxiety for the patient. In addition, biopsy disrupts the tissue architecture causing fibrosis and obliterating the surgical planes of dissection, which makes fascial dissection more challenging. This has a direct effect on difficulty with neurovascular bundle (NVB) preservation and hence functional outcomes. 8,19 –21 In addition, 20% csPCa have been noted to be missed on biopsy as false negatives, which leads to delay in definite treatment and increases the aggressiveness of the cancer. 22 Our study found no significant association between biopsy status and csPCa (GGG ≥1), supporting these findings. The absence of missed csPCa cases in our study substantiates the higher log odds of a positive biopsy for GGG1 compared with GGG2.
A multicenter study conducted by the Uro-oncology Association correlates the use of mpMRI with PIRADS scoring in Turkish PCa patients to histopathologic factors observed in radical prostatectomy (RP) specimens. 23 Previous literature consistently indicates that higher PIRADS scores are associated with aggressive cancer, upstaging on final histopathology, and increased risk of biochemical recurrence. 17,23 –27 Our study highlights a crucial correlation between PIRADS 5 score on mpMRI and csPCa on final RP histopathology.
Numerous studies have investigated the potential of PSMA PET, mpMRI, and PSAD, both and in combination, for the diagnosis of PCa and the execution of RALP without a prior biopsy. 11,28 –30 The current body of literature lacks consensus because of conflicting and nonsignificant results, often influenced by inherent biases in study designs, absence of statistical power, randomization, and correlation to functional outcomes.
Meissner and associates and Sharma and colleagues observed that patients with mpMRI PIRADS ≥ 4 and elevated standard uptake value max on PSMA PET may potentially forego biopsy before RALP. 12,14 In the former case series, lesion-based analysis exhibited comparable sensitivity and PPV for mpMRI and PSMA PET scans in diagnosing csPCa. 12 Although PSMA PET augmented the sensitivity of mpMRI in diagnosing csPCa (83% vs. 88%), no beneficial effect was found in specificity, Negative Predictive Value (NPV), and PPV among both imaging modalities. 14 A systematic review and meta-analysis revealed that the pooled specificity of mpMRI was higher than PSMA PET for primary PCa (0.88 vs. 0.71, p = 0.0226). 13 A Prospective Multi-Center Study (PRIMARY) revealed comparable results with a higher NPV for the combination of PSMA PET and mpMRI compared with mpMRI alone. 30 However, it is important to note that the mpMRI findings in the study were influenced by nonstandardized readings, creating a potential bias in favor of PSMA PET. 30 This strategy has missed diagnosing 9.2% of csPCa cases in a recent retrospective single-center study. 15
In our study, csPCa was found on postoperative pathology in 95% of patients with PIRADS 5 lesions who directly underwent RALP and in 85% of men with PIRADS 5 lesions who underwent biopsy before RALP (Fig. 2). NS rate was higher in men with no prior biopsy compared with those who had a biopsy before RALP based on IOPAG scoring. 21 A greater proportion of men in the NoBiopsy group attained continence and erections at 1-, 3-, and 6 months following RALP compared with controls. To the best of our knowledge, this is the first study to demonstrate better functional outcomes in patients undergoing RALP without prior biopsy versus with a prior biopsy. There was no substantial difference among the comparative groups for rates of EPE, perineural invasion (PNI), SVI, and PSM. All men were continent and able to achieve erections at 1-year follow-up. This is attributed to the surgeon’s experience and learning curve that directly impacts the NS performed. This finding supports our practice of transitioning PIRADS 5 men to RALP and avoiding unnecessary stress caused by a prostate biopsy to the patient and health care resources. In addition, our findings suggest that DRE and preoperative PSA are potentially valuable predictors in determining the necessity of intervention for individuals with PIRADS 5 on mpMRI.
All mpMRI in our cohort were read according to PIRADS v2 and were read by a single senior Uro-radiologist with over 30 years of experience interpreting mpMRI of prostate with formal training at prostate MRI centers of excellence and MRI-PRO certification from Monash University, Australia. 7 This justifies the crucial factor of interindividual variation in PIRADS scoring of the lesions and increases the strength of our study and reliability of our findings. The overall model’s limited explanatory power suggests potential unexplored factors influencing postoperative Gleason grade in patients with PIRADS 5 findings. Consequently, further investigations with larger sample sizes and prospective studies are crucial to validate these results and provide comprehensive insights for optimizing patient management. Despite its retrospective nature and a relatively small sample size, the study holds value in establishing its real-life clinical relevance. Our single-surgeon and single-center cohort present limitations, emphasizing the need for future randomized controlled trials to validate the findings across a broader and more diverse population. That being said, the results presented herein represent a valuable addition to the urologic literature and can be used as a reference for further debate in the urologic oncology sphere.
Conclusion
Men with PIRADS 5 lesions on mpMRI represent a subset of patients with a high probability of csPCa. Performing RALP without antecedent biopsy in men with PIRADS 5 lesions results in higher csPCa detection rates while improving functional outcomes postoperatively. Further randomized controlled trials can validate this approach, assess its long-term oncologic outcomes, and refine patient selection criteria and guidelines.
Footnotes
Authors’ Contributions
All authors contributed substantially to the conception, design, acquisition, analysis, and interpretation of data. Each author approved the final version for publication and agrees to be accountable for the accuracy and integrity of the work in accordance with the standards set by the Journal of Endourology. S.R.: Conceptualization, validation, writing—original draft (equal), writing—review and editing (lead), visualization, and project administration. S.P.: Methodology, investigation, writing—original draft (lead), visualization, and project administration (equal). E.K.W.: visualization (lead) and data curation (equal). J.M.: Data curation (lead) and investigation (equal). J.P.: Software (lead), formal analysis (lead), and writing—review and editing (supporting). N.M.K.: Software (supporting) and formal analysis (supporting). C.W.: Software (lead) and resources (lead). S.R.: Conceptualization (lead), writing—review and editing (lead), visualization (lead), supervision (lead), and project administration (lead).
Author Disclosure Statement
Authors have no conflict of interest to declare.
Funding Information
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.