
Abstract
Purpose:
Ureteral wall thickness (UWT) was proposed as a potential predictor for spontaneous stone passage (SSP). In earlier studies, the effect could not be isolated from stone size. Accordingly, we sought to determine whether UWT, alone or combined with stone size, could enhance SSP predictability.
Material and Methods:
In total, 199 patients with acute renal colic and a single ureteral stone visible on noncontrast computerized tomography (NCCT) who opted for SSP were prospectively enrolled. A reviewer, blinded to the enrollee’s stone passage status, analyzed NCCTs for both stone metrics (linear measurements, area, volume, density) and ureteral parameters (UWT at the point of greatest soft-tissue thickness, location, hydronephrosis). Logistic regression models were used to evaluate the relationship between these factors and SSP.
Results:
In a univariate analysis, longer (odds ratio [OR] = 0.285; 95% confidence interval [CI]: 0.375–0.608), wider (OR = 0.477; 95% CI: 0.375–0.608), denser (OR = 0.997; 95% CI: 0.995–0.998) stones with larger surface areas (OR = 0.920; 0.890–0.951), larger volumes (OR = 0.984; 95% CI: 0.977–0.990), and greater depth (OR = 0.538; 95% CI: 0.427–0.676), as well as those surrounded by a thicker UWT (OR = 0.665; 95% CI: 0.504–0.878), were less likely to pass spontaneously. In a multivariate analysis, UWT actually lost its significance. Indeed, in the multivariate analysis, only the largest linear stone measurement retained significance (OR = 0.454; 95% CI: 0.343–0.600).
Conclusion:
Although significant in a univariate analysis, in a prospective cohort study that adjusted for stone size, UWT lost significance in the multivariate model. SSP of a ureteral calculus was best predicted by its maximum linear measurement.
Introduction
Acute renal colic (ARC) is one of the most common emergency department (ED) discharge diagnoses. 1 Observation/expectant management for 4–6 weeks (approximately 40 days) after initial ARC presentation is currently recommended by both the American and European Urological Association guidelines for the management of uncomplicated ARC. 2,3 Nevertheless, although some patients do not meet the criteria for emergent intervention (i.e., fever >38°C, acute kidney failure, obstructed single kidney, active urinary tract infection, or sepsis), they would benefit from earlier intervention if those with a poor chance of spontaneous stone passage (SSP) could be more clearly identified. 4
Notably, neither the European nor the American urological associations have delved into the potential contribution of radiomic predictors for SSP other than stone size. In the context of wide adoption of NCCT as an essential tool for managing ARC in the ED, the concept of measuring NCCT ureteral wall and surrounding pericalculus edema was met with significant interest. With a normal cross-sectional thickness of 0.95–2 mm, the 65 ureteral wall adjacent to the stone becomes edematous, with histological changes such as 66 interstitial fibrosis and muscular hypertrophy noted. 5 –8
However, as highlighted by Dean et al. in a recently published meta-analysis, the effect of stone size, an important confounding variable, could not be completely removed from the analysis, and thus the absolute value of ureteral wall thickness (UWT) remains in question. 9 These earlier publications recommended that future studies control for stone size to determine whether the two metrics are confounding or truly correlated. 9 Accordingly, we sought to assess how UWT alone, stone size alone, or the two measurements together affect the predictability of SSP in a prospective, adequately powered, observational cohort study.
Materials and Methods
Study population
The protocol for our prospective, observational, single-center study was approved by our Institutional Review Board. Results are presented in accordance with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines. 10
Between November 2020 and August 2023, 250 patients presenting with ARC to our ED, who had a single ureteral stone visible on NCCT and who opted for a trial of SSP, were enrolled in this study. All CT scans were performed within 24 hours of ED presentation at the time of the acute episode of renal colic. Inclusion and exclusion criteria are presented in Table 1.
Inclusion and Exclusion Criteria
ARC = acute renal colic; NCCT = noncontrast computerized tomography.
Study variables
Variables were selected a priori based on potential correlations with SSP based on the peer-reviewed published literature and their availability in clinical practice based on the enrollee’s NCCT. UWT, the primary variable of interest, was determined in a soft-tissue window according to the Yoshida method as “the point of greatest soft-tissue thickness (ureteral wall ± periureteral edema) around the circumference of the stone; this evaluation ranged from the top to the top of the stone” (Fig. 1). 11,12 Secondary variables included other stone and ureteral radiological metrics. NCCT images were assessed in all planes by a reviewer physician who was blinded to the patient’s group (SSP or intervention).
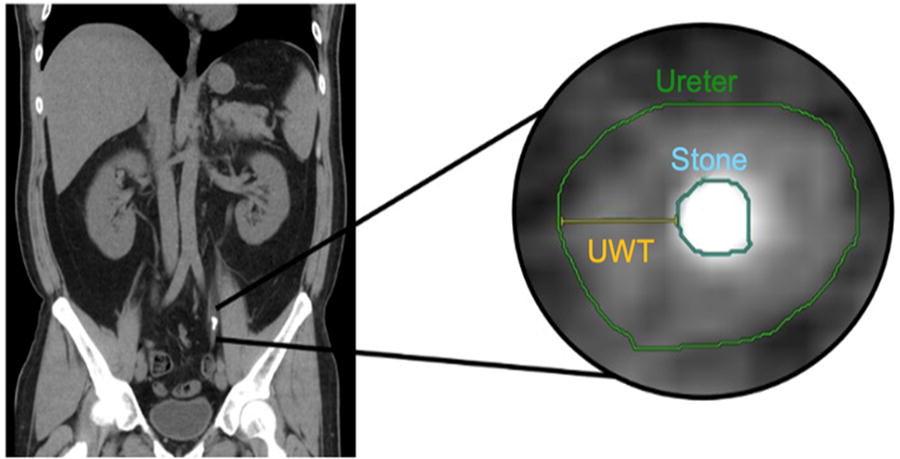
Visual representation of the methodology employed to measure the UWT around the stone’s circumference. AUC = area under the curve; UWT = ureteral wall thickness.
Upon evaluation of the stone bed from the top to the top of the stone on the axial plane, stone area was calculated at the point of maximal stone surface. Stone length (a) was defined as the maximum longitudinal stone diameter on coronal view, whereas stone width (b) and stone depth (c) corresponded to the maximum transverse and anteroposterior diameters on axial and sagittal views, respectively. The three-dimensional (3D) stone volume was determined using an open-source segmentation software (3D Slicer®) by an experienced reviewer (200+ hours using the software), who had been previously validated as a reliable reviewer by comparing their segmentation of 98 stone-bearing kidneys with segmentations on the same NCCT by a board-certified radiologist, a fellowship-trained endourologist, and an endourology fellow (interclass correlation coefficient = 0.99). 13 Stone shape was assessed according to Finch’s “best-fit” ellipsoid shape as follows: scalene ellipsoid (the three dimensions of the stone are unequal, a > b > c), oblate spheroid (the stone has the shape of a disk, with a = b > c), or prolate spheroid (the stone has a rugby ball shape, with a = b < c). 16
Stone location was defined as “proximal” if the stone was located caudal to the renal pelvis but cranial to the iliac crest, as “mid” if the stone was between the iliac crest and the sacroiliac joint overlying the sacroiliac joint, or as “distal” if the stone was located caudal to the sacroiliac joint. Ureteropelvic (i.e., ureter seen just distal to the stone, rather than having ureter both above and below the stone) and stones lodged in the ureteral tunnel were excluded from the analysis because of difficulty in accurately assessing the surrounding UWT in the former case and difficulty in assessing UWT in the latter case plus the likelihood of these distal stones passing spontaneously.
The presence of hydronephrosis was evaluated both as a binary variable (“yes” or “no”) as well as a multinomial variable (0—no hydronephrosis; 1—mild; 2—moderate; 3—pronounced; 4—massive). The average, central, and peripheral stone densities were measured in Hounsfield units.
Study outcomes
The primary outcome was SSP, assessed at least 40 days after presentation. Only patients with a confirmation of SSP by repeat imaging, physical stone collection, or negative ureteroscopy were included. The secondary endpoint of our study was stone impaction. This was defined as a failure to pass a 0.035-inch glidewire or a 5F open-ended catheter at the time of the initial retrograde attempt.
Statistical analysis
The statistical analysis was performed using IBM SPSS Statistics version 29.0.0.0 (IBM Corp, Armonk, NY). Continuous variables were described using means/standard deviations for normally distributed data and medians/interquartile ranges for nonnormal distributions. Normal distribution was assessed by performing the Kolmogorov–Smirnov test. Statistical analysis of normally distributed continuous data was completed using two-tailed unpaired sample t-tests. Categorical variables were presented as percentages, and chi-square testing was used to assess for any associations between the test variable and the outcome. Univariate and multivariate binary logistic regressions were employed to determine correlations between the aforenoted variables and SSP.
Results
Baseline clinical and radiological differences between the SSP and early intervention groups are summarized in Table 2. After up to 40 days of trial of passage, SSP was observed in 78 (39.20%) patients, whereas in 121 (60.80%) patients, SSP did not occur, and the patients proceeded to have a surgical intervention. SSP was confirmed by imaging in 50 cases (64.10%), by physical stone collection in 22 cases (28.21%), and by negative ureteroscopy in 6 cases (7.69%).
Patient Characteristics Stratified by Group (Spontaneous Stone Passage vs Early Intervention)
p-Values were compiled by employing two-tailed unpaired sample tests for continuous variables and chi-squared tests for categorical variables.
BMI = body mass index; HU = hounsfield unit.
Upon multiple unadjusted simple binary logistic regression analyses, various stone characteristics were correlated with a reduced likelihood of SSP. Longer, wider, denser stones with larger surface areas, volumes, and depth, as well as those surrounded by a thicker UWT were less likely to pass spontaneously (Table 3). Although stone location did not reach statistical significance, there was a notable trend suggesting distal ureteral stones may pass more easily than proximal ones (p = 0.086). Moreover, an increased ureteral wall inflammation and pericalculus edema on NCCT increases the likelihood of the stone being impacted (OR = 1.418; 95% CI: 1.038–1.936, p = 0.028).
Correlations Between Risk Factors and Spontaneous Ureteral Stone Passage as Assessed by Univariate Binary Logistic Regression Models
CI = confidence interval; OR = odds ratio; UWT = ureteral wall thickness. p- values were deemed statistically significant; p < 0.05.
A receiver operating characteristic (ROC) analysis was conducted to evaluate the predictive performance of the variables identified as significant based on the univariate analysis. Stone length, width, and depth demonstrated comparable predictive performance, emerging as the most reliable predictors of SSP, with respective area under the curve (AUC) values of 0.86, 0.85, and 0.83. Conversely, UWT exhibited the lowest predictive capability (AUC = 0.64) (Fig. 2).
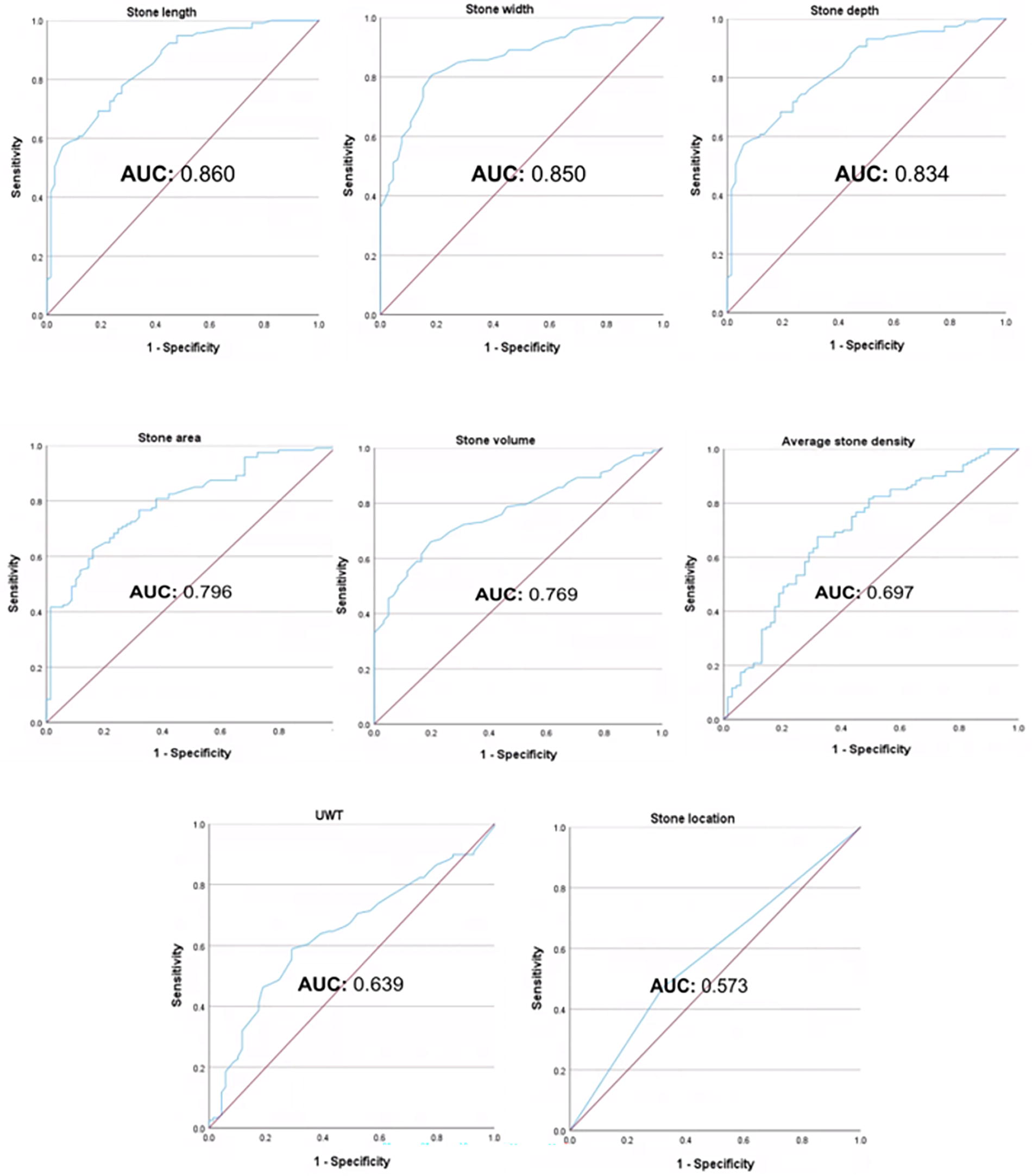
Receiver operating characteristic (ROC) curve for stone metrics that were found to be statistically significant predictors of spontaneous stone passage upon multiple unadjusted binary logistic regression analyses.
Given the potential correlation among linear stone metrics, stone area, stone volume, and resulting UWT, the multicollinearity among significant univariate predictors was assessed using Spearman correlation coefficients (rho). Since the linear stone measurements are highly correlated with one another as well as with stone area and volume (rho > 0.85), we opted to include only the maximum linear stone measurement as a potential predictor in the multivariate analysis. Notably, there was minimal correlation between linear measurements and pericalculus edema and UWT (rho < 0.45) (Table 4).
Multicollinearity Assessment After Univariate and Multivariate Binary Logistic Regression Models
Each cell represents the bivariate Spearman correlation coefficient (Spearman rho) value between the variable on each row and each independent column.
Upon a multivariable logistic regression (MVLR) analysis, only the largest linear measurement (OR = 0.454; 95% CI: 0.343–0.600) retained statistical significance for predicting SSP (Table 5). Subsequently, a predictive model for SSP stratified by maximum linear stone measurements was formulated (Fig. 3). Upon applying Youden’s criteria of identifying an optimal cutoff that maximizes both sensitivity and specificity, a threshold value of 5 mm maximum linear stone length was determined (sensitivity: 0.798; specificity: 0.771).
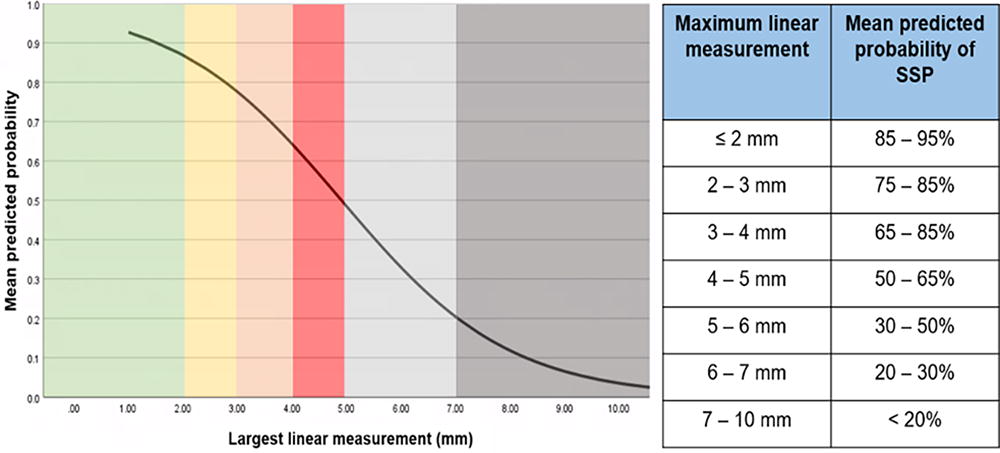
Mean predicted probability of spontaneous stone passage (SSP) stratified by maximum linear stone length (mm).
Correlations Between Risk Factors and Spontaneous Ureteral Stone Passage as Assessed by a Multivariate Logistic Regression Analysis Model
Upon comparing SSP rates between the subgroups of patients who did not receive tamsulosin and those who did, irrespective of stone size, it was found that the tamsulosin group exhibited statistically significantly higher SSP rates. The benefit was greater among 5–10 mm stones as compared to those with <5 mm stones, with a 37.14% increase in SSP rates for stones ≥5 mm and a 19.16% increase for stones <5 mm (Fig. 4). Although we were able to confirm a statistically significant association between tamsulosin use and higher SSP rates, it is important to note that the current study may be underpowered to comprehensively assess the correlation between tamsulosin use and SSP rates in an MVLR.
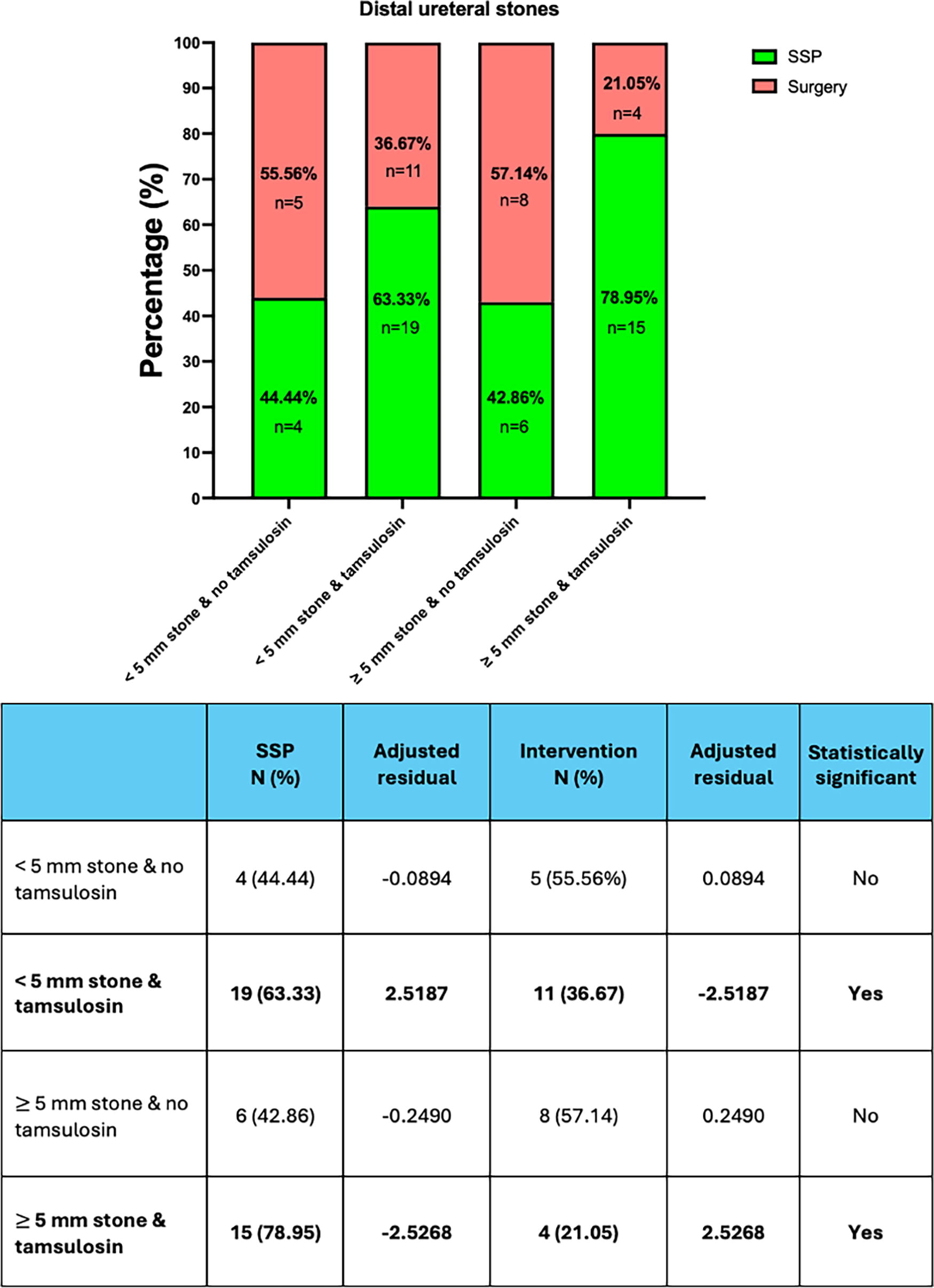
Association analysis between distal ureteral urolith’ SSP rates and tamsulosin use. A statistically significant increase in SSP rates for the <5 mm stone and tamsulosin group as well as for the ≥5 mm stone and tamsulosin group (both adjusted residuals larger than 2.49771 or less than −2.49771) were noted.
Discussion
An impacted stone, by its disruption of the urothelial layers, serves as an inflammatory promoter, leading to fibrinous exudate production over the traumatized area and adhesion formation across the distal opposing walls of the urothelium. 7,8 In the acute setting, this pericalculus inflammation and edema can interfere with the likelihood of the ureteral stone passing spontaneously. 7,8 Accordingly, the concept of measuring NCCT UWT was met with significant interest both for the surgeon, in terms of fast-tracking the procedure and for patients in establishing realistic SSP expectations. 10,12,13,15 –19
Recognizing the subjective nature of stone impaction, we aimed to mitigate confirmation bias by adopting a more conservative definition for impaction. 9,12,19 Specifically, we defined impaction as the failure to pass either a 0.035-inch glidewire or a 5F open-ended catheter upon initial retrograde attempt. Even with this conservative criterion, our data corroborated the predictive value of UWT for stone impaction (OR = 1.418; p = 0.028).
Additionally, we were able to confirm, through a univariate logistic regression analysis that stones surrounded by a thicker ureteral wall are associated with a decreased likelihood of SSP (OR = 0.665; 95% CI: 0.504–0.878). 11,18,20 –23 Furthermore, our data confirm that longer, wider, and denser stones, with larger surface areas and volumes, are less likely to pass spontaneously. We also corroborated earlier studies suggesting that distal stones trended toward a higher SSP than proximal ureteral calculi. 25 –27 Despite these findings which were confirmatory with other published data, we unexpectedly found that upon conducting an MVLR analysis, in which we accounted for all relevant confounders, UWT no longer correlated with SSP.
Our failure to corroborate earlier studies extolling the value of UWT may largely be because of variations in those studies including study design, a smaller cohort size, retrospective reviews, and different statistical methodologies (Table 6). Notably, retrospective studies are susceptible to confirmation bias. Additionally, in small cohorts, with fewer than 10 events per tested variable, the chance of the analysis reflecting the idiosyncrasies of the dataset, a phenomenon termed model overfitting, is likely, particularly when employing MVLR models. 26,27 In turn, this leads to a reduced generalizability of the predictors.
Comparison of Previous Studies Assessing the Impact of Ureteral Wall Thickness on Spontaneous Stone Passage
SSP = spontaneous stone passage; WBC = white blood cell; CRP = C reactive protein.
Only two prospective studies assessed UWT and SSP through MVLR analysis. 18,23 Samir et al. found that only UWT and hydronephrosis grade influenced SSP2; however, their model was constrained by its design which limited study inclusion to stones in the distal ureter that were between 5 and 10 mm in size. 23 In the study conducted by Selvi et al., their primary aim was to assess other nonestablished predictors for SSP such as the Framingham cardiovascular risk score. 18 In their study they adjusted for the difference in longitudinal and transverse stone dimensions between the SSP and intervention groups; thus the specific effect of stone size on SSP was not fully assessed by the MVLR model. 18
As highlighted by Dean et al. in their meta-analysis, the effect of UWT could not be fully isolated from that of stone size. 9 Our prospective cohort study specifically addressed this limitation. From a univariate perspective, as assessed by the ROC curves, the effect of UWT fades in comparison to that of stone size. This mirrors the findings of Jendeberg et al., where both stone length and stone width displayed essentially equivalent power for SSP success (AUC: 0.86 and 0.85, respectively). 24 Moreover, despite observing a weak correlation between stone size and UWT (rho < 0.5), UWT lost its statistical significance when incorporated into the same MVLR model as the maximum linear stone measurement. This suggests that stone size and UWT are confounding rather than correlated parameters, with the effect of UWT on SSP overshadowed by linear stone measurements. One explanation for this observation is that a larger stone might become more readily impacted and thereby trigger a more robust inflammatory response, leading to ureteral edema and smooth muscle hypertrophy seen on the NCCT as an increase in UWT. Clearly, though the stone came before the increase in UWT and thus our study, not surprisingly, has shown the superiority of stone linear measurements in predicting SSP rather than UWT.
Furthermore, the previously noted meta-analysis acknowledges there was a wide variation of UWT optimal cutoffs, ranging from 1.8 to 5.3 mm (mean: 3.1 mm). 10 This highly heterogeneous UWT range could, in part, be attributed to a higher interobserver variability. This is in concert with multiple studies that have shown inaccuracies when it comes to linear stone measurements; the mean interobserver variability was 26.2% among three board-certified radiologists who measured the maximum linear dimension of the same stone, 28 a level of variability corresponding to an average measurement error of 1.2–1.9 mm. 29 In contrast, identifying the dense stone borders proves a considerably easier and more precise endeavor. This raises the warranted concern regarding the accuracy and precision of UWT readings across different reviewers.
Indeed, our study would suggest that a maximum linear measurement of 5.1 mm is the optimal predictor of stone passage (sensitivity: 0.798; specificity: 0.771). These data correlate with previous studies assessing the mean size of the human ureter (14.92F, 4.75 mm diameter) and might explain why the SSP rates drop precipitously as soon as any of the three linear stone dimensions exceeds 5 mm. 30
What is much needed, however, is a standardized artificial intelligence program to assess stone size in order to eliminate the observer variability in stone measurements. Consequently, this improved accuracy in stone sizing could lead to more dependable SSP predictions, and thereby facilitate more expeditious judgment with respect to immediate intervention vs a trial of passage.
Our study bears some limitations. Although a prospective study, the data were observational. As the urologists initially assessing the patient were not blinded to the stone’s linear measurement, there is also possible clinical bias. Some physicians may indeed have a lower threshold for intervention. To address this, the trial of passage period was fixed for at least 40 days. Although we ensured that the CT scans were completed shortly after ED presentation with ARC, we are unable to control for the exact timing from initial symptom onset prior to the ED visit. One plausible explanation for our findings could be the exclusion of patients with intramural or ureteropelvic junction stones and is thus a further limitation of our study. Additionally, our study’s measurements were performed manually by an experienced 3D Slicer® reviewer. In the future, fully automated artificial intelligence (AI)-enabled software could eliminate human error and produce more accurate results and thus better guidance for clinical decision-making.
Conclusion
In a prospective cohort study, the chances of a ureteral stone spontaneously passing were best predicted by linear stone measurements (i.e., stone length, width, or depth). Albeit significant in univariate analysis, UWT lost its significance in a multivariate model, suggesting that the initial correlation was likely confounded by stone size. Moreover, in concert with earlier publications, the optimal predictor of successful or failed stone passage is a maximal linear measurement of 5.1 mm.
“We shall not cease from exploration, and the end of all our exploring will be to arrive where we started.”
T.S. Eliot, “Little Gidding” (1942 poem, from Four Quartets)
Authors’ Contributions
Conception and design: R.V.C., R.M.P., J.L., and A.D.C. Data analysis and interpretation: B.C., T.N.V., C.M.T., W.-p.C., K.V., R.B., and A.D.C. Data acquisition: B.C., T.N.V., C.M.T., K.V., R.B., A.D.C., B.M.G., and Z.E.T. Drafting article: B.C., T.N.V., C.M.T., K.V., A.D.C., Z.E.T., B.M.G., and R.V.C. Critical revision of the article: A.D.C., B.C., T.N.V., C.M.T., Z.E.T., B.M.G., R.M.P., P.J., J.L., and R.V.C. Statistical analysis: W.-p.C., A.D.C., T.N.V., and C.M.T. Supervision: R.V.C., J.L., R.M.P., P.J., Z.E.T., and B.M.G.
Ethics Statement
All human subjects provided written informed consent with guarantees of confidentiality.
Authors’ Disclosure Statement
The authors have no conflicts of interest to disclose.
Footnotes
Funding Information
This research received no external funding from any funding agency in the public, commercial, or not-for-profit domains.