
Abstract
Vesico-vaginal fistulae require complex reconstructions and robotic assistance can be beneficial in obtaining successful outcomes. In this video, we demonstrate two of our techniques of vesicle-vaginal fistula repair, one with transverse cystotomy and other with vertical cystotomy, along with salient steps of the procedure. The indication, preparation, instrumentation, and surgical steps are also discussed along with a review of available literature.
Indications
Large complex fistulae preferably supra-trigonal in location. Deep narrow vagina not conducible for trans-vaginal repairs. Previously failed trans-vaginal approach. Need for adjunct procedures (urinary bladder augmentation, ureteral reimplants). Associated genitourinary fistulas (ureterovaginal fistulas/uterovaginal fistulas).
Preparation
Preoperative counselling Discussion on success rates. Alternative options. Expected post operative course and need for prolonged catheterization. Complications. Discussion on postoperative voiding and sexual dysfunction. Correction of malnutrition if present. Local estrogen use in case of postmenopausal women to improve tissue integrity. Menstruation—some experts suggest avoiding performing repairs during menstrual periods owing to increased tissue vascularity (not a standard recommendation). Local hygiene and care considering the possibility of urinary dermatitis of local tissues. Part preparation—nipples to mid-thigh. Antibiotic prophylaxis—30 to 60 minutes prior to surgical incision. Bowel preparation—not recommended. Cystoscopic and vaginoscopic evaluation—bilateral ureteric catheterization and catheterisation of the fistula for intra-operative guidance and identification. Placement of sponge in the vagina—maintains pneumoperitoneum and can be utilized for intraoperative localization of the fistula site.
.
INSTRUMENTS (Da Vinci Xi System)
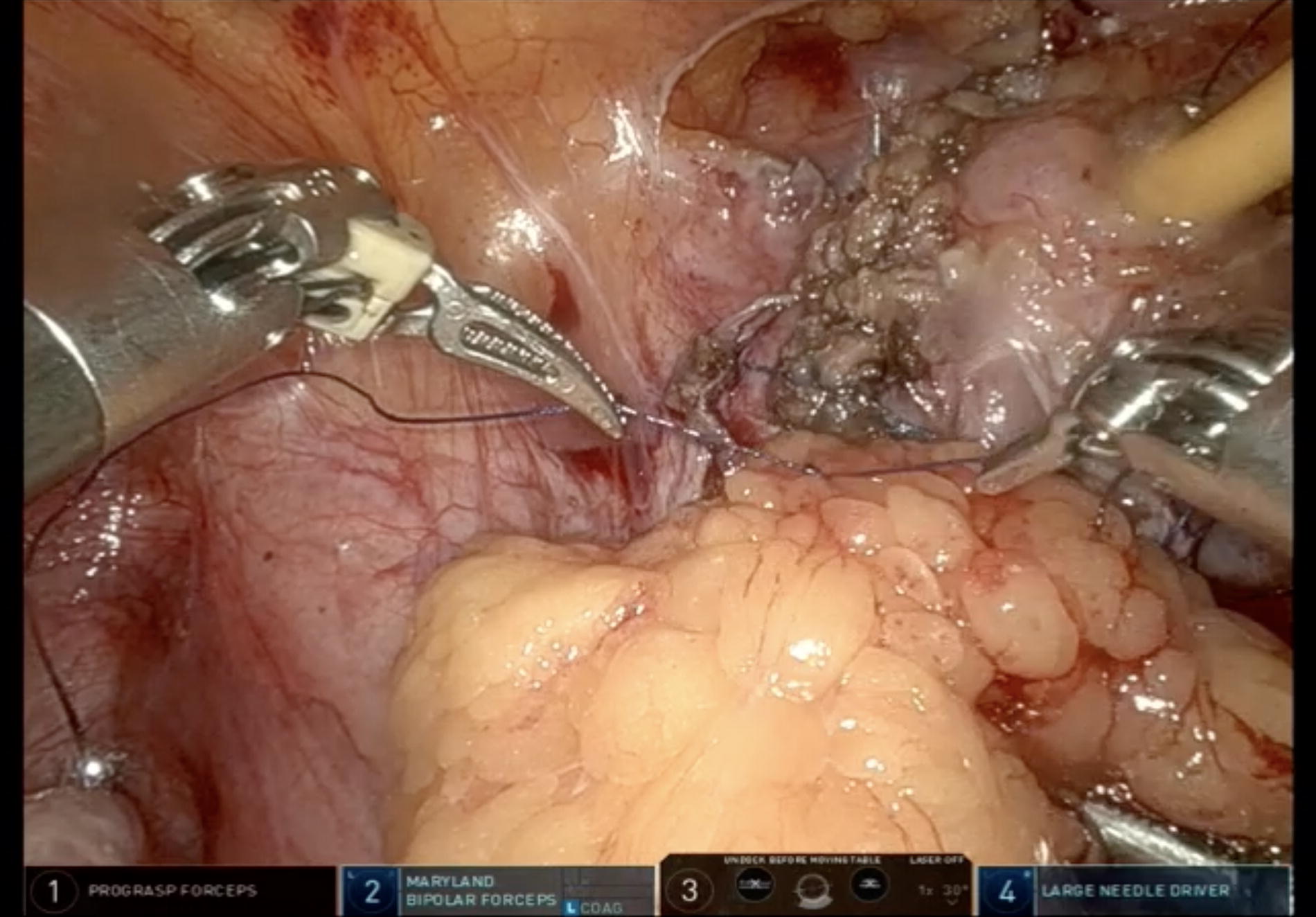
Endo wrist Robotic Instruments: 30° Endoscopic Camera. Hot Shears/Monopolar curved scissors. Fenestrated/Maryland bipolar forceps. Large needle driver. Pro Grasp forceps (optional). Assistant Instruments Laparoscopic Maryland forceps. Laparoscopic needle holder. Laparoscopic scissors. Laparoscopic suction catheter. Energy sources—Monopolar and Bipolar Electrocautery Sutures V-Loc 2’0 & 3’0 sutures—Vaginal and bladder wall closure. Vicryl 2’0 & 3’0 sutures (Polyglycolic acid)—Interposition tissue anchoring. Foleys catheter—14/16 Fr.
Positioning
The patient is placed supine on the operating table with anatomic pillows to protect the head and shoulders in addition to the adequate padding at the pressure points. To prevent hypothermia, elastic cotton drapes are wrapped around the extremities over the anti-thrombotic elastic socks and a special warm air blanket covers the patient’s face and chest. The patient is placed in lithotomy with the legs placed in special boots (Allen’s stirrups) that facilitate the active legs positioning during the procedure. Differential positioning during the procedure: Cystoscopy—lithotomy position with the horizontal operating table. Adhesiolysis to tissue interposition—lithotomy position with steep trendelenburg positioning (10–30°) (keeps the Douglas pouch free of sigmoid colon and small intestine, providing complete access to the vagina and bladder). During tissue interposition (optional)—Reduced Lithotomy with an almost horizontal (0 to 5 degrees) operating table (facilitates tension free fixation of the omentum) with the hips and knees only slightly flexed to reduce the distance between the root of mesentery and os pubis facilitating tension free approximation of the omentum to the fistula site.
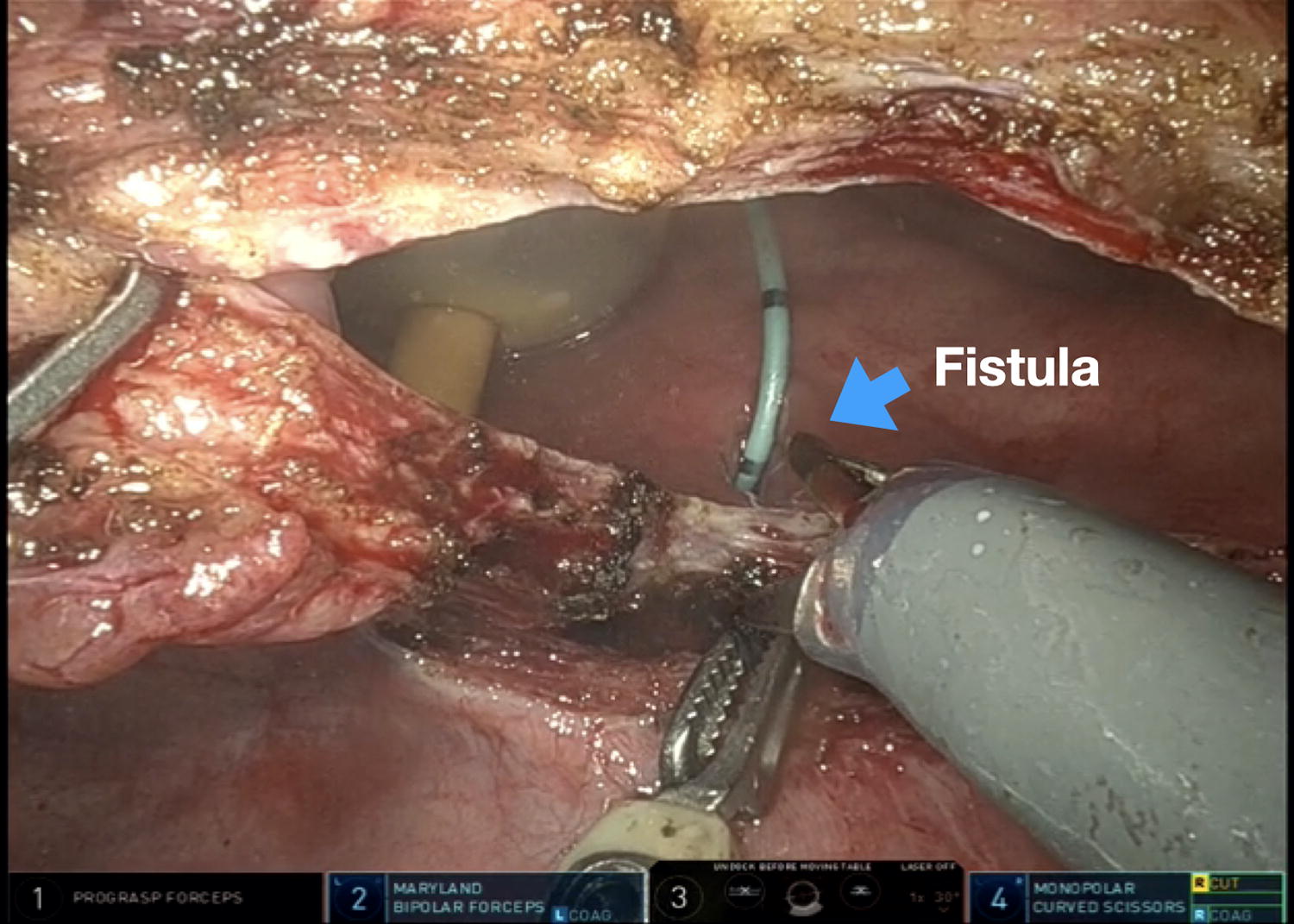
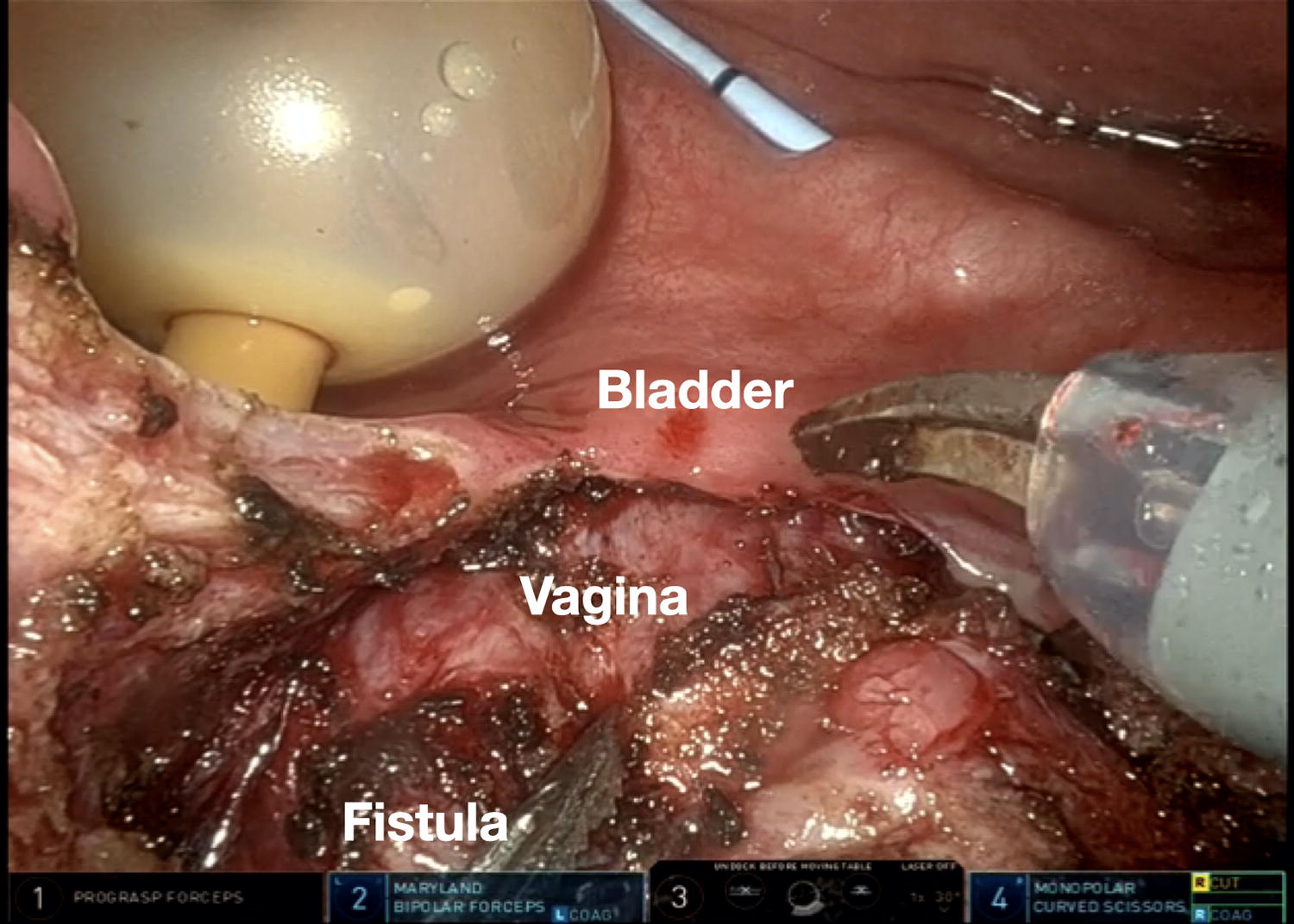
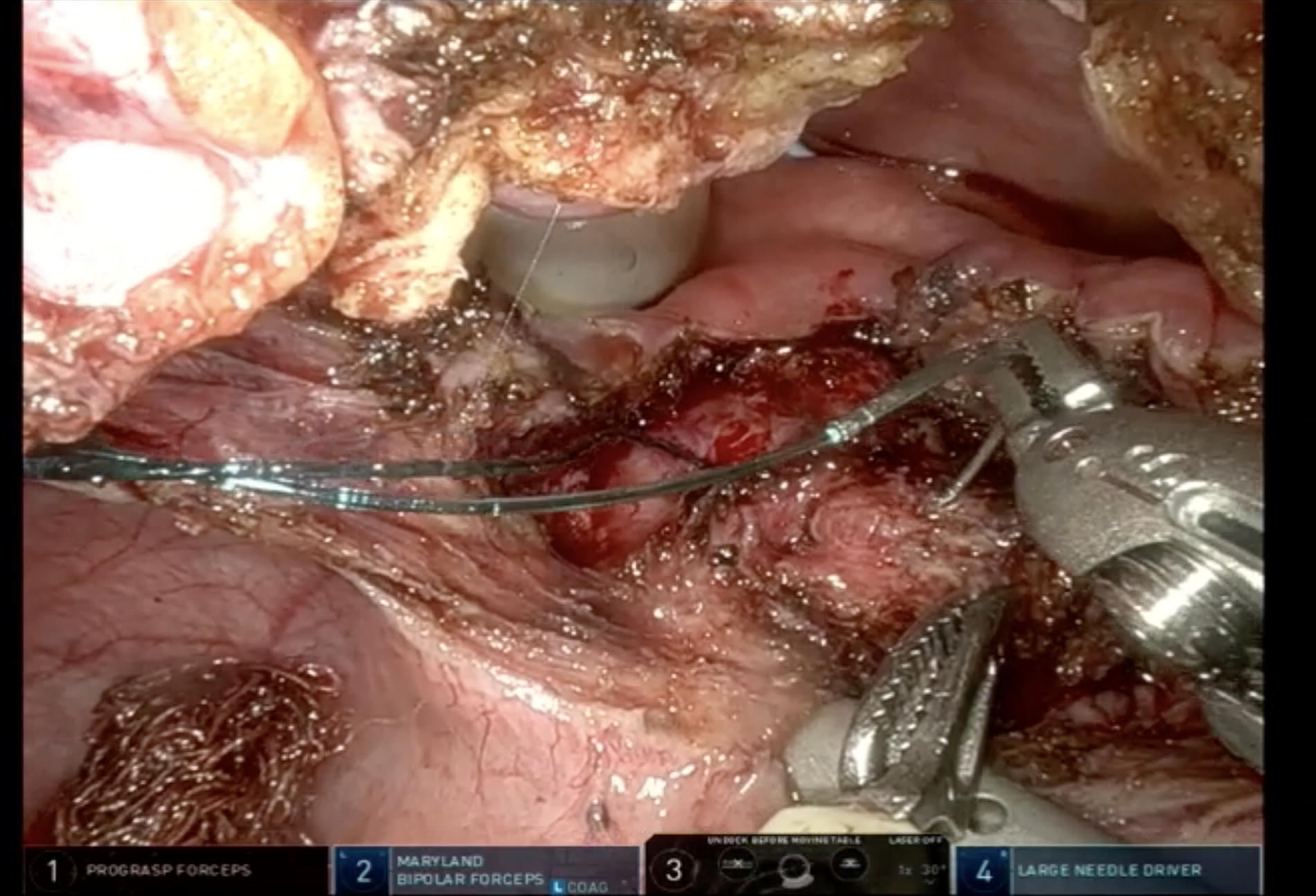
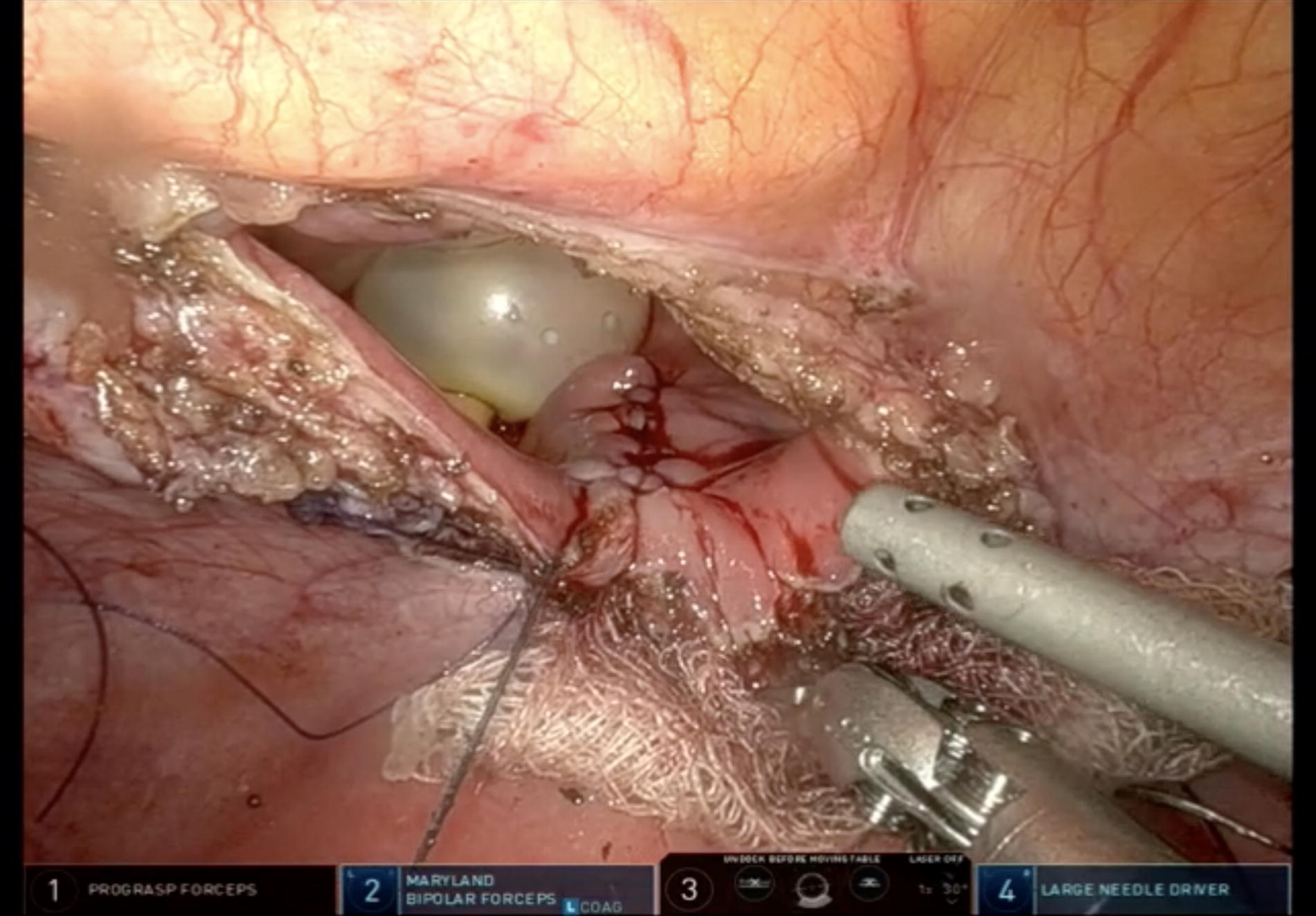
PORT POSITION: Camera Port (8 mm)—2 to 3 cm Above the umbilicus in the midline/just left of the midline based on the height of the patient. 2nd 8 mm and 3rd 8mm ports—At the level of the umbilicus in the right and left para-rectal line. 4th Arm port (8 mm)—3 to 5 cm above the left iliac crest. Assistant port (5/10/12 mm)—Symmetric to the 4th arm port on the right side. Peritoneoscopy & Adhesiolysis—General evaluation of status of the pelvis with adhesiolysis to clear the pelvis off the small bowel adhered at the operative site to enable localisation of fistula site. Localisation of fistula site—By manipulation of the ureteric catheter placed through the fistula site or the vaginal sponge. These facilities to create a smaller cystotomy at the site of tentative fistula as compared with the traditional complete bi-valving of the bladder. Alternative Technique—Diaphanoscopy (focusing the light of the cystoscope on the fistula, which becomes clearly visible laparoscopically through the bladder after switching off the robotic camera light). Cystotomy with fistula identification—Either a transverse cystotomy or a vertical cystotomy is made in the posterior wall at the site of tentative fistula (Fig. 1). Separation and mobilisation of the bladder from the vagina—The bladder wall is fully mobilized off the anterior aspect of the vagina. The pre-placed ureteric catheters are helpful in identifying the ureteric orifices and preventing inadvertent injury to the ureters. Further mobilization and disconnection of the bladder from the anterior vaginal wall allows a tension-free closure. (Fig. 2). Vaginal Closure with V-loc 3’0 sutures and closure integrity is checked by visualization of maintenance of the pressure of pneumoperitoneum after removal of the vaginal tamponade (a rough test to check the adequacy and the water tightness of vaginal closure) (Fig. 3). Bladder closure with V-loc 2’0 running sutures and the integrity of the closure is checked by inflating the bladder with saline to 150 or 200 cc capacity. (Fig. 4). Placement of a supra-pubic catheter (optional)—preferably via a separate incision made in the dome of the bladder. The supra-pubic catheter is then fixed with a purse string suture. Omental interposition with fixation of the pedicle to the anterior vaginal wall between the suture lines of bladder and vagina. Alternatively, the apendices epiploicae can also be utilised if omentum is not accessible. (Fig. 5) Drain placement in pelvis and port site closure. Limited vertical cystotomy. Separation of bladder and vagina. Vaginal closure. Bladder closure. Omentum interposition. Outcomes for Series Published till Date (≥10 Case Series)
Post Operative Management
Early mobilization preferably starting 8 hours postoperative and resumption of normal diet as early as possible. Avoid and manage clot retention early if it does occur, to avoid any pressure on the integrity of bladder closure. Prophylactic antibiotics till catheter removal. Anticholinergics for 2 weeks. Pelvic Drain is removed once output is <30 mL. Ureteric catheter removed on POD 3 to 7 days based on the quality of reconstruction and surgeon’s preference. In straight forward cases with healthy tissue margins, the ureteric catheters may be removed in the immediate postoperative period also. Per urethral catheter removed at 2–3 weeks (cystogram may be done prior to catheter removal as per the operating surgeon’s preference). Sexual abstinence for 6 weeks is advised. Patients is counselled about measures to overcome possible sexual and voiding dysfunction post operatively.
Consent
Obtained from the patient.
Footnotes
Authors’ Contributions
A.K.—Proof read the article, operated upon the patient shown in the video. A.T.K.—drafted the article, assisted in surgical procedure that has been shown in the video, edited the video. H.S.—drafted the article, assisted in surgical procedure that has been shown in the video, gave voice over to the video. S.Y.—drafted and proof read the article, edited the video, operated upon the patient shown in the video. R.M.—proof read the article, edited the video. P.M.S.—drafted the article, edited the video. A.G.—drafted the article, edited the video. Robotic Vesico-vaginal fistula Repair.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.