
Abstract
Purpose:
Ureteral stents are extensively utilized in the treatment of urolithiasis. Given the anatomical and physiological differences between children and adults, the rational, effective, and safe application of ureteral stents in pediatric patients is a matter of significant clinical interest. This review summarizes the classification, application scenarios, and potential adverse effects of ureteral stents in pediatric urolithiasis, aiming to provide a reference for clinical decision-making related to ureteral stents in children with urinary tract stones.
Materials and Methods:
A systematic review was conducted by searching PubMed, Embase, and Cochrane with the keywords “ureteral stent,” “urolithiasis,” and “pediatric” up to June 4, 2024. The review exclusively included comparative trials. Information regarding patient medical records and treatment efficacy were meticulously extracted.
Results:
For uncomplicated cases, routine placement of ureteral stents before and after extracorporeal shock wave lithotripsy, ureteroscopic lithotripsy, percutaneous nephrolithotomy, and open stone surgery do not confer significant clinical benefits. Selective stent placement is recommended for complex cases with intraoperative ureteral injury, ureteral stricture, anatomical or functional solitary kidney, or renal impairment. Novel ureteral stents have shown promise in reducing stent-related complications, avoiding secondary anesthesia, and decreasing health care-related costs.
Conclusions:
Currently, there is no consensus on the indications for ureteral stent placement in children in clinical practice. Urologists should selectively place ureteral stents based on the medical center’s conditions, the child’s condition, and intraoperative findings. The future development direction of ureteral stents is to improve the postoperative quality of life of patients, reduce stent-related complications, and facilitate stent removal.
Introduction
Ureteral stents are an essential tool in the treatment of urinary tract stones, serving to drain urine and passively dilate the ureter. With a growing incidence of pediatric urolithiasis, the management of urolithiasis has become increasingly important. 1 In recent years, there have been increasing reports of stent-related complications such as pain, bladder irritation, urinary tract infections, and stent encrustation, which have raised concerns about the rational, effective, and safe application of ureteral stents in children. The unique anatomical and physiological characteristics of children, along with the specific considerations required for stone surgery and anesthesia methods, present distinct challenges compared with the adult population. 2
The current clinical guidelines for ureteral stent use are primarily based on adult data, and the evidence related to children is still insufficient, with no consensus yet. This systematic review aims to synthesize the available evidence for the materials and design of stents, indications for stent placement in children, and the management of stent-related complications, providing a reference for clinical decision-making related to ureteral stents in pediatric stone disease.
Materials and Methods
Search strategy
A systematic research was conducted by searching PubMed, Embase, and Cochrane databases with the keywords “ureteral stent,” “urolithiasis,” and “children” up to June 4, 2024. This was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Selection criteria
We analyzed articles that met the following criteria: a randomized controlled trial (RCT) or a nonrandomized comparative trial, the subjects are children under the age of 18, articles published in English and examined the application of stents in stone treatment. Exclusion criteria were noncomparative studies, case report, and review articles.
Data extraction
Two researchers (Q.H. and H.L.) independently extracted the following information: authors, publication year, article type, sample size, subject age, stone size, stent type, stent indwelling time, success rate, and complications.
Results
Out of 25 pertinent publications identified, a total of seven studies met the criteria for inclusion in our systematic review.3–9 Eighteen studies were excluded because of their noncomparative nature (Fig. 1). The quality assessment of the included studies is provided in the Supplementary Data. Among these studies, six employed Double-J (DJ) stents, while the remaining one provided insufficient details regarding the specific types of stents used. The duration that stents were left in situ varied across the studies, ranging from 24 hours to 15 weeks.

Flowchart for article selection of the review.
Among the seven eligible studies, two studies examined the success rate and associated complications of DJ stenting versus no stenting in extracorporeal shock wave lithotripsy (ESWL).3,7 Three studies investigated the impact of prestenting on the outcomes of ureteroscopic lithotripsy (URL).4–6 In addition, one study compared the efficacy of percutaneous nephrolithotomy (PCNL) and DJ stent in the initial urinary drainage in children with obstructive anuria and acute renal failure because of ureteral stone. 9 Another study examined the success rate and complications of DJ stenting in laparoscopy ureterolithotomy 8 (Table 1).
Characteristics of the Included Studies
DJ = Double-J; ESWL = extracorporeal shock wave lithotripsy; NA = not applicable; NR = not reported; PCN = percutaneous nephrostomy; PCNL = percutaneous nephrolithotomy; SD = standard deviation; URL = ureteroscopic lithotripsy.
Discussion
Stent material and design
Stent material
The ideal material for ureteral stents should reduce bladder irritation, urinary tract infection rates, stent encrustation, and facilitate easy removal or biodegradability. Commonly used materials include silicon and polyurethane. Polyurethane stents offer good mechanical properties and drainage capabilities but are prone to encrustation. Silicon stents are softer, have a lower rate of encrustation, and are widely used in clinical settings. 10 Other polymeric materials, such as organosilicon copolymers (Cook® C-Flex) and polyolefin copolymers (Percuflex™), have improved the physical properties of stents but have not yet effectively addressed the issue of encrustation associated with long-term stent placement.
Biodegradable stents can avoid the need for secondary anesthesia when removing stents in children, reducing urinary tract injury, pain, and medical costs. A key challenge for biodegradable stents is to ensure effective mechanical properties while degrading adequately within a set timeframe to prevent obstruction by degradation fragments. Barros et al. reported a biodegradable stent made from a mixture of alginate, gellan gum, and gelatin that demonstrated high biocompatibility, low bacterial contamination, and a low tendency for encrustation, which was validated in a porcine model. 11 Biodegradable stents represent an important area of future research with broad application prospects in pediatric urolithiasis.
Stent coating
Coatings are a solution to reduce stent encrustation and suppress stent-related infections. Hildebrandt et al. reported a heparin-coated stent that showed good antiencrustation effects in both in vitro and clinical trials. 12 Zhao et al. recently reported on a propolis ethanol extract-coated stent, which in vitro tests showed could eliminate more than 90% of bacterial biofilm attached to the stent and maintain antibacterial properties for up to 3 months. 13 In vivo experiments indicated that this stent significantly reduced bacteria, calculi, and salt deposits on the surface of the ureteral stent and mitigated inflammatory responses. 13 Other coatings, such as hyaluronic acid, antibiotic-added hydrogel coatings, and nanosilver coatings, are still in the preclinical trial stage, and no in vivo tests have yet proven their effectiveness in reducing stent encrustation.14,15 How to ensure that coated stents stably function in the body is a question that needs to be explored in the future.
Stent design
To reduce stent-related complications, various types of ureteral stents have been reported in recent years, such as DJ stents, single-J stents, fishtail stents, dual-durometer stents, and antireflux stents. Among them, DJ stent is currently the most widely used stent type in pediatric urinary tract stones, which fixes the stent in the ureter through the DJ structure to prevent stent displacement. Fishtail stents and dual-durometer stents both reduce bladder irritation by improving the morphology of the bladder end of the stent, enhancing patient comfort. Antireflux stents, use an antireflux membrane flap formed by a lumen to play an antireflux role, thereby alleviating pediatric lumbar pain and urinary tract infection (Fig. 2).
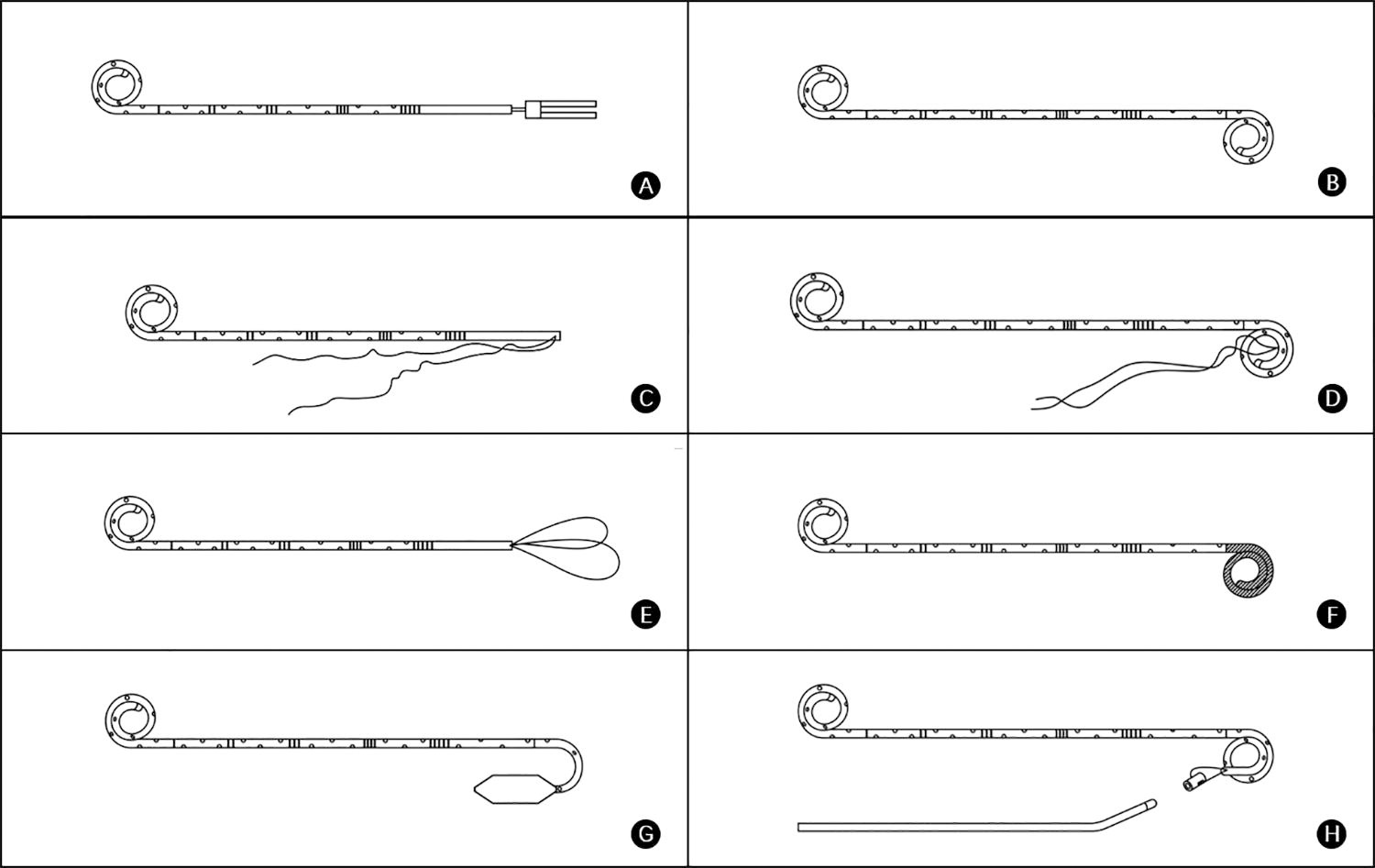
Stents commonly used for pediatric urolithiasis.
Stent removal methods
Because of higher tolerance and cooperation in adults, stents are usually removed under local anesthesia via cystoscopy, while most children have poor compliance, requiring general anesthesia for stent removal. Therefore, some researchers have improved stent removal methods to avoid the secondary anesthesia brought by stent removal. Some clinicians fix the stent to the catheter or ureteral catheter, and the stent is removed together with it after the operation, which is suitable for children with shorter stent retention time. 16
The “string method” involves pulling the string connected to the tail end of the DJ stent out of the body to remove the stent. Compared with the cystoscope method, this method has a higher emergency visit rate (6.6% in cystoscopy vs 11.3% in string method, p = 0.05) for severe pain. 17 Studies have shown that for patients with no history of urinary tract infection, string stents usually do not increase the risk of urinary tract infection. 18 However, for children with a history of urinary tract infection, especially female pediatric patients, the risk of urinary tract infection associated with string stents significantly increases, and antibiotic prophylaxis cannot reduce this risk. 19
The “magnet method” uses the magnet on the remover to attract the magnet at the tail end of the DJ stent to remove the stent. However, because of the large volume of the magnet, the insertion failure rate of the magnetic DJ stent is as high as 34%, the removal failure rate is 4%, and the magnetic DJ stent limits the application of nuclear magnetic resonance imaging. 20
The “fishing method” uses a self-made “fishing rod” to remove the stent. This method avoids secondary anesthesia for children and reduces the risk of iatrogenic injury from cystoscope insertion (Fig. 3). Sundaramurthy et al. compared the effectiveness of the “fishing method” and cystoscopy in removing DJ stents, showing that it is noninferior to the cystoscope method while avoiding anesthesia and reducing costs. 21
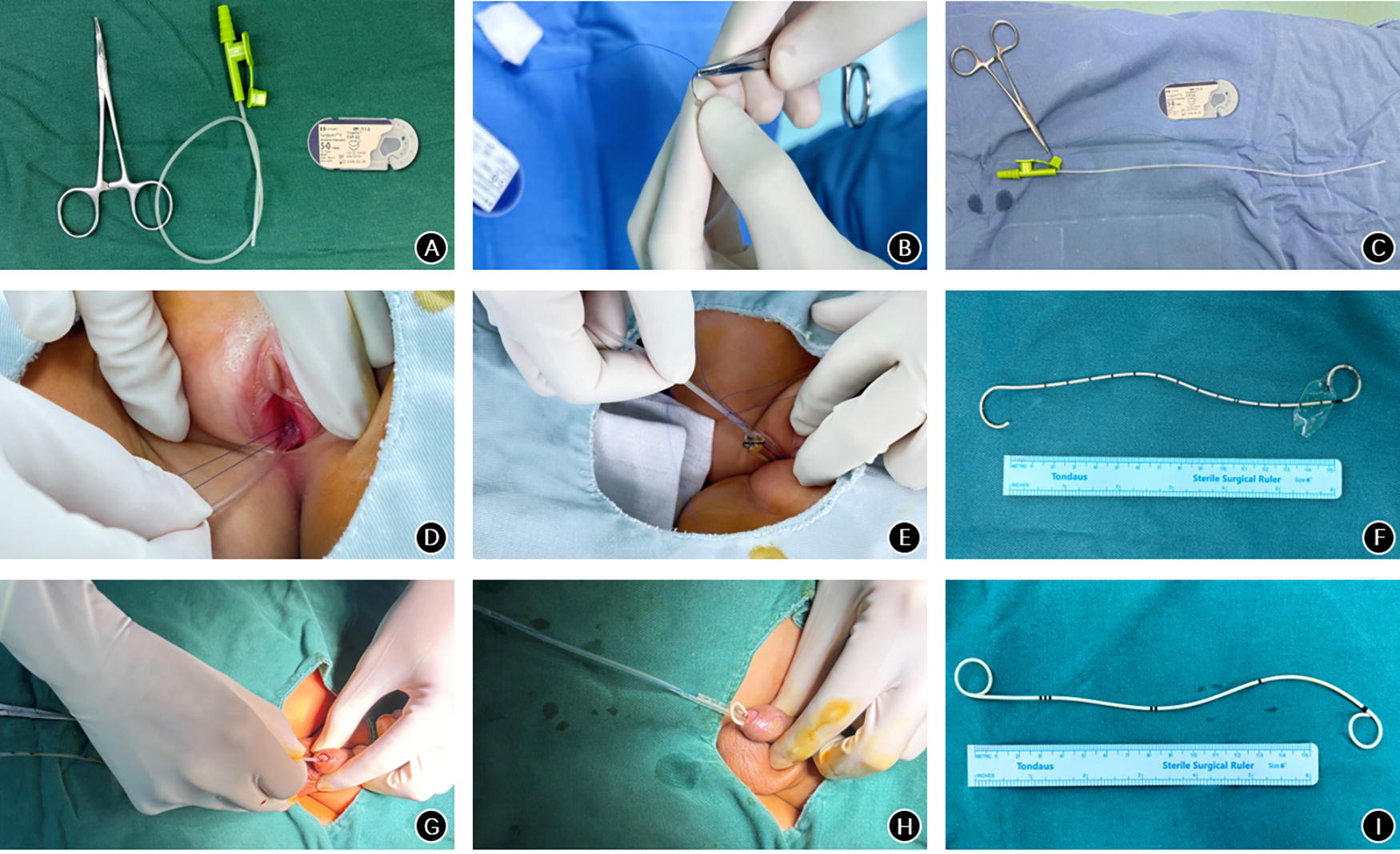
The “fishing method” to remove ureteral stent. Patients received propofol, midazolam, and nalbuphine intravenously before the surgery. Preoperative bladder distention by holding urine before surgery. The patients were in the supine position.
Extracorporeal shock wave lithotripsy
ESWL is primarily indicated for the treatment of upper urinary tract stones less than 20 mm in size, with a stone-free rate of 70% to 90% in children. 1 A meta-analysis including eight randomized comparative trials (n = 876) have shown that stenting before ESWL does not improve the stone-free rate (78.1% in stented group and 83.0% in stentless group, p = 0.27) or does it reduce auxiliary treatment after ESWL (Risk Ratio [RR] 1.43, 95% confidence interval [CI] 0.70–2.92, p = 0.33). 22 Although stents may prevent the formation of Steinstrasse, the incidence of Steinstrasse is inherently lower in children compared with adults. 8 Considering the clinical benefits and stent-related complications for pediatric patients, routine stent placement before ESWL in children is not recommended.
ESWL has also been attempted for the treatment of pediatric stones larger than 20 mm. Compared with adults, pediatric stones are relatively loose, and the high water content in the less muscular tissue results in minimal loss of shock wave energy. Additionally, the higher compliance of the pediatric ureter facilitates stone expulsion. Research suggests that both PCNL and ESWL have high stone-free rates for stones larger than 20 mm, and either methods can be chosen. 23 From the 1990s to the early 21st century, because of the significant invasiveness of standard PCNL in children, some researchers used ESWL to treat pediatric staghorn calculi, reporting stone-free rates of 73.3% to 87.5% with relatively few complications. 24 A nonrandomized controlled study by Al-Busaidy et al. found that stenting during ESWL did not improve the stone-free rate of staghorn calculi but could reduce the risk of postoperative complications. 3 With the miniaturization of the working channels in PCNL, it has become safer in children, offering higher stone-free rates compared with ESWL and gradually becoming the first-line treatment for pediatric staghorn calculi. However, in cases where medical facilities are insufficient or when ESWL is applicable (relative contraindications for PCNL, loosely packed stones, family preference, etc.), ESWL may be attempted for pediatric staghorn calculi.
Routine stent placement after ESWL in children is not standard. Stents are indicated for children with renal stones larger than 20 mm in total burden, those with anatomically or functionally solitary kidneys, and those with ureteral strictures. 23 The risk of post-ESWL obstruction and infection is higher for renal stones larger than 20 mm, and residual stones can easily lead to infection and recurrence. Postoperatively, close attention must be paid to the child’s pain, urinalysis, urination status, and stone expulsion.
Ureteroscopic lithotripsy
Currently, routinely placing a stent before URL is not standard.1,23 For pediatric patients in whom the initial ureteroscope insertion is unsuccessful, some institutions left a DJ stent in situ for 10 to 14 days to passively dilatate the ureter. Three publications explored the impact of prestenting prior to URL and concluded that this approach enhances the stone-free rate and reduces the incidence of complications.4–6 While there is no consensus on the duration of stent placement before surgery. Fahmy et al. compared stent placement 2 or 4 weeks before surgery and found no significant difference in the success rate of stone-free rate (86.6% vs 90%, p = 0.199). 25 However, the incidence of postoperative urinary tract infection increased with the prolonged duration of stent placement (6.7% in 2 weeks indwelling time and 30% in 4 weeks indwelling time, p = 0.046). Based on the author’s single-center clinical experience, it is suggested that the duration of preoperative stent placement should not exceed 2 weeks to reduce discomfort and lower the risk of infection.
The placement of a stent after URL remains a matter of debate. Some researchers believe that without stent placement, ureteral edema or mucosal inflammation caused by the surgery and the heavy burden of stones may lead to postoperative obstructive symptoms (pain, oliguria, etc.) or ureteral stricture. Some studies suggest that it is feasible to omit stent placement after URL. Kocaoglu et al. reported on the use of a 4.5F semirigid ureteroscope to treat 36 pediatric patients with urinary tract stones. Stents were placed in all 16 initial cases, but as surgical experience increased, stents were not used in the subsequent 20 cases. 26 In terms of complications, there was no statistical difference between the two groups, and no severe complications occurred. The placement of a stent after URL is a risk factor for complications, and for ureteral stones less than 10 mm, omitting stent placement after URL is effective and safe.
The placement and removal of stents significantly increase medical costs. A report assessing the cost of pediatric stone treatment found that the surgery of stent placement accounted for 20.4% to 24.1% of all surgeries. 27 The cost of stent placement/removal surgery is comparable to that of ESWL and URL. 27 Data from the author’s single center show that the treatment cost for children with stent placement is 1.8 times that of those without stents. In summary, it is believed that for experienced urologists, stent placement is not necessary after noncomplex URL for patients with a small stone burden and good ureteral conditions.
For some complex situations, such as intraoperative ureteral injury (laser burn or instrument abrasion), visible mucosal edema, ureteral tortuosity, stenosis, solitary kidney, or planned secondary surgery for URL, it is recommended to leave the stent in place. 1 The duration of postoperative stent placement has not yet been determined. A retrospective study comparing the impact of stent placement duration after URL on complications found that the incidence of fever, lumbar pain, and other complications in patients with stent placement for more than 2 weeks was 3.6 times that of those with less than 2 weeks. 28 The common duration for stent placement is currently 2 weeks postoperatively, and some medical centers fix the stent to the catheter, removing the stent along with the catheter 3 to 5 days after surgery. In summary, it is necessary to minimize the duration of stent placement while fully leveraging the drainage and stone expulsion functions.
Percutaneous nephrolithotomy
The application of PCNL in children dates back to 1985. Traditional PCNL concludes with the placement of a nephrostomy tube and/or a ureteral stent to facilitate the healing of the fistula, hemostasis, and urine drainage to prevent extravasation, or to maintain a channel for potential secondary surgeries. At the beginning of the 21st century, researchers introduced the concept of “tubeless PCNL,” which replaces the nephrostomy tube with internal drainage through a ureteral stent. A meta-analysis including 10 RCTs indicated that the stone-free rates were similar between patients who underwent traditional PCNL and those who had tubeless PCNL (RR = 1.05, 95% CI 0.96–1.14). 29 Tubeless PCNL can reduce the incidence of urinary leakage, decrease hospital stay, and lower the demand for analgesia. With technological advancements, the notion of “completely tubeless PCNL” has also been proposed, meaning that neither a nephrostomy tube nor a ureteral stent is placed after PCNL. In 2012, a randomized controlled study in children demonstrated that completely tubeless PCNL, compared with traditional PCNL, reduced postoperative hospital stay (39.54 ± 11.39 hours vs 58.7 ± 10.37 hours, p < 0.01) and analgesic use (0.07 ± 0.03 mg/kg vs 0.15 ± 0.04 mg/kg, p < 0.01), with no significant difference in postoperative complications (fever and leakage, p > 0.05). 30 In summary, for noncomplex cases after PCNL, it is feasible to attempt stent omission. For complex cases, such as those requiring secondary surgery for residual stones, intraoperative bleeding, solitary kidney, or coagulation disorders in children, it is recommended to place a nephrostomy tube or stent after PCNL.
Application of ureteral stents in acute renal obstruction
For obstructions caused by urinary tract stones, where primary stone removal is not feasible, emergency treatments such as internal drainage through stent placement or external drainage via percutaneous nephrostomy (PCN) are both viable options. Current guidelines do not specifically recommend one surgery over the other. Haleblian et al. believe that PCN provides better drainage effects in children with stones compared with stent placement, with more adequate drainage of purulent urine, shorter duration, and reduced exposure to radiation, analgesics, and antibiotics for children. 31 A meta-analysis of seven studies by Cardoso et al. found that stent placement and PCN are equally effective in the primary treatment of stone obstruction, with no significant difference in complications and less invasiveness. 32 Therefore, for acute renal obstruction caused by stones, it is recommended to choose between PCN and stent placement (ureteral stent placement for URL, PCN for PCNL) based on the needs of subsequent treatment. If the symptoms of obstruction are not significantly relieved after the placement of a ureteral stent, conversion to PCN may be considered.
Application of ureteral stents in laparoscopy/robotic-assisted stone treatment
Most pediatric urinary tract stones can be treated with ESWL and endoscopic techniques. However, in certain cases, open stone surgery is inevitable. Compared with adults, the need for open surgery for urinary tract stones in children is higher (2% in adults, 17% in children). 33 Currently, stent placement after pyelolithotomy is generally not performed, and whether to place a stent after ureterolithotomy remains controversial. Some researchers believe that stent placement after ureterolithotomy helps prevent ureteral stricture, while others believe that omitting the stent postoperatively is equally safe and effective. Srivastava et al. conducted a study on whether to retain a stent after laparoscopy ureterolithotomy in children and found that the stone clearance rate was 100% in both groups. 8 However, 12% of patients in the stent group had mild hematuria postoperatively, while 4.2% of patients in the unstented group had urinary leakage. The stent group also had a higher demand for postoperative analgesics and anticholinergic medications. 8 There are limited reports on laparoscopy lithotomy for pediatric urinary tract stones, and the author suggests that because of the impaction of stones causing local mucosal inflammation and edema of the ureter, to prevent postoperative ureteral stricture, it is recommended to retain a ureteral stent after surgery.
For children with hydronephrosis (caused by ureteropelvic junction obstruction [UPJO], neurogenic bladder, ureteral stricture, etc.) combined with urinary tract stones, the rate of stent retention after robotic-assisted laparoscopy lithotomy is high. Roth et al. retrospectively analyzed 26 cases of robotic-assisted laparoscopy pyelolithotomy, of which 77.8% of the children also underwent pyeloplasty, with a stent retention rate of 85.2% and a median stent retention time of 26 days. 34 Complications included one case of stent displacement and one case of urinary sepsis. Esposito et al. retrospectively analyzed 15 cases of robotic-assisted laparoscopy lithotomy, among which 73.3% had hydronephrosis and UPJO, 13.3% had neurogenic bladder, with a stent retention rate of 100% and a median stent retention time of 21 days, 33.3% of the children had hematuria and/or urinary tract infection postoperatively. 35 Most pediatric stones treated with robotic-assisted laparoscopy surgery are combined with other diseases, and there is limited research evidence. The rate of stent retention postoperatively is high, the duration of retention is long, but the incidence of stent-related complications is not high.
Stent-related complications and management
Ureteral stent-related complications include bladder irritation symptoms, urinary tract infections, stent migration, fracture, and encrustation. The application of magnetic stents and string stents in the treatment of pediatric urological diseases (ureteroscopy, ureteral reimplantation, and pyeloplasty) has been reported. The studies showed that magnetic stents are beneficial in reducing the need for anesthesia, secondary surgeries, medical costs, and surgical time, but they do not reduce stent-related complications. String stents are advantageous in reducing the time of anesthetics, invasive surgeries, and are more convenient for removal, but they do not decrease stent-related complications. 31 In 2003, Joshi et al. developed and validated the Ureteral Stent Symptom Questionnaire (USSQ) to assess symptoms associated with ureteral stents. 36 The questionnaire covers aspects including micturition, somatic pain, general health status, work performance, sexual function, and other areas, aiding in the clinical selection of different types of stents and the implementation of corresponding diagnostic and treatment measures. However, the assessment is hindered by the limited expressive ability of children, and the work performance and sexual function sections of the USSQ are not applicable to children. Currently, there is no symptom assessment scale specifically for children.
Bladder irritation symptoms and management
Symptoms of bladder irritation such as urinary frequency, urgency, dysuria, and difficulty in urination often trouble children and their families. Studies report that the incidence of bladder irritation symptoms is as high as 78%. These symptoms are mainly related to the stimulation of the bladder mucosa by the stent, particularly in the trigone area rich in nerve fibers. Some researchers have improved the distal structure of the stent to alleviate bladder irritation symptoms, such as fishtail stents and dual-durometer stents, which have to some extent alleviated bladder irritation symptoms, but there are limited reports in children. Since bladder irritation symptoms are similar to overactive bladder (OAB), some researchers have proposed using drugs that inhibit OAB to treat bladder irritation symptoms. Clinically, α1-receptor blockers such as tamsulosin and solifenacin are used to alleviate bladder irritation symptoms related to stents in children. In addition, the safety and efficacy of new drugs such as M3-receptor blockers such as tolterodine and β3-receptor agonists such as mirabegron in relieving bladder irritation symptoms have also been confirmed in adult studies. 37 Because of the late start of their use in children, coupled with the U.S. Food and Drug Administration’s restrictions on the safety of children’s medication, there is still absence of high-quality evidence.
Stent-related pain management
Pain is a major reason for children’s emergency visits. Studies have shown that lumbar pain is related to bladder–ureteral reflux, and the presence of the stent prevents the closure of the bladder–ureteral opening, causing urine to reflux during urination, leading to lumbar pain. Zhang et al. have shown that antireflux stents can partially prevent bladder–ureteral reflux but may cause more severe urinary symptoms. 38 Currently, there are limited reports on the application of antireflux stents in children. The author’s single-center experience draws a similar conclusion with Zhang, and we found that the rate of stent migration was higher in antireflux stent (5% in the antireflux stent group and 0% in the regular stent group, p < 0.05).
Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used analgesics in pediatrics, which can relieve pain with fewer side effects. Rove et al. explored the effect of preoperative NSAIDs on relieving pain related to stents in children, and the results showed no statistical significance (9.1% in NSAID vs 4.5% in placebo, p = 1.000). 39 The analgesic effect of NSAIDs is relatively weak, and some children need opioids to relieve stent-related pain. 40 Stent-related pain may be related to bladder irritation symptoms, and OAB-related drugs are also effective in relieving stent-related pain. Currently, there are limited high-quality studies on pain management related to stents in children.
Stent-related infections and management
Stent-related infections are a common complication of stent placement, which can lead to retrograde urosepsis and can be life-threatening in severe cases. It is related to bladder–ureteral reflux and the formation of bacterial biofilm. The bacterial biofilm on the stent has strong drug resistance and immune evasion, which is the main cause of clinically refractory infections. For the treatment of stent-related infections, some studies have reported that continuous antibiotic prophylaxis can reduce the incidence of febrile urinary tract infections in children for a short time. 41 However, a study showed that continuous low-dose antibiotic treatment during the stent placement period did not reduce the incidence of urinary tract infections and stent-related complications compared with only receiving perioperative antibiotic prophylaxis. 42 How to effectively prevent and treat stent placement-related infections is still a clinical problem that needs to be solved urgently.
Stent migration and management
Stent migration is a rare complication. The incidence of stent migration in adults is 0.6% to 3.5%. Since there are only case series reports on stent migration in children, the real incidence is still unclear. Some scholars have studied the impact of stent length on stent migration and found that shorter stents are more prone to migration. 43 Therefore, it is necessary to calculate the reasonable retention length of the stent to avoid stent migration while reducing the bladder irritation symptoms caused by the stent being too long. The length of the stent can be calculated precisely by imaging. For children, a simple calculation method is age + 10 cm. 44 The size of the stent does not affect the incidence of stent migration, but the smaller size can reduce urinary symptoms and patient-reported pain. 45 The migrated stent is difficult to play a normal role in drainage and support and may cause damage to the urinary system, so it needs to be removed as soon as possible. Based on the author’s single-center experience, for pediatric patients, stent sizes are generally less than 5F, and it is unusual to place two ureteral stents within the same ureter on one side.
Stent encrustation and management
Ureteral stent encrustation refers to the accumulation of mineral crystals within the lumen and/or on the surface of the stent, with an occurrence rate of 13%. Currently, there is no standardized treatment protocol. Crystal deposition can impede the drainage of urine and may interact with the urothelium of the ureter, leading to ureteral damage. The management of encrusted stents is complex, and the cost of treatment is, on average, 6.9 times that of the standard stent removal surgery. 46 Therefore, it is crucial to determine the degree of stent encrustation and formulate corresponding therapeutic strategies.
The key risk factor for stent encrustation is the duration of stent indwelling. Kawahara et al. reported that the encrustation rate of the stent was 56.8% at 6 to 12 weeks and 75.9% thereafter. 47 The role of bacterial biofilm in encrustation remains controversial, with some studies suggesting that biofilm is a major cause of encrustation. Some other researchers, by comparing the total mass of biofilm, bacterial load, and stone composition analysis with stent-related symptoms, found that the role of biofilm in encrustation is limited. The mechanism of stent encrustation is not fully understood and may be related to increased levels of urinary minerals (such as calcium, oxalate, and phosphorus) leading to spontaneous encrustation; urease-producing bacteria (such as Proteus, Pseudomonas, and Klebsiella) break down urea to produce ammonia, increase urine pH, and promote the crystallization of calcium phosphate and magnesium phosphate. 46
Children with encrusted stents may exhibit pain, crying, and reluctance to urinate. Clinically, initial screening for stent encrustation can be done using X-ray to visualize the thickness and uniformity of the stent. CT can clearly identify the location of encrustation and grade the severity, which is considered the “gold standard” for diagnosing stent encrustation. Encrusted stents need to be removed immediately to prevent further enlargement leading to obstruction, urinary tract infection, and other complications. Studies have reported that encrusted stents can be removed in one surgical surgery, but for complex cases, multiple surgeries may be required, and a new stent may be placed at the end of the surgery. Encrustation stent grading systems, such as the Forgotten, Encrusted, Calcified grading system (Table 2) and the Visual Grading System for Ureteral Encrustation Stents classification system (Table 3), help clinicians assess the difficulty of treatment and choose appropriate therapeutic strategies. 48
Forgotten, Encrusted, Calcified Stent Grading System
Visual Grading System for Ureteral Encrustation Stents Classification System
Combined access: endoscopic combined intrarenal surgery and PCNL plus cystolithotripsy or semirigid ureteroscopy.
PCNL = percutaneous nephrolithotomy.
Some researchers have reported single-center management approaches for encrusted stents. Dinesh et al. described a method for removing encrusted stents using a ureteral access sheath: first, the bladder end of the stent is removed from the urethra, then the stent is inserted into the access sheath closure device, and the closure device is advanced forward to strip off the encrustation and maintain the ureteral passage. 49 However, this method requires completion under X-ray fluoroscopy, increasing the radiation exposure to the child. Lukies et al. improved this method based on Dinesh’s approach, allowing for the simultaneous removal of the encrusted stent and replacement with a new stent. 50
In pediatric patients, there is also the phenomenon of encrustation because of forgotten long-term stent retention. To reduce encrustation because of forgetting, physicians should provide adequate health education to patients, inform them of the timing for stent removal or replacement, and the consequences of forgetting the stent, to gain the active cooperation of parents. In addition, mobile software and electronic medical record tracking can be used to remind both medical staff and patients to remove the stent in a timely manner.
Conclusions
Ureteral stents are an essential tool in the treatment of pediatric urinary tract stones. For uncomplicated cases, ureteral stents are not routinely placed before or after surgery for pediatric urolithiasis. For complex cases involving intraoperative ureteral injury, ureteral stricture, solitary kidney, or renal function impairment, stents are selectively placed. Novel ureteral stents show promise for their application because of their potential to reduce stent-related complications and avoid secondary anesthesia. Currently, there is still absence of research on the use of ureteral stents in pediatric urolithiasis, more high-quality, multicenter pediatric clinical studies are needed in the future to provide evidence-based support for the application of ureteral stents.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data