
Abstract
Purpose:
Retrograde intrarenal surgery is the gold-standard treatment for most kidney stones. During ureteroscopy, ureteral access sheath insertion at forces greater than 8.0 Newtons (N) risks high-grade ureteral injury. To monitor force, our institution utilizes a unique, Bluetooth-equipped device (i.e., the University of California—Irvine Force Sensor). Given the unique nature of the force sensor, we sought to develop an inexpensive and accessible force sensor based on Boyle’s law and the specific amount of force required to compress an occluded 1.0 mL syringe.
Materials and Methods:
We evaluated three brands of 1.0 mL syringes. After setting the plunger at 1.0 mL, the syringe was occluded, and the syringe plunger was compressed. The syringe volume was recorded when the applied force on the plunger reached 4.0 N, 6.0 N, and 8.0 N. Multiple trials were performed to assess reliability and reproducibility. A method for applying this clinically was also developed.
Results:
The precise force thresholds identified for a 1.0 mL Luer-Lok™ Syringe (Becton Dickinson, Franklin Lakes, NJ) were 0.30 mL for 4.00 N, 0.20 mL for 6.00 N, and 0.15 mL for 8.00 N. The 1.0 mL Tuberculin Syringe and 1.0 mL Luer Slip Syringe were less precise, but compression from 1.0 to 0.40 mL, 0.25 mL, and 0.20 mL corresponded to force sensor readings that did not exceed 4.00 N, 6.00 N, and 8.00 N, respectively.
Conclusions:
Based on volume changes, 4.00 N, 6.00 N, and 8.00 N of force can be reliably and reproducibly achieved using an occluded 1.0 mL syringe.
Introduction
Retrograde intrarenal surgery (RIRS) is the gold standard for the management of kidney stones that are less than 2 cm. 1 In RIRS, ureteral access sheaths (UAS) and ureteroscopic instruments are passed up the ureter to allow for incisionless, natural orifice access to the kidney. UAS facilitates stone treatment by allowing for the repeated and safe passage of the flexible ureteroscope into the kidney while maintaining a low intrarenal pressure, reducing the risk of sepsis, and decreasing operative time. 2 –4 Despite these benefits, there is an ongoing reluctance to use UAS because of concerns over UAS-induced ureteral injury; prior studies revealed low-grade injuries in 47.8% of patients and high-grade injuries—involving splitting of the ureter with exposure of the periadventitial adipose layer—in 23.8% of patients. 5
It has been postulated that the mechanism of ureteral injury during UAS deployment is related to the surgical force used to deploy the UAS. In this regard, porcine studies using a proprietary University of California, Irvine-developed force sensor (UCI-FS) (Fig. 1) characterized the forces exerted upon the ureteral wall during UAS insertion, demonstrating that high-grade ureteral injuries were routinely noted at forces ≥8.0 Newtons (N). 6 A subsequent prospective randomized clinical trial in humans with 210 anatomically normal renal units (no reconstruction, radiation exposure, or transplantation) and the UCI-FS demonstrated that a surgical force <8.0 N during UAS deployment precluded high-grade ureteral injury. In this study, an insertion force of ≤6.0 N was recommended for the safe passage of UAS, resulting in successfully deploying 16 Fr UAS in 61% of renal units. 7 We concluded that these findings corroborated the importance of continuous and precise force monitoring during UAS insertion to mitigate the risk of high-grade ureteral injury while optimizing the size of the UAS deployed.
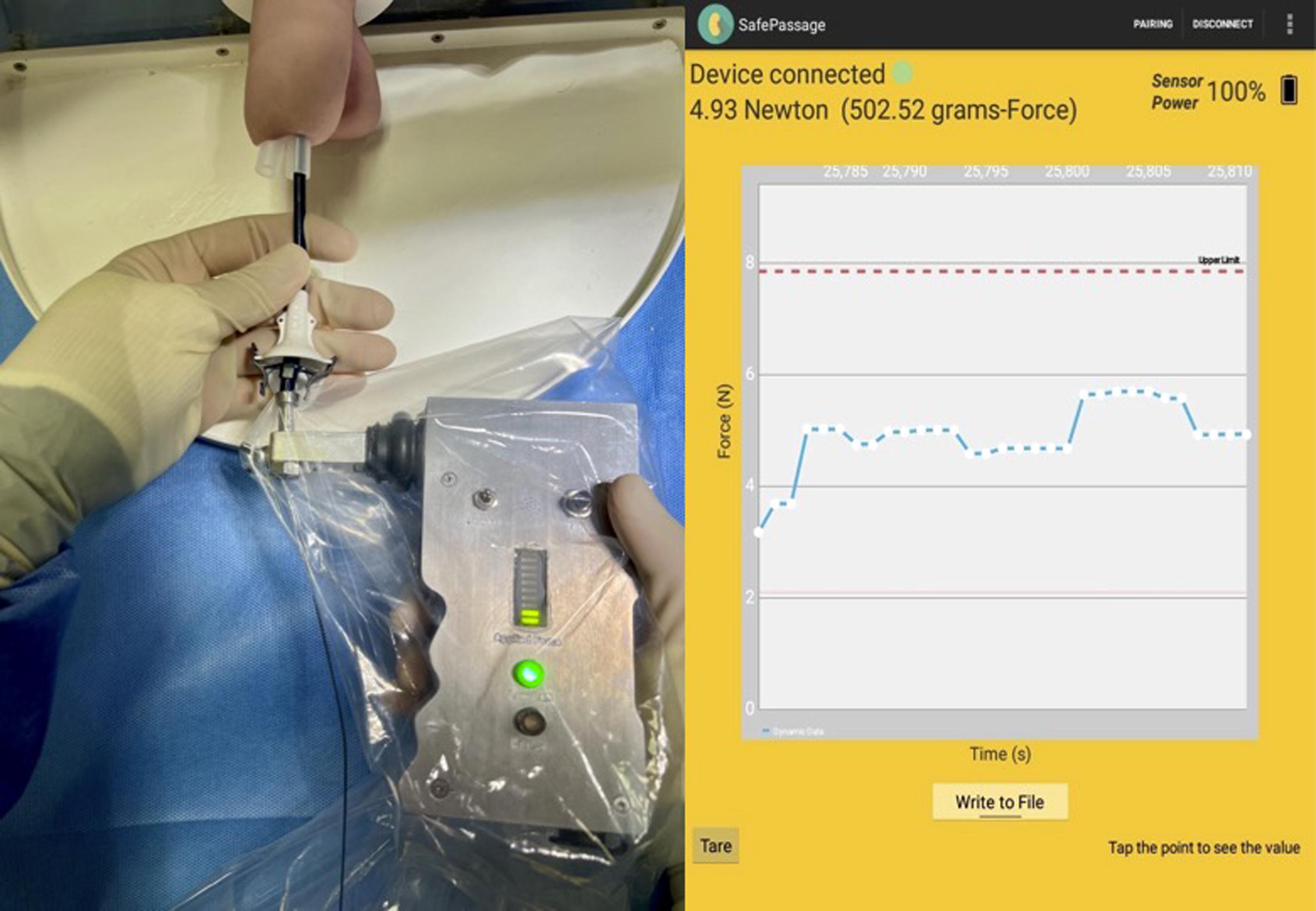
Proprietary mechanical UAS force sensor (UCI-FS) connected to a UAS over a guidewire with a screenshot of sample force reading. UAS = ureteral access sheath; UCI-FS = University of California, Irvine force sensor.
Despite the importance of surgical force monitoring during UAS insertion, the UCI-FS is not widely available. The UCI-FS is a complex, Bluetooth-equipped instrument that detects an applied force in 1/100ths of a Newton through an internal spring. Given the value of force information, we sought to develop an easily assembled, accessible, and affordable force sensor (i.e., “compressed air pressure sensor” or CAPS) that any urologist in the world could construct.
The CAPS concept is based upon Boyle’s law (P1V1 = P2V2). Boyle’s law states that at a constant temperature, the pressure of any given quantity of ideal gas is inversely related to its volume. 8 In a completely airtight, occluded 1.0 mL syringe, compression of the syringe with the plunger starting at 1.0 mL to a specific lower volume requires an increasingly specific and theoretically reproducible, measurable amount of pressure (Fig. 2A). In this system, the initial pressure P1 (atmospheric pressure), the initial volume V1 (1.0 mL), and the final volume V2 (the final volume of compressed air) are all known—accordingly, the final pressure P2 can be calculated. As such, the final pressure, P2, can be converted to force, given that pressure (P) equals force (F) divided by area (A). In the cases of a 1.0 mL syringe, the area would be the inner circle of the syringe. Thus, we can translate a change in volume to a force in Newtons generated within an occluded 1.0 mL syringe (Fig. 2B).
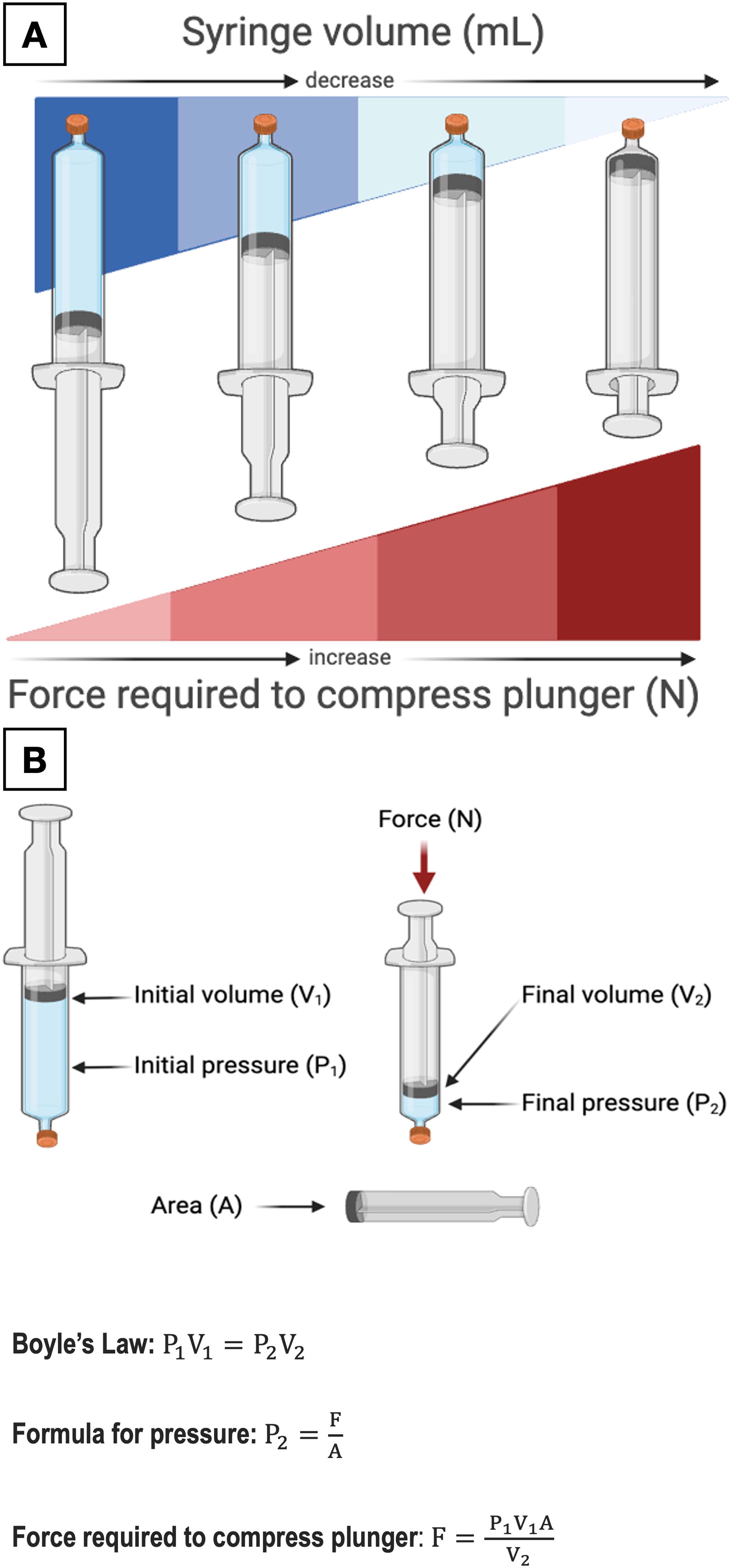
Given that 8.00 N is a threshold of crucial importance during UAS insertion, we sought to apply Boyle’s law to estimate the amount of compression necessary in an occluded 1.0 mL syringe to reach 8.00 N; we also defined the amount of compression to reach forces of 4.00 N and 6.00 N. The latter information was sought as we believe that if the UAS is placed with a force of 4.00 N or less, then the impact on the ureteral wall is minimal, and thus, postprocedural indwelling ureteral stenting may not be necessary; this hypothesis is currently being tested in an ongoing clinical trial at UCI. Furthermore, we routinely seek to exert 6.00 N to place a larger UAS as this force allows a larger sheath to be safely placed than if less force was applied (16 Fr at 5.47 N vs. 14 Fr at 5.28 N vs. <13 Fr at 4.22 N). 9
The following text documents a series of benchtop tests using the UCI-FS to calibrate several 1.0 mL occluded syringes from different manufacturers to determine the reproducibility of both intersyringe and intrasyringe volumes corresponding to 4.00 N, 6.00 N, and 8.00 N. In addition, we include instructions on assembling a force sensor costing <$4.00 from materials readily available in the operating room.
Materials and Methods
Syringe collection
We collected three brands of 1.0 mL medical-grade syringes: Luer-Lok™ Syringe (Becton Dickinson [BD], Franklin Lakes, NJ), Tuberculin Syringe (BD), and Luer Slip Syringe (Berpu Medical Technology, Zhejiang, China). The syringes were collected from several practice sites at the UCI Medical Center: operating room, outpatient surgical center, anesthesia preoperative clinic, pain clinic, urology clinic, and inpatient wards. Five syringes of each brand of syringe were tested using the UCI-FS while pushing the occluded syringe against a flat surface (Fig. 3).
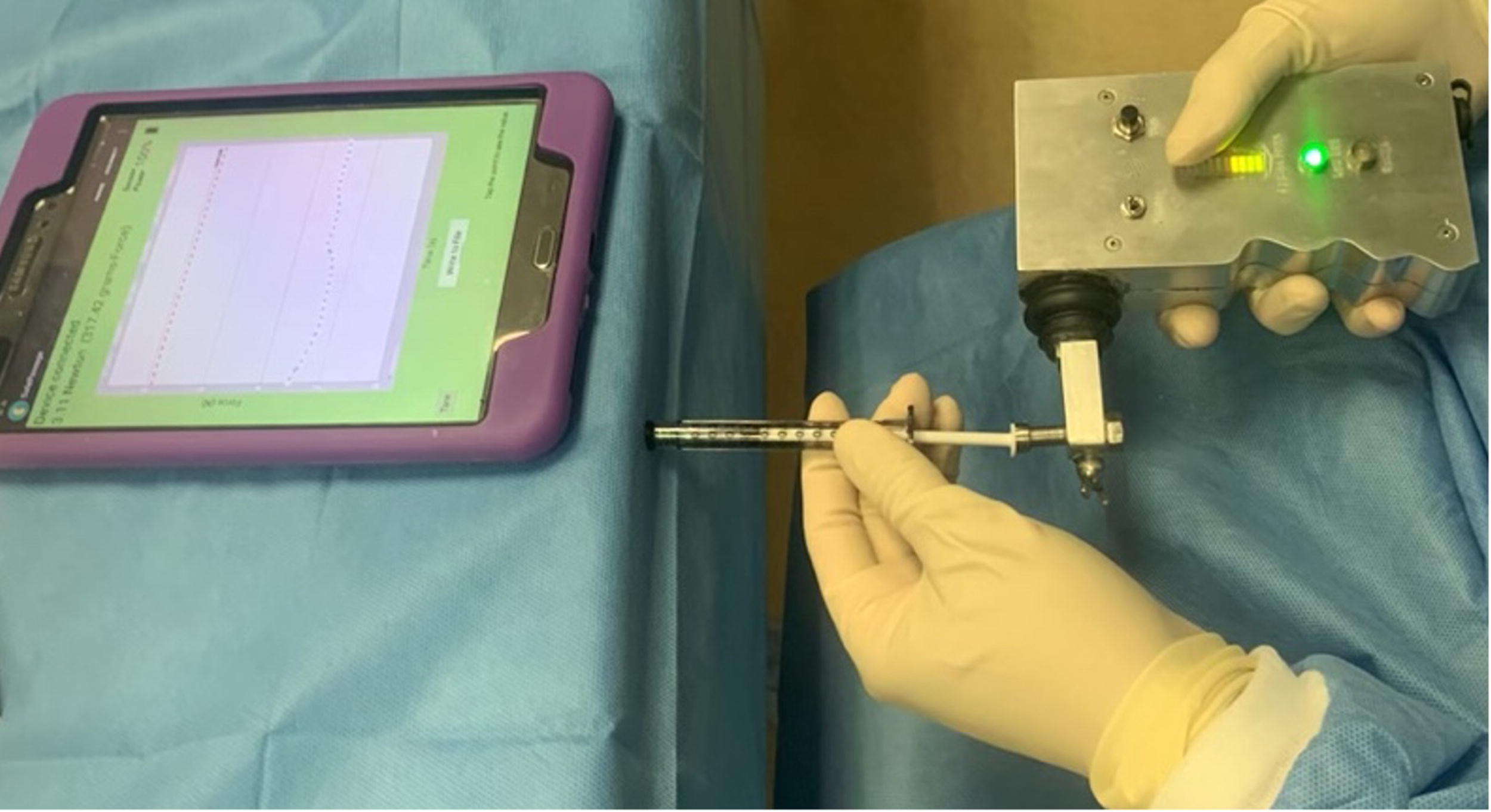
Experimental setup testing the relationship between applied force and the change in volume of an occluded 1.0 mL syringe with the UCI-FS.
Syringe testing protocol
The UCI-FS was first calibrated with standardized tungsten weights to ensure its accuracy and precision to 0.01 N. The CAPS 1.0 mL syringe was prepared by placing the syringe plunger at the 1.0 mL mark. Next, the syringe tip was occluded using a BD Luer Tip Cap (BD), thereby making the syringe completely airtight. Then with the occluded tip of the syringe flush on the laboratory bench, the UCI-FS was abutted against the plunger of the syringe, and the UCI-FS was pushed against the plunger, slowly advancing it at a constant rate until 4.00 N, 6.00 N, and 8.00 N were reached (Fig. 3). For each test, the UCI-FS forces of 4.00 N, 6.00 N, and 8.00 N were correlated with the milliliter graduations at the point of descent of the 1.0 mL syringe’s plunger at which each of those three forces was exerted. These milliliter readings were recorded.
Assessing reliability and reproducibility within and between syringe brands
We collected a total of 15 1.0 mL syringes from three different brands (n = 5/brand). Five consecutive experimental trials were performed for each syringe. Each reading was done in quintuplicates for a total of 225 readings. All trials were randomized and conducted at room temperature in a single session in our laboratory. Syringe testing was distributed evenly between two fully trained urologists (B.M.G. and J.A.-V.) who completed the measurements independently.
Statistical analyses
Continuous variables were displayed as mean and standard deviation. For each force threshold (i.e., 4.00 N, 6.00 N, and 8.00 N) and syringe brand (i.e., Luer-Lock™, Tuberculin, Luer Slip), analysis of variance (ANOVA) testing followed by Tukey’s post-hoc analysis assessed the consistency of each syringe’s force-specific volume. F-tests compared the standard deviations of the independent syringe group readings. All statistical analyses were performed using IBM SPSS Statistics 29.0 (IBM Corp., Armonk, NY). Graphs were generated using GraphPad Prism 10.0.1 (GraphPad Software, Boston, MA).
Force sensor assembly for clinical use
To move this device into the clinical realm, we devised a simple setup using inexpensive, widely available materials (Fig. 4). The tip of a 1.0 mL Luer-Lok Syringe is affixed to a Luer Tip Cap (BD) covered with Mastisol liquid adhesive. The plunger of a 20.0 mL Luer-Lok Syringe is removed. The 1.0 mL Luer-Lok Syringe is then placed inside the barrel of the 20.0 mL Luer-Lok Syringe. The flange on the 1.0 mL Luer-Lok Syringe is then clamped with a short Kelly clamp to the flange of a 20.0 mL Luer-Lok Syringe, thereby securing the two syringes together (Fig. 4). The open tip of the 20.0 mL syringe is passed over the same guidewire over which the UAS has been passed; the 20.0 mL syringe is then secured into the Luer-Lok end of the obturator of the UAS. The surgeon supports the UAS with one hand and then, with the other hand, slowly pushes on the syringe plunger, thereby advancing the 1.0 mL syringe, the 20.0 mL syringe, and the UAS simultaneously as a single unit. The surgeon carefully watches as the 1.0 mL plunger descends from the 1.0 mL mark; the UAS is advanced up the ureter until it either reaches the desired location or the plunger on the 1.0 mL syringe has descended to the 0.20 mL mark, which would indicate that the force on the UAS is now 6.00 N based on our experimental findings. The total cost to assemble the CAPS device is <$4.00 (Supplementary Table S1).
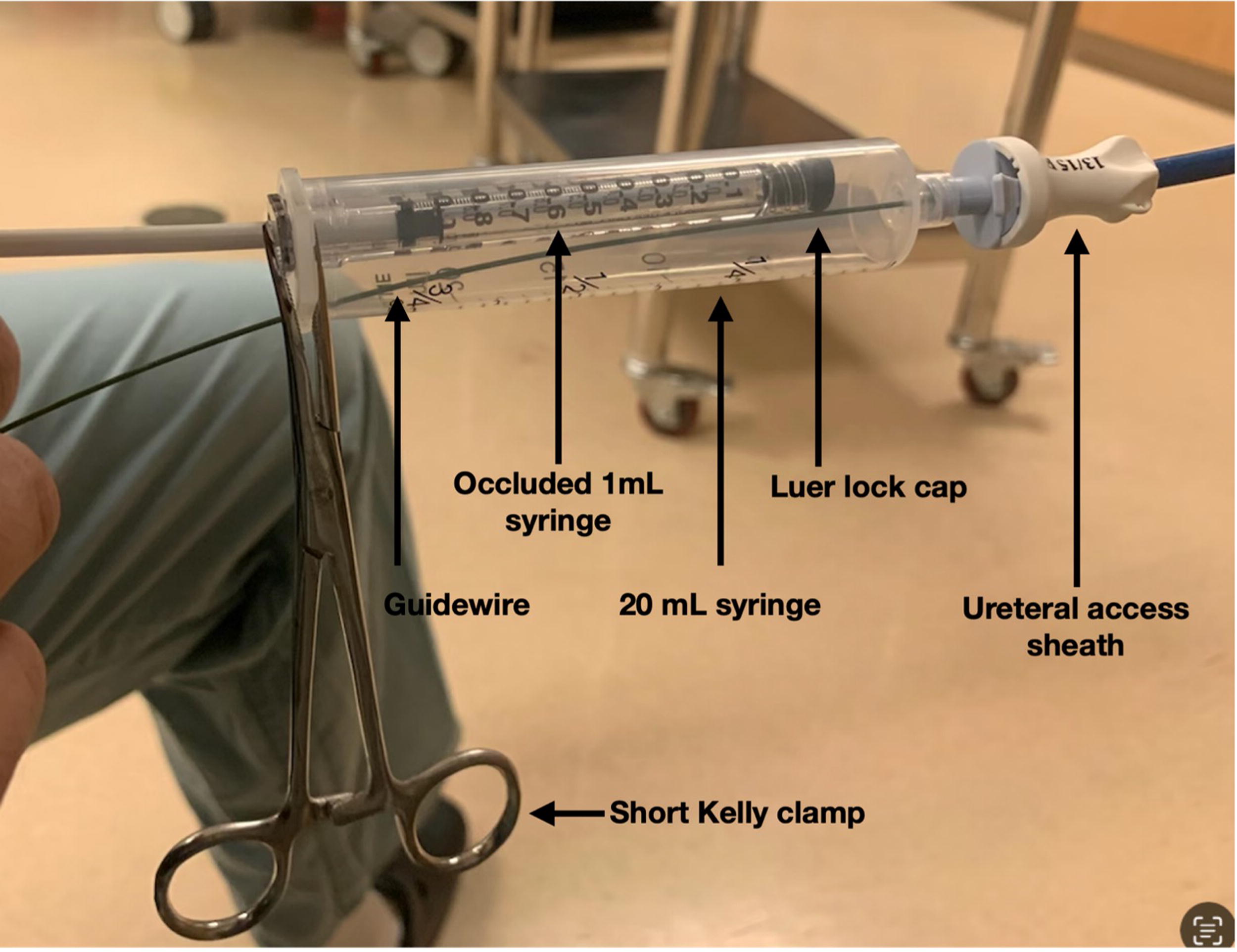
Labeled setup of CAPS surgical force sensor over a guidewire attached to a UAS for clinical use. CAPS = compressed air pressure sensor.
Results
Luer-Lok Syringe
A force of 4.00 N, 6.00 N, and 8.00 N compressed the occluded syringe to a mean volume of 0.295 ± 0.010 mL, 0.198 ± 0.006 mL, and 0.145 ± 0.006 mL, respectively (Fig. 5). The measurements were consistent across different copies of the same syringe at 4.00 N, 6.00 N, and 8.00 N force thresholds. ANOVA and Tukey’s post-hoc analysis between five replicate syringes of the same brand showed nonstatistically significant differences at all force thresholds (4.00 N, p = 0.11; 6.00 N p = 0.36; 8.00 N p = 0.26) (Supplementary Fig. S1).
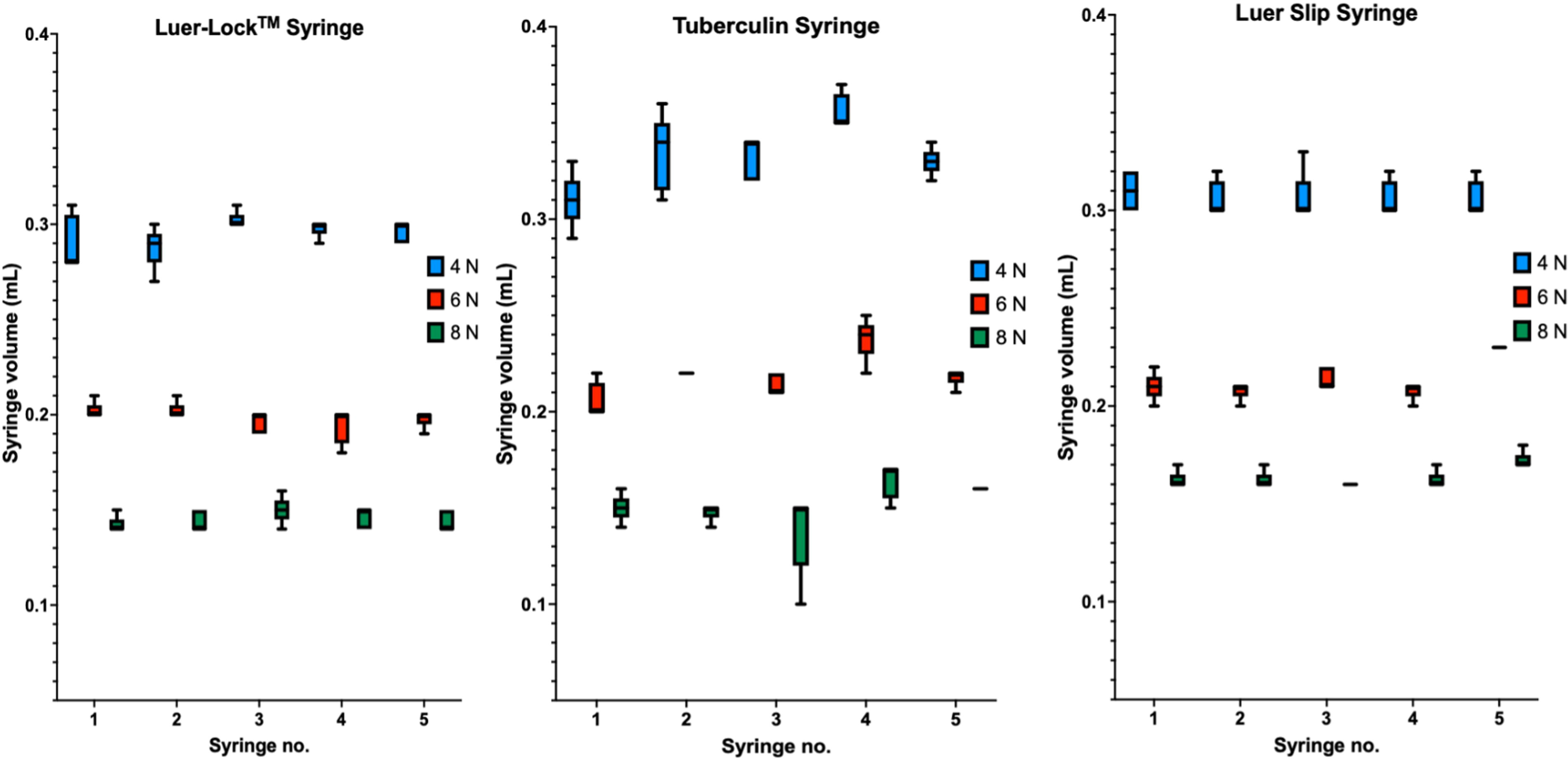
Syringe volume marking to push the syringe plunger to reach force thresholds of 4.00 N, 6.00 N, and 8.00 N when compressing an airtight 1.0 mL syringe with the plunger starting at 1.0 mL. Each syringe brand has five identical syringes with five trials per syringe.
Tuberculin Syringe
A force of 4.00 N, 6.00 N, and 8.00 N compressed the occluded syringe to a mean volume of 0.332 ± 0.019 mL, 0.219 ± 0.013 mL, and 0.152 ± 0.014 mL, respectively (Fig. 5). The measurements were less consistent across different copies of the syringe at 4.00 N, 6.00 N, and 8.00 N force thresholds. ANOVA and Tukey’s post-hoc analysis between five replicate syringes of the same brand showed statistically significant differences at all force thresholds (4.00 N, p = 0.0005; 6.00 N, p = 0.0001; 8.00 N, p = 0.001) (Supplementary Fig. S1).
Luer Slip Syringe
A force of 4.00 N, 6.00 N, and 8.00 N compressed the occluded syringe to a mean volume of 0.307 ± 0.009 mL, 0.214 ± 0.010 mL, and 0.164 ± 0.006 mL, respectively (Fig. 5). The measurements were less consistent across different copies of the syringe at 4.00 N, 6.00 N, and 8.00 N force thresholds. ANOVA and Tukey’s post-hoc analysis between five replicate syringes of the same brand showed statistically significant differences at all force thresholds (4.00 N, p = 0.0001; 6.00 N, p = 0.0001; 8.00N, p = 0.0010) (Supplementary Fig. S1).
Overview
Multiple independent sample F-tests revealed that the Luer-Lok Syringe displayed consistent results, whereas the Luer Slip and Tuberculin Syringes displayed less consistent results (statistically significant higher variance) (Supplementary Table S2). For the Luer-Lok Syringe specifically, compressing the syringe to a volume of 0.30 mL, 0.20 mL, and 0.15 mL corresponds to a force of 4.00 N, 6.00 N, and 8.00 N, respectively. For the other two syringes, there was increased variability and compressing to a volume of 0.40 mL, 0.25 mL, and 0.20 mL provided a force that would not exceed 4.00 N, 6.00 N, and 8.00 N, respectively.
Discussion
There is an ongoing reluctance to use UAS because of concerns over UAS-induced ureteral injury; however, this problem can be eliminated by a force sensor during UAS insertion. 6,7 The present study introduces CAPS: an accessible and cost-effective intraoperative force sensor. By applying Boyle’s law, our benchtop setup indicates that CAPS can reliably estimate the surgical force applied on an occluded 1.0 mL syringe based on volume change during UAS insertion (Fig. 6). The force thresholds identified for the Luer-Lock Syringe—0.30 mL for 4.00 N, 0.20 mL for 6.00 N, and 0.15 mL for 8.00 N—are of paramount importance as forces exceeding 8.00 N are associated with high-grade injuries, whereas forces less than 4.00 N might undersize the UAS placed. 7 Our findings demonstrate that the volume of room air compressed within the modified syringe can be correlated with the force exerted.
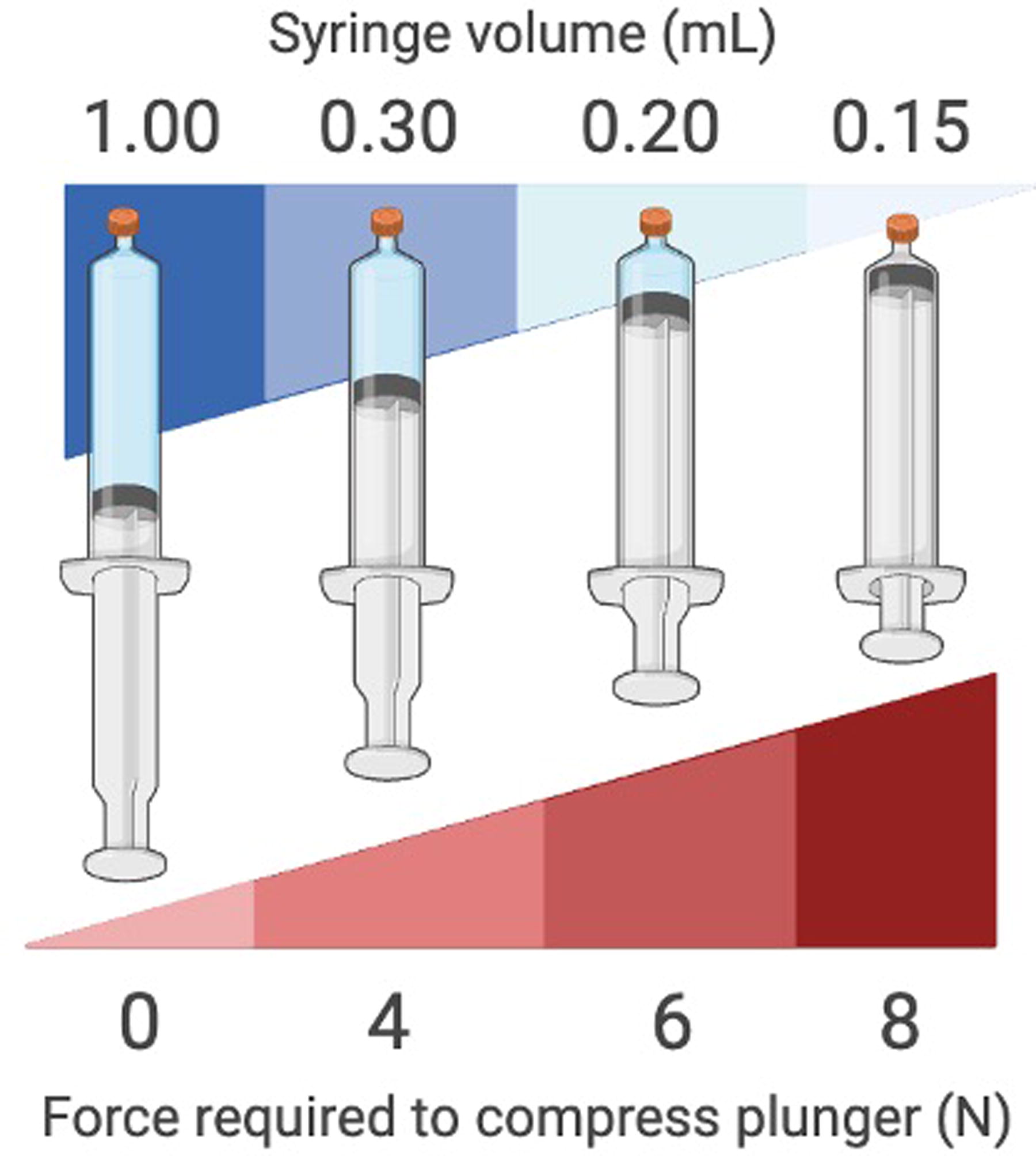
The volume to push the syringe plunger (Luer-Lock syringe) to reach force thresholds of 4.00 N, 6.00 N, and 8.00 N when compressing an airtight and occluded 1.0 mL syringe with the plunger starting at 1.0 mL.
The comparative analysis of three different brands of 1.0 mL syringes revealed that only the Luer-Lok Syringe displayed no significant variability across multiple tests at all three force thresholds, underscoring its potential as a reliable force sensor. Although the Tuberculin and Luer Slip Syringes demonstrated a broader range in testing, compressing the two syringes to a volume of 0.40 mL, 0.25 mL, and 0.20 mL still ensured that force would not exceed 4.00 N, 6.00 N, and 8.00 N, respectively. In this regard, the slight difference in mean volume to reach the force thresholds among syringe brands is likely due to the difference and potential variability in the surface area of the syringe’s plunger, which would affect the pressure–volume relationships (Luer-Lok inner diameter [ID] 4.8 mm; Tuberculin ID 4.5 mm; Luer Slip ID 4.6 mm).
Notably, the CAPS sensor embodies a user-friendly design, requiring minimal setup using items readily available in operating rooms around the world with a total cost of less than $4.00. With this easy-to-assemble device, the incidence of UAS-induced ureteral injuries could be markedly reduced globally.
Although designed to monitor surgical force during UAS passage, other possible applications depend upon future studies designed to define the tolerance of a broad array of tissues to an applied force. Discoveries in this new field of research (i.e., the science of surgical force) may eventually provide invaluable insight into what the “safe” or threshold force is for a broad variety of tissues (e.g., vein, artery, esophagus, colon, urethra, and abdominal wall). This, in turn, could ensure the safe passage of a variety of clinical instruments across surgical fields, including but not limited to Veress needle entry of the abdomen, laparoscopic trocar placement, percutaneous renal access, the passage of catheters or endoscopes, or deployment of surgical retractors not to injure the retracted tissue.
There are natural limitations to our described findings. Specifically, the application of Boyle’s law assumes an ideal gas and can be influenced by the atmospheric pressure of the operating room. To this end, we applied Boyle’s law to compare Belgrade (the city with the highest barometric pressure in the world, 102.84 kPa) to Anchorage (the city with the lowest barometric pressure in the world, 98.51 kPa). Our calculations demonstrate the extremes of atmospheric pressure where ureteroscopy may be conducted, with the two cities resulting in a small theoretical difference of up to 0.02 mL in syringe thresholds. All testing in this study occurred in Orange, CA, a city close to sea level with a barometric pressure of 101.66 kPa. Furthermore, Boyle’s law assumes a constant temperature that may alter in rapid compression processes or extreme environments. Given that UAS insertion is slow and the operating room’s temperature is well controlled, the effect of a fluctuating temperature is potentially minimized. A final limitation is that the manual compression of the syringe might introduce user variability, which warrants further investigation into standardizing the technique or designing a commercialized pneumatic syringe-based force sensor.
Conclusion
In conclusion, pushing an occluded 1.0 mL Luer-Lok Syringe from 1.00 mL to 0.30 mL, 0.20 mL, and 0.15 mL requires precisely 4.00 N, 6.00 N, and 8.00 N of force.
Footnotes
Acknowledgments
The authors wish to express their sincere appreciation to B.M.G.’s cousin, Enray Li, whose high school chemistry homework on Boyle’s law sparked the inspiration for this study.
Authors’ Contributions
B.M.G., J.C.T., and R.V.C. were responsible for the conceptualization of the project. The methodology design was contributed to by B.M.G., J.C.T., A.D.C., J.A.-V., Y.X.W., E.G., and R.V.C. B.M.G. and A.D.C. conducted the statistical analysis. B.M.G. and J.A.-V. carried out the experiments. J.C.T., A.D.C., S.S., and V.P. provided assistance in experimental data collection and curation and also facilitated the acquisition of 1.0 mL syringes. The initial draft of the article was written by B.M.G. and J.C.T. B.M.G. also developed the original figures for the article. The article was reviewed and edited by J.C.T., A.D.C., J.A.-V., S.S., V.P., E.G., Y.X.W., Z.E.T., S.N.A., P.J., R.M.P., J.L., and R.V.C. J.L. and R.V.C. provided the study materials, equipment, and laboratory space.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
No external funding was used for the completion of this study.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Abbreviations used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.