
Abstract
Purpose:
This case series describes the experiences and outcomes of multiple Australian surgeons performing robotic-assisted bladder diverticulectomy (RABD), highlighting the procedural effectiveness and safety, for both benign and malignant indications for diverticulectomy.
Methods:
Outcomes were analyzed from 13 experienced Australian urologists who performed RABD between 2016 and 2023. Retrospective analysis was performed on prospectively collected data, which included patient demographics, diverticulum characteristics, surgical approaches, and post-operative outcomes. Surgical techniques included the extravesical and intravesical approaches, with the focus on maintaining oncological principles in cases of malignancy.
Results:
A total of 28 patients underwent RABD, with the majority being male and a mean age of 63.9 years. All surgeons utilized a four-port transperitoneal approach and opted for the extravesical dissection of the diverticular neck; one case utilized both an extravesical and a trans-diverticular approach. Functional outcomes demonstrated symptomatic resolution in patients with nonmalignant diverticula, whereas oncological outcomes indicated clear margins in 90% of malignant cases. The average length of the procedure was 106 minutes, with minimal blood loss and a mean hospital stay of 2.67 days. Early complications occurred in 14% with the majority Clavien–Dindo grade II.
Conclusion:
Robotic bladder diverticulectomy, predominantly via the transperitoneal extravesical approach, has emerged as a safe, effective, and reliable surgical intervention for both malignant and nonmalignant bladder diverticula. The consistent surgical approach and excellent outcomes demonstrated in this case series reinforce the procedure’s potential as a safe option, even in the setting of malignancy within a diverticulum.
Introduction
Bladder diverticula (BD), characterized by sac-like outgrowths from the bladder wall, are primarily caused by bladder outlet obstruction or a neurogenic bladder and can be exacerbated by recurrent infections. 1,2 These protrusions, although not invariably symptomatic, can escalate in size, leading to a spectrum of complications ranging from urinary tract infections (UTI) to bladder stones and urinary retention. 3,4 These outpouchings, while mostly benign, can undergo neoplastic changes in up to 10% of cases. 5 For those manifesting symptoms or harboring malignancies, bladder diverticulectomy stands as the definitive therapeutic intervention. 3,6 –8
The evolution of surgical management for BD has seen a shift from traditional open surgery and laparoscopy to the increasing adoption of robotic-assisted techniques. 9 The emergence of robotic technology offers the benefits of minimal invasiveness while retaining surgical precision and ergonomics. 9 Given its infrequent occurrence, most urologists find themselves navigating this surgical procedure only sporadically, perhaps once every several years. This, coupled with the nascent emergence and progressive adoption of robotic surgery, culminates in a diverse array of individual experiences with RABD.
The literature illuminates this diversity, unveiling an array of operative techniques and approaches. 4,7,10 With no standardized technique, variations include extravesicular, transvesicular, and transdiverticular approaches. 2,6,7 Furthermore, when malignancy is localized within the bladder diverticula, it necessitates nuanced surgical methodologies. These are vital to uphold the oncological principles of resection and forestall any malignancy spillage into the peritoneal cavity.
Considering this varied landscape, our case series aims to report our experience and surgical outcomes from numerous Australian surgeons engaged in RABD. By sharing these consolidated insights, we aim to propel its broader application within the urological community, thereby elevating the standard of care and ensuring enhanced outcomes for forthcoming patients.
Methods
Data collection
We conducted a retrospective study, gathering data from 13 experienced Australian urologists encompassing five major hospitals who had performed RABD between 2016 and 2023. All urologists had ten or more years of robotic surgical experience. The data was de-identified and systematically recorded in a predefined collection sheet.
All procedures were performed under general anesthesia using the four-arm da Vinci Xi robotic platform (Intuitive Surgical, Sunnyvale, CA, USA). Given the retrospective nature of our audit, we did not contact patients, and no additional visits were required.
Data collected included anonymized patient details, clinical history, diverticulum characteristics, preoperative assessments, surgical technique, and post-operative outcomes. Specific details included age, BMI, prior surgeries, diverticulum size and location, preoperative symptom scores, oncological history, surgical methods, concurrent procedures, hospitalization duration, and complications. Operative techniques were recorded from operative reports along with qualitative feedback from individual surgeons.
Outcomes were categorized and reported under two main dimensions: functional and oncological. Under functional outcomes, we evaluated the proportion of patients manifesting symptomatic resolution 6 weeks post-op, the decrement in post-void residual volumes, and the attenuation in the International Prostate Symptom Score. 11 In the oncological domain, our principal metric encompassed surgical margin status.
Surgical Approaches
Extravesical approach
Suitable for moderate to large diverticula near the bladder dome or lateral wall, the extravesical approach involves minimal bladder mobilization. After establishing pneumoperitoneum, the diverticulum’s peritoneal covering is scored, and the bladder may be retrogradely filled for BD localization. The diverticulum is then mobilized and excised. Closure is achieved with two layers of absorbable sutures.
Transvesical approach
Preferable for posterior or posterolateral diverticula close to a ureteral orifice. The space of Retzius is developed by dividing the median and medial umbilical ligaments after incising the peritoneal bladder covering. An anterior vertical cystotomy allows for the insertion of ureteral stents or catheters and facilitates diverticular neck identification and excision through combined intra- and extravesical dissection. This approach also allows for concurrent procedures like bladder stone evacuation or robot-assisted simple prostatectomy.
Trans-Diverticular approach
Optimal for large benign diverticula, this approach involves entering the diverticulum sac and performing an extravesical dissection after disconnecting it from the bladder.
For all approaches concurrent cystoscopy can assist in identifying the diverticular neck. A leak test is conducted to confirm a watertight closure, and a pelvic drain is placed prior to undocking the robot. Postoperative management includes cystogram prior to catheter removal. In cases of diverticular urothelial carcinoma (UC), surveillance through cytology, imaging, and cystoscopy is conducted to monitor for recurrent disease.
Ethics
Ethical approval was attained from St Vincent’s Hospital Human Research Ethics Committee-2021/ETH11360.
Statistical Analysis
Statistical analyses in this study constituted only descriptive statistics. Objective outcomes such as post-void residuals were compared with paired sample t-tests. Collected data were analyzed using SPSS version 21.0 (IBM Corp., Armonk, NT, USA). All p values reported are two-sided, and statistical significance was set to p < 0.05.
Results
Twenty-eight patients underwent RABD, ten for diverticula containing malignancy with the remaining for symptomatic diverticula. The majority were male (n = 26), with only 2 females. Mean age was 63.9 years with a wide range of 21 to 87 years. Patient demographics are tabulated (Table 1). Clinical indications were categorized as malignant (n = 10) or nonmalignant (n = 18). Indications in the nonmalignant group included symptomatic lower urinary tract symptoms (n = 13), recurrent UTI (n = 4), bladder stone (n = 1), and congenital conditions (n = 1). The majority of patients (71%) had not undergone previous intrabdominal surgery, while most patients had previous bladder outlet operations (71%).
Patient Demographics
ASA, American Society of Anesthesiologists Classification; BMI, body mass index; LUTS, Lower urinary tract symptoms.
All 13 surgeons utilized a four-port transperitoneal approach and opted for the extravesical dissection of the diverticular neck (Table 2). One surgeon utilized the extra- and trans-diverticular approach. Concurrent flexible and/or rigid cystoscopy was employed for intravesical illumination and visualization in 79% of all cases, 77% of nonmalignant cases, and 80% of malignant cases. Rigid cystoscopy was preferred in cases where concurrent stenting or instrumentation occurred; otherwise, flexible cystoscopy was used only for concurrent intra- and extravesical visualization. Concurrent procedures included placement of ureteral stent (50%), ureteral re-implantation (11%), radical prostatectomy (21%), transperitoneal vasectomy (4%), prostate enucleation (4%), laser bladder neck incision (4%), and radical lymph node dissection (4%). The mean (SD) number of diverticula resected was 1.81 (0.87) with the average diameter of the largest diverticulum being 74 mm, 91 mm in nonmalignant, and 46 mm in malignant. The mean surgery duration was 106 minutes with mean estimated blood loss of 85 mL and mean hospital stay of 2.57 days. There were no conversions to open surgery.
Operative Metrics
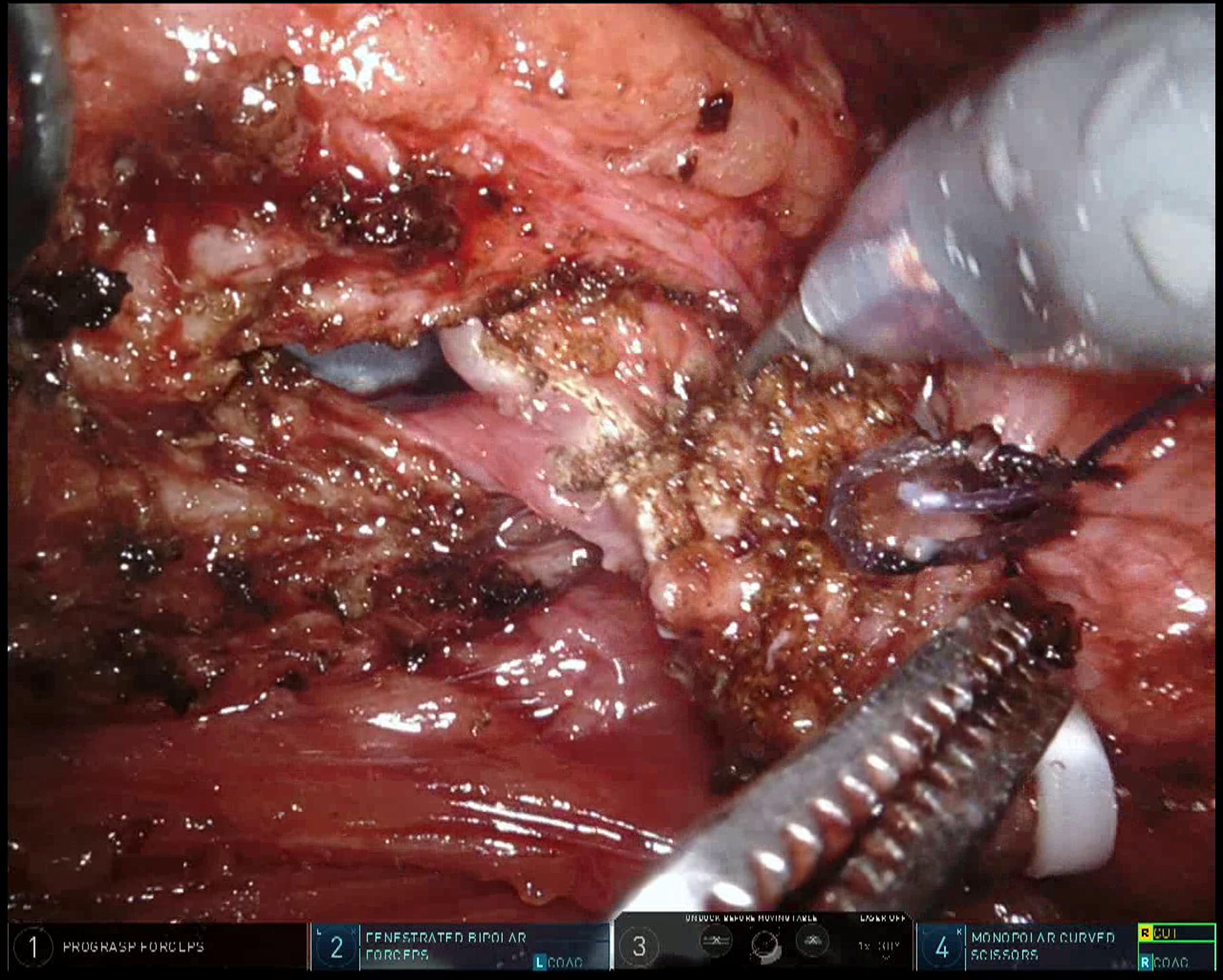
Intraoperative techniques for maintaining oncological principles for malignant diverticula varied (Table 3). These techniques included the use of rigid and flexible cystoscopy to assist with identification of the diverticulum neck (Figs. 1 and 2), the instillation of intraoperative intravesical mitomycin C before dissection of the diverticulum, application of a laparoscopic stapler, ties, or clips across the neck of the diverticulum (Fig. 5), emptying the bladder via cystoscopy and then insufflating it with air to avoid tumor spillage (Fig. 3), and finally, one surgeon utilized Rumel tourniquets to both ureters (preventing reflux of malignant urine).
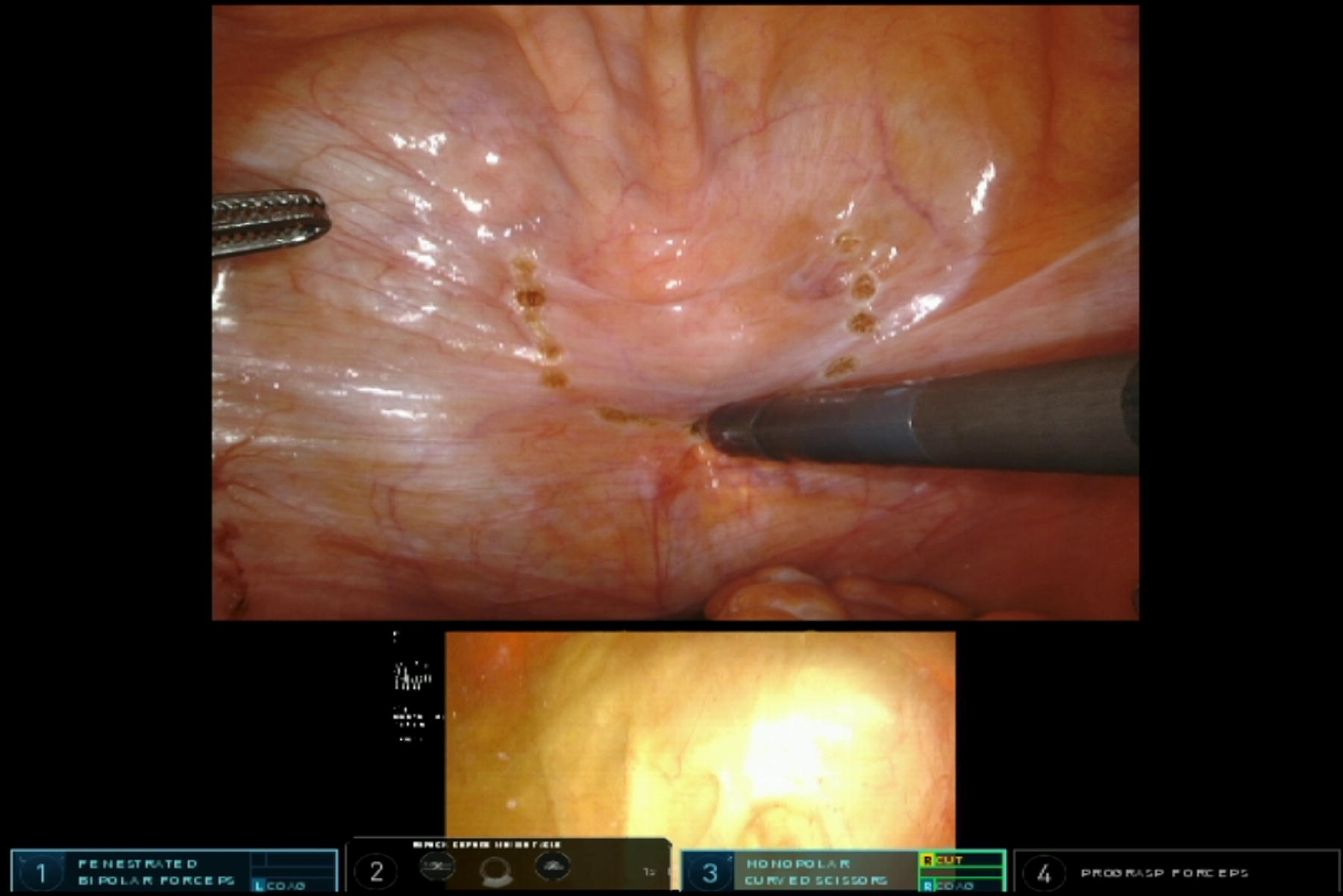
Concurrent flexible cystoscopy facilitating easy identification of diverticulum by transillumination and marked by diathermy.
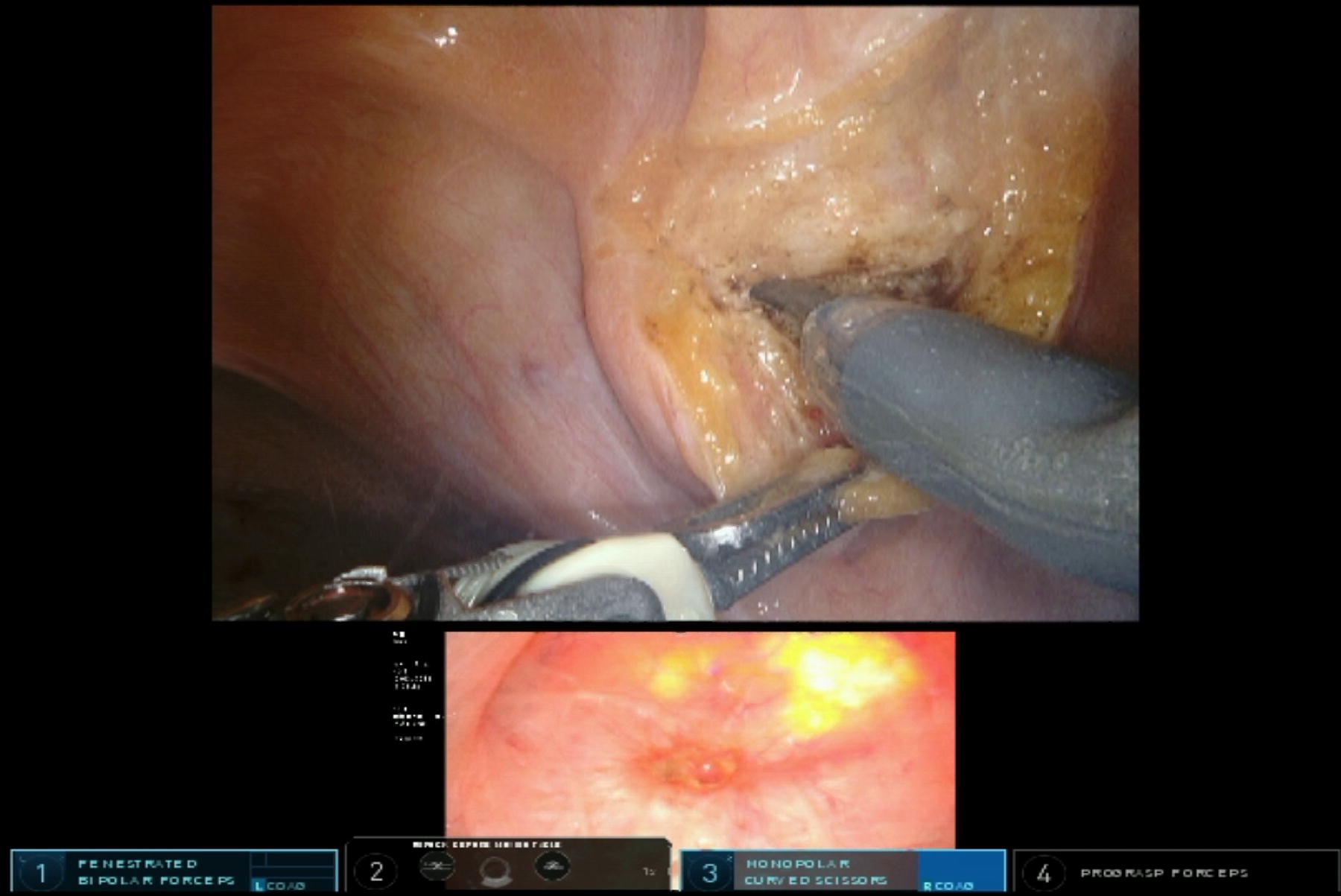
Concurrent flexible cystoscopy view during dissection of malignant lesion.
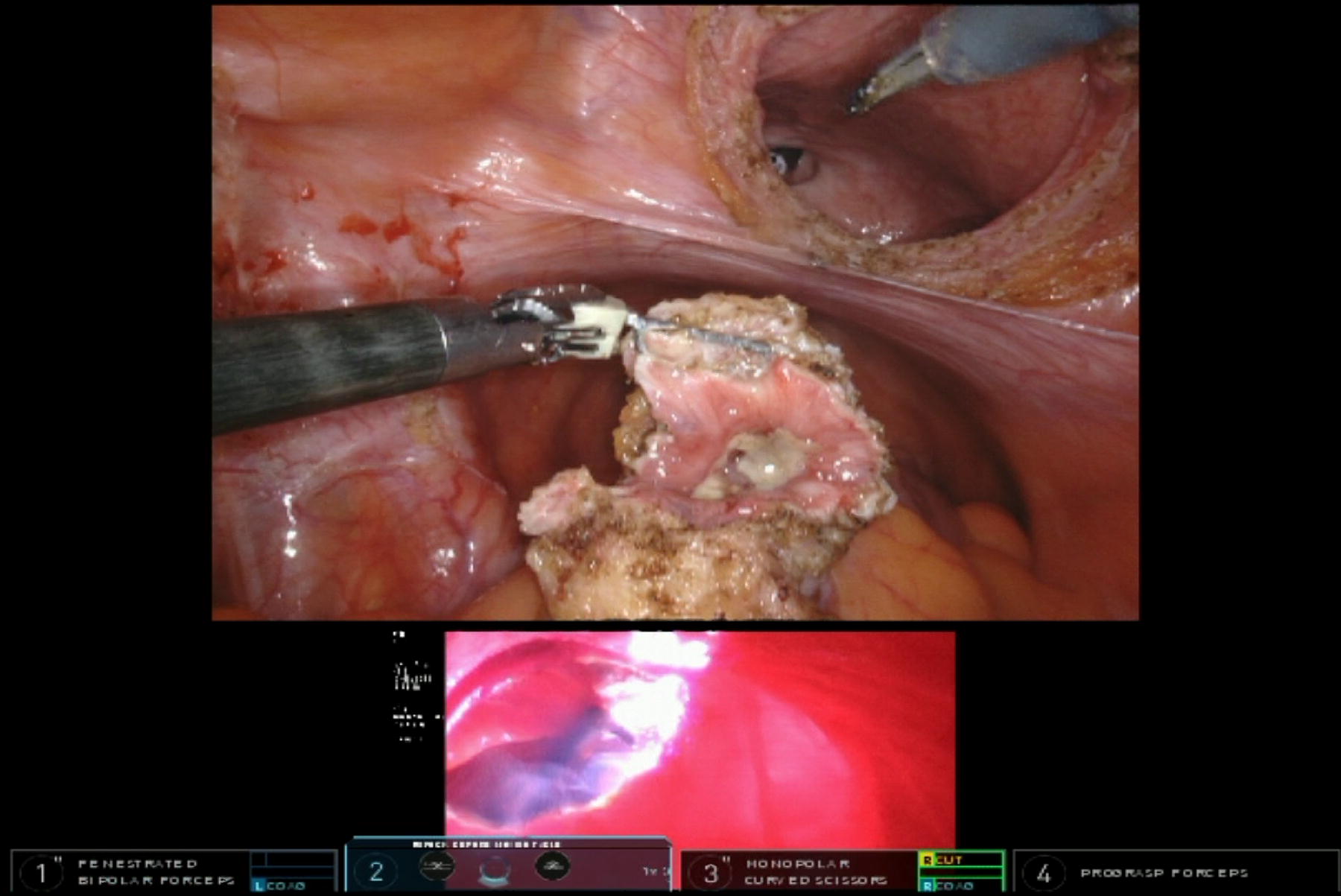
Bladder emptied of urine, insufflated with carbon dioxide, dissection of malignant lesion completed, cystotomy on view with flexible cystoscopy at bladder neck, lesion placed in endocatch immediately.
Malignancy Cases
There were no intraoperative complications. Two patients experienced a posterior post-operative leak, while the average length of catheterization was 10.36 days. Four patients experienced early complications (14%): postoperative ileus (Clavien–Dindo I), urinary retention and infection (Clavien–Dindo II), a lymphocele requiring interventional radiology drainage under local anesthesia (Clavien–Dindo IIIa), and pulmonary embolus treated by anticoagulation (Clavien–Dindo IVa).
All patients except for one with urethral strictures experienced subjective symptomatic resolution of their symptomatic diverticula at 30 days post-op (Table 4). Clear margins were achieved in all but one patient (Table 5). There was a reduction in the post-operative post-void residual (p = 0.0047) for patients with symptomatic diverticula.
Functional Metrics
Oncological Outcomes
HG, High grade T3a, High grade T2a ect; CIS, Carcinoma in situ; SCC, Squamous cell carcinoma.
Discussion
This Australian case series reports the techniques, peri-operative outcomes as well as the short-term functional and oncologic results of 28 patients who underwent RABD for malignant and nonmalignant bladder diverticulum. These results demonstrate that RABD is effective, reliable, and safe across a number of different indications, including the management of UC within diverticula. Despite being similar in size to other RABD series, our study is unique for its Australian perspective, representing the most extensive collection of independent urologists performing RABD, the largest group of malignant cases, and largest transperitoneal extravesical series to our knowledge in the literature.
Patient demographics including sex, age, BMI, and ASA were comparable with other RABD reports. 3,4,6,7 Indications for RABD were also consistent with the literature, encompassing symptomatic high post-void residuals, bladder stones, recurrent UTIs, malignancy, and congenital diverticulum. Mean operative time (102 minutes) was slightly shorter than other series results, including a transvesical series (140 minutes), Giannarini’s extravesical series (126 minutes), Liu and colleagues mixed series (139 minutes), and Davidiuk’s mixed series (extravesical 228 minutes, transvesical 149 minutes). 3,4,6,7 Estimated blood loss was comparable to other recorded results at 85 mL.
Intra-operative complication rates remained low with no cases requiring conversion to open surgery. Four patients (14.3%) had early complications including a pulmonary embolism, UTI, post-op ileus, and lymphocele drainage, with these rates consistent with existing literature (12.5–15%). 4,6,7 The duration of stay (2.57 days) and catheterization (10.36 days) aligned with other studies (2–6 days, 2–11 days). 3,4,6,7
Functional outcomes post-RABD have been highlighted in other studies with subjective improvements in voiding function identified through various symptom scores. 12 Our findings further emphasize this, as all patients with symptomatic diverticula reported subjective symptomatic improvement 30 days post-operatively, excluding one patient with known urethral strictures, underscoring the effectiveness of the RABD procedure.
All surgeons consistently used a four-port transperitoneal extravesical approach for the operative technique, with unanimous preference for the extravesical method. This uniformity suggests the standardization of RABD on the east coast of Australia. One surgeon chose the trans-diverticular approach for a large diverticulum with extravesical access challenges. However, in other cases, the same surgeon opted for the extra-vesical method. The prevalent use of concurrent cystoscopy in most cases, especially in malignancy, highlights its utility in improving visualization and evaluating the diverticular neck during the operation. Transvesical illumination with marking by extravesicular diathermy was the predominant technique. Concurrent non-related procedures occurred in 50% of all cases (80% of nonmalignant) without complication. While this has been described well in other reports, our data further demonstrates the safety of concomitant procedures including four cases of robotic-assisted radical prostatectomy.
Within the literature, there are varying descriptions of the optimal technique for RABD. A total of 122 cases have been documented, with single case series ranging to 23 patients. 3,9 Although Develtere et al. remain the largest transvesical series, our extravesical series evenly contrasts their results. 3 Operative time for diverticulectomy remained similar (106 minutes vs. 123 minutes), but estimated blood loss was higher (85 mL vs. 250 mL). 3 Impressively catheter removal rates were much shorter in the transvesical series (2 days vs. 10.36 days) with the authors crediting the utilization of a barbed running suture for watertight closure of the cystotomy and diverticular defect. 3 Furthermore, only 39% of their cases utilized cystography post-op, while the standard across all 11 surgeons was for a day 7 cystogram before removal of catheter. 3 One patient experienced a leak in the transvesicle study, whereas two posterior leaks occurred in our slightly larger sample (28 patients). 3 Running barbed sutures for bladder closure were standard across all cases in our series. The transvesical series suggests that the Australian catheterization duration practice might be overly cautious. The results between the two approaches are remarkably similar and should not be dismissed as both techniques demonstrated safety, reliability, and good patient outcomes. Despite this, the authors’ recommendations remain in favor of extravesical approach, especially in the setting of malignancy.
This case series, with ten patients, is the largest collection of malignant cases reported in literature. In this population, bladder diverticulectomy also doubles as a partial cystectomy acknowledging that T1 disease within the diverticulum is often considered a T2. Eventually, a portion of this population will go on to have a cystoprostatectomy as recommended by current guidelines. 8 Despite the ubiquity of the transperitoneal, extravesical approach across all 13 surgeons, the management of malignant diverticula included more variation in techniques. The rarity of malignancy within the diverticulum resulted in five of nine urologists each having their own unique variation on management. All referencing the risk of seeding from malignant diverticulum, variations aimed to minimize the risk of urine spilling into the peritoneum or ascending the ureters. Most techniques involved concurrent cystoscopy, the emptying of the bladder followed by air insufflation via flexible cystoscopy (Figs. 1, 2, and 3). Rumell tourniquettes were also used to clamp the ureters, with bilateral stents placed at the end of the procedure. Other solutions involved positioning an endocatch bag below the specimen before immediate removal of diverticulum into bag, stapling of diverticular neck, and intravesical mitomycin C before clamping the diverticular neck and subsequent resection (Figs. 4, 5, and 6). From all these techniques, oncological outcomes from these cases were good, with only one specimen found to have separate CIS disease at a margin. One patient with high-grade T3 disease in the diverticulum went on to have metastatic disease.
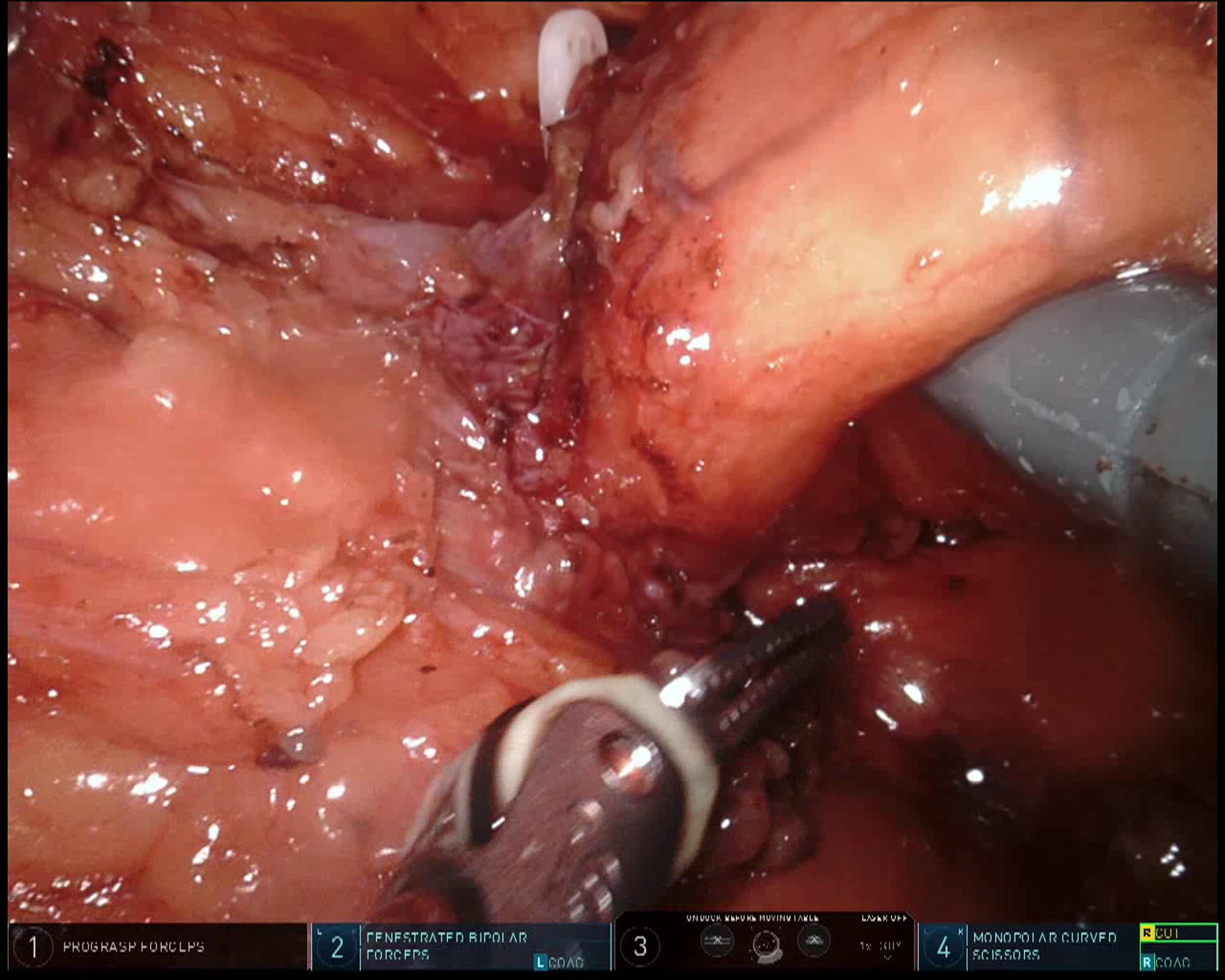
Extravesical approach to diverticular neck in malignant lesion.
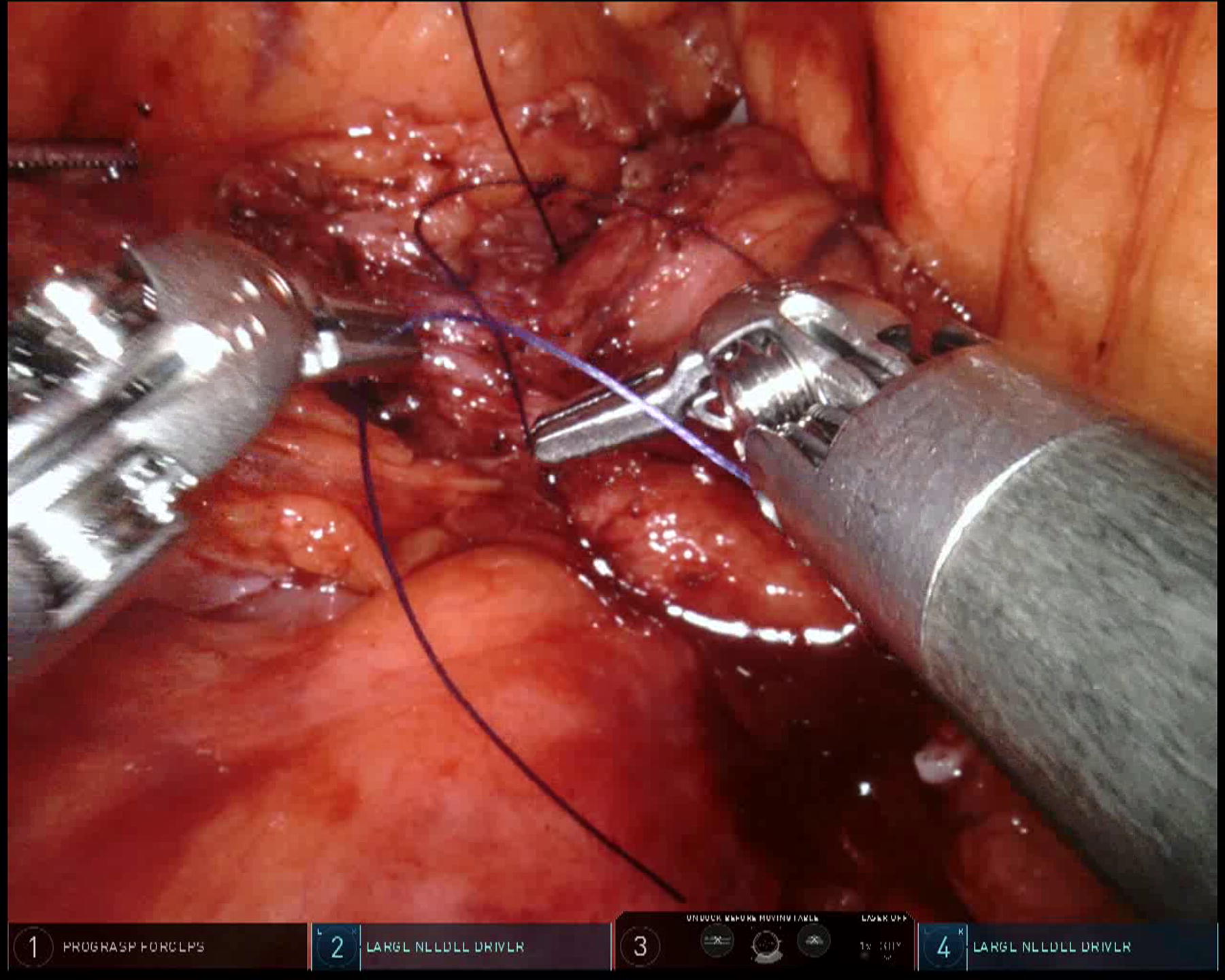
Vicryl tie to diverticular neck to ensure no malignant urine spillage.
Dissection of malignant diverticular neck with multiple ties to enclose malignant urine.
This study highlights the safety, efficacy, and applicability of RABD across a variety of indications. The consistency in surgical approach, coupled with promising clinical outcomes, underscores its potential as a standardized procedure for bladder diverticula. This study is limited in applicability due to its retrospective nature and limited follow-up length. It is important to note that the variability in technique as well as the frequency and variety of concurrent procedures performed in this series do represent a significant limitation. These concurrent procedures carry potential morbidity and did impact the outcomes of certain cases. Prospective and larger multi-center studies would be beneficial to confirm these findings and further investigate the safety of RABD and its benefits, such as improved urinary symptoms and oncological control.
Conclusion
RABD is an increasingly popular technique due to its minimally invasive approach, improved visualization, and precise instrumentation. Among the participating urologists, the transperitoneal, extravesical approach was ubiquitous and strongly advocated. The management of malignant diverticula included more variation in techniques to maintain oncological principles. RABD remains safe, with excellent operative metrics and good patient outcomes.
Footnotes
Acknowledgment
Figures courtesy of Dr Scot Leslie, Dr Bill Papadopoulas, and Dr Norbert Douek.
Authors’ Contributions
D.G.: Protocol/project development, data collection, data analysis, and article writing/editing. R.S.: Data collection, and article writing/editing. G.M.: Protocol/project development. C.P.: Protocol/project development. A.H.: — Data collection. N.A.: Data collection. M.A.: Data collection. M.E.: Data collection. R.T.: Data collection. N.D.: Data collection. B.P.: Data collection, P.R.: Data collection. K.R.: Data collection. T.N.: Data collection. J.T.: Data collection. P.A.: Data collection. P.J-T.: Article editing. S.L.: Protocol/project development, article editing, and supervision.
Author Disclosure Statement
The authors have no relevant financial or non-financial interests to disclose.
The authors have no competing interests to declare that are relevant to the content of this article.
Funding Information
No funding was received to assist with the preparation of this article.