
Abstract
Introduction and Objective:
Increased intraocular pressure (IOP) during robot-assisted radical prostatectomy (RARP) is known to occur and may cause in rare cases anterior ischemic optic neuropathy. In this study, we evaluated the impact of abdominal insufflation pressures on IOP during RARP in a cohort of patients undergoing RARP.
Methods:
Patients undergoing RARP were recruited for this Institutional Review Board-approved study from January 2019 to October 2022 at our Center. IOP was measured for both eyes using a Tonopen (Reichert, Buffalo, NY) at six time points (T1−T6); preoperatively, in the operating room in supine position under anesthesia without insufflation, at 30ο Trendelenburg position (T position) without insufflation, at Trendelenburg position with abdominal insufflation at 10 mm Hg, 15 mm Hg, and 20 mm Hg. A mixed effects model was applied to analyze changes in IOP with changes in insufflation pressure, while controlling for age, body mass index (BMI), and systolic blood pressure.
Results:
For a total of 28 patients, the mean age and BMI were 61.2 ± 7.4 (SD) years, and 29.0 ± 4.6 kg/m2, respectively, while the mean systolic blood pressure was 128.1 mm Hg ± 17.0 mm Hg. The mean IOP at six time points increased from 13.6 mm Hg to 26.8 mm Hg, whereas the mean systolic blood pressure ranged from 132.1 (±17) mm Hg to 130.9 (±18) mm Hg from time points 1–6. On a mixed-effects model, a change in 1 mm Hg of abdominal insufflation pressures was associated with a 0.35 mm Hg increase in IOP (95% confidence interval [CI] = 0.29–0.4) holding all other variables constant. Furthermore, a 1 mm Hg change in systolic blood pressure was associated with a 0.06 mm Hg increase in IOP (95% CI = 0.03–0.09).
Conclusion:
Our findings suggest that intra-abdominal insufflation pressure and systolic blood pressure are significantly associated with IOP during RARP after accounting for the correlation of the repeated measures and controlling for age and BMI.
Introduction
Robot-assisted radical prostatectomy (RARP) is the gold standard management option for localized prostate cancer (PCA) and offers benefits such as minimized blood loss, reduced surgical complications, improved functional results, and a diminished duration of hospitalization. 1,2 RARP necessitates the patient’s placement in an exaggerated Trendelenburg posture (head lowered to upward of 30ο) combined with pneumoperitoneum usage. 3,4 While the Trendelenburg position pushes the abdominal contents upward toward the thorax, abdominal insufflation lifts the anterior abdominal wall upward. 4 These maneuvers create sufficient room for robotic arms to operate, however, in rare cases, they can lead to adverse physiological effects on the circulatory system, respiratory system, neurological system, and hemodynamic stability in general. 3,5 –8 These changes can subsequently result in conditions such as limb nerve damage, swelling of the face, and multiple eye-related complications. 3 In addition, intraocular pressure (IOP), the central point of this investigation, changes during RARP. Included among the ophthalmic complications is ischemic optic neuropathy (ION), which while uncommon, can be particularly devastating when encountered. 9 ION is due to a decrease in perfusion of the optic nerve and is attributed to a surge in IOP during these cases. 10 The impact of the Trendelenburg positioning has shown a substantial increase in IOP in prior studies. 8 However, the impact of abdominal insufflation pressure on IOP changes during RARP is least explored. 11 Given this backdrop, our research aimed to evaluate the association of changes in intra-abdominal insufflation pressures in the Trendelenburg position on IOP shifts in a prospective cohort of patients undergoing RARP at our facility.
Materials and Methods
From January 2019 to October 2022, among the patients scheduled for RARP at the University of Maryland Medical Center, a total of 28 patients were recruited for this study. The study was approved by the Institutional Review Board (IRB) at our institution and informed consent was obtained from all the participating patients. In this study, one surgeon performed the 26 RARPs for PCA and two robot-assisted simple prostatectomies (for benign prostatic hyperplasia) in a standard fashion, using the DaVinci system (Intuitive Surgical, Sunnyvale, CA, USA). Patients with pre-existing glaucoma, retinal vascular diseases, and a history of eye operation were not recruited. IOP was measured using Tonopen (Reichert, Buffalo, NY) for all 28 participants at six different time points. IOP measurements were taken by the two urology research fellows who were trained and certified by an ophthalmologist at the same medical center for using Tonopen. The six IOP measurement time points (T1–T6) were in preoperative room (T1), in the operating room after anesthesia induction in supine position without insufflation (T2), in Trendelenburg position at 30ο head tilt (T position) without insufflation (T3), at Trendelenburg position with abdominal insufflation at 10 mm Hg (T4), 15 mm Hg (T5), and 20 mm Hg (T6).
IOP for each eye was measured and then an average IOP of both eyes was calculated and used as the unit of analysis. Patients’ blood pressure was collected for each time point while abdominal insufflation pressures was measured for time points T3−T6. An opening intra-abdominal pressure was measured after the T2 time point (i.e., in supine position and under anesthesia) but before T3 time point; however, we assigned the opening pressure of abdominal pressure to the T3 time point. Afterward, abdominal insufflation pressure was increased to 10 mm Hg (T4), 15 mm Hg (T5), and 20 mm Hg (T6), and corresponding IOP measurements were taken. Preoperatively, the patient’s age, BMI, serum Prostate Specific Antigen (PSA) at diagnosis, clinical and pathological tumor stage, Gleason score at biopsy, and prostate size were recorded.
Statistical analysis
An exploratory data analysis was performed for the association between IOP and abdominal insufflation pressure. In the next step and given the repeated measures nature of the data, we applied a mixed effects model, validated by the Shapiro−Wilk test, to analyze changes in IOP with changes in abdominal insufflation pressure, while controlling for age, BMI, and systolic blood pressure. Variance inflation factor was employed to check for multicollinearity between covariates. The mixed-effects model provided estimates for the fixed effects (i.e., the independent variables) and the random effects (i.e., the variability between patients). All statistical analyses were performed using Stata 18.0 software (CA, USA), and p values < 0.05 were considered significant. Likelihood-ratio test was employed for model selection between the linear regression model without random effects and the mixed effects model. The chi-square test was utilized to check for significance.
Results
The preoperative baseline clinicopathological characteristics of the 28 men recruited and analyzed in this study are shown in Table 1. The mean (±SD) age of the patients was 61.2 (±7.4) years, and the mean (±SD) BMI was 29.0 (±4.6) kg/m2 (shown in Table 1). The mean (±SD) systolic blood pressures were 132.1 (±17) mm Hg, 111.85 (±16) mm Hg, 117.88 (±12) mm Hg, 131.1 (±16.8) mm Hg, 132.1 (±12.2) mm Hg, and 130.9 (±18.8) mm Hg, for six time points T1, T2, T3, T4, T5, and T6, respectively.
Clinical Characteristics and Demographics of the Patients Undergoing Robot-Assisted Radical Prostatectomy
BMI, body mass index; SD, standard deviation; BPH, benign prostatic hyperplasia.
The mean (±SD) IOP values corresponding to each of the six time points T1, T2, T3, T4, T5, and T6 were 13.6 (±3.7) mm Hg, 10.9 (±3) mm Hg, 20.6 (±3.9) mm Hg, 24.2 (±4.2) mm Hg, 26.0 (±4.4) mm Hg, and 26.8 (±4.3) mm Hg, respectively as shown in Figure 1. Figure 1 also illustrates a positive correlation between mean IOP and six time points, specifically with abdominal insufflation pressure. Compared with baseline mean IOP at T1, there is an initial decline in IOP of 2.7 mm Hg as an effect of anesthesia at T2. However, Trendelenburg position at 30° (T3) increases the mean IOP by 7 mm Hg. Afterward, as we increased the abdominal insufflation pressure, mean IOP increased by 10.6 mm Hg at 10 mm Hg of abdominal insufflation pressure (T4), by 12.4 mm Hg at 15 mm Hg of abdominal insufflation pressure (T5) and by 13.2 mm Hg at 20 mm Hg of abdominal insufflation pressure (T6) compared with baseline mean IOP at T1. On an analysis of percent change in mean IOP at different time points (T2–T6) compared with T1, it is observed that 56.33% rise in mean IOP correlates with Trendelenburg position, and that this gradually increases to a 102.56% increase in IOP with insufflation (at T6), showing the nearly equal contribution of position and insufflation with change in IOP.
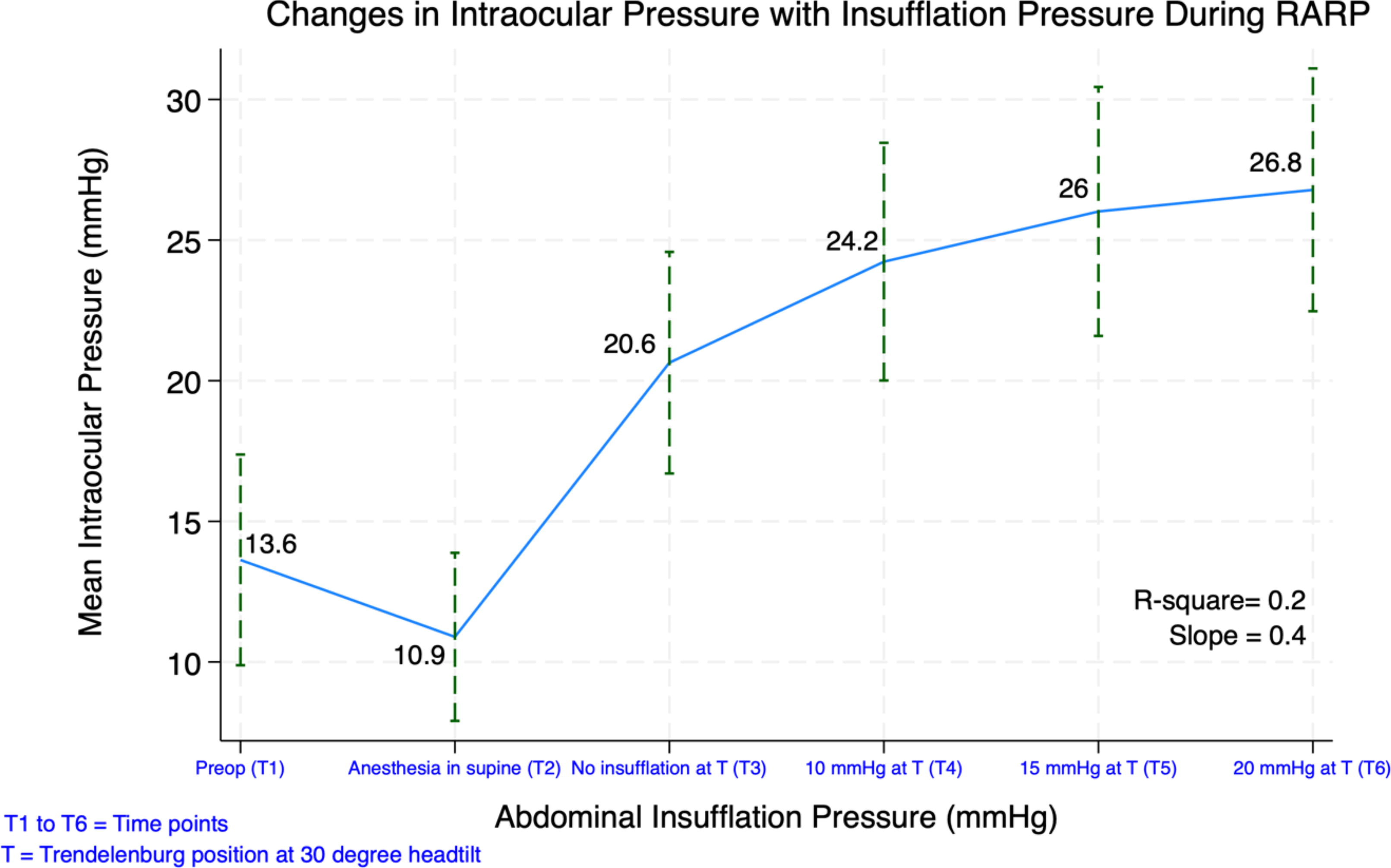
Change in intraocular pressure with change in abdominal insufflation pressure at six time points: in the preoperative room (T1), in the operating room after anesthesia induction in supine position without insufflation (T2), in the Trendelenburg position at 30ο head tilt (T position) without insufflation (T3), at the T position with abdominal insufflation at 10 mm Hg (T4), 15 mm Hg (T5), and 20 mm Hg (T6). Error bars represent standard deviation around the mean IOP. Slope and R 2 are only for T3–T6 and do not account for the IOP at T1 and T2. IOP = intraocular pressure.
On a simple linear regression, an R 2 value of 0.2 suggests that abdominal insufflation pressure can account for about 20% of the observed variability in IOP, shown in Figure 2. The quantitative impact of this relationship is further emphasized by a slope of 0.4, suggesting a significant increase in IOP for each unit increase in abdominal insufflation pressure.
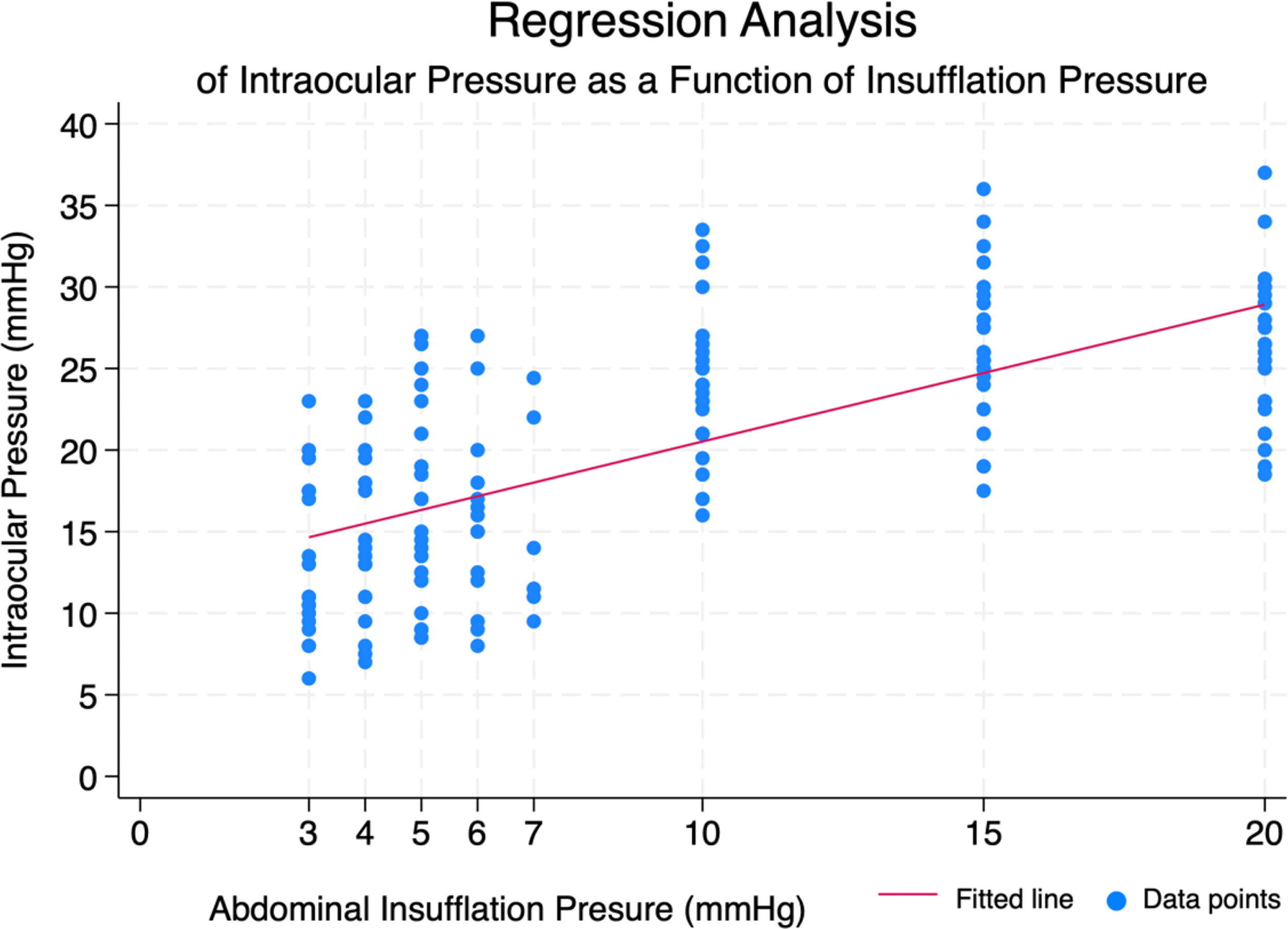
Simple linear regression of change in intraocular pressure as a function of abdominal insufflation pressure applied for four time points T3, T4, T5, and T6 corresponding to abdominal opening pressure, abdominal insufflation pressure at 10 mm Hg, 15 mm Hg, and 20 mm Hg, respectively.
We applied a mixed-effects method for IOP measurements at four time points T3, T4, T5, T6, and validated by Shapiro−Wilk test (to assess normal distribution of the data, p = 0.821). It showed that a change in 1 mm Hg of abdominal insufflation pressure was associated with a 0.35 mm Hg increase in IOP (95% CI = 0.29–0.40, p < 0.001) holding all other variables constant (Table 2). Furthermore, as observed among patients, 1 mm Hg increase in systolic blood pressure was associated with a 0.06 mm Hg increase in IOP (95% CI = 0.03–0.09, p < 0.001). Age and BMI were statistically not associated with IOP. The mixed-effects model provided a significantly better fit to the data than a simpler linear regression model without random effects, indicated by a chi-square value of 121.11 and a p value of <0.0001.
Mixed-Methods Model: Effect of Abdominal Insufflation Pressure on Intraocular Pressure (mm Hg) After Adjusting for Systolic Blood Pressure, Age, and BMI During RARP at Six Time Points
BMI, body mass index; IOP, intraocular pressure.
Discussion
Although there are advantages of minimally invasive laparoscopic operation such as RARP, it is associated with certain adverse physiological effects such as changes in IOP, which sometimes results in complications such as postoperative ION, benign subcutaneous emphysema, and glaucoma due to the application of different maneuvers during the procedure. 3,12,13 Patients undergoing RARP are placed in Trendelenburg position with heads tilted downward as much as 30ο−45ο along with abdominal insufflation to create room for robotic arms to work. 14
Previous studies have explored the behavior of different systems in response to these maneuvers during RARP. 15 One of the adverse physiological changes during RARP is the change in IOP and various studies have attempted to identify various factors associated with this change such as impact of Trendelenburg position, degree of head inclination at Trendelenburg position, length of operation, BMI, age, and blood pressure; however, the interplay between abdominal insufflation pressure and IOP remains minimally explored. 15
Our study aimed to delve into the aspects of changes in IOP as a function of abdominal insufflation pressure through measuring IOP changes at a series of six time points such as: in preoperative room (T1), in the operating room after anesthesia induction in supine position without insufflation (T2), in Trendelenburg position at 30ο head tilt (T position) without insufflation (T3), at the Trendelenburg position with abdominal insufflation at 10 mm Hg (T4), 15 mm Hg (T5), and 20 mm Hg (T6). Our findings suggest that IOP is strongly associated with abdominal insufflation pressure. As shown in the Figure 1, IOP drops from a mean of 13.6 mm Hg to 10.9 mm Hg after anesthesia induction while the patient is in supine position. Subsequently, placing the patient into a Trendelenburg position causes an increase in the IOP from a mean of 13.6 mm Hg to 20.6 mm Hg, and thereafter increase in insufflation increases the mean IOP to 24.2, 26, and 26.6 mm Hg at T4, T5, and T6, respectively.
On an analysis of percent change in mean IOP at different time points (T2−T6) compared with T1 as shown in Supplementary Figure S1, it is observed that after anesthesia induction there is an average 17.85% drop in mean IOP. However, Trendelenburg position at T3 causes a 56.33% rise in mean IOP compared with baseline mean IOP at T1. From time points T4−T6, there is gradual increase in percentage change to 82.47%, 95.56%, and to 102.56%, showing the nearly equal contribution of position and insufflation. Therefore, our results show that both positioning as well as insufflation are the key parameters driving the change in IOP during RARP.
This finding is consistent with the previous studies that have illustrated an increase in IOPs with Trendelenburg position at different degrees of head inclination such as 30ο and 45ο. 7 In this study, we delved into a unique aspect that plays a pivotal role in increasing the IOP during RARP, which is the recommended increase in abdominal insufflation pressure to lift the anterior abdominal wall upward to create room for robotic arms to work. 4
Several other factors that presumably impact IOP were considered in our study, such as systolic blood pressure, age, and BMI. 12,16,17 We found a substantial association of systolic blood pressure with IOP consistent with previous studies. 18 In this study, the mean systolic blood pressure ranged from 111.85 (±17) mm Hg to 132.1 (±17.3) mm Hg across six time points. Blood pressure is quite often maintained during RARP for hemodynamic stability; however, our findings indicate that 1 mm Hg increase in systolic blood pressure increases the IOP significantly by 0.058 mm Hg. While low blood pressure may also be a concern for potential ischemia, the finding of higher IOP with higher blood pressure suggests that patients undergoing RARP with a history of hypertension should be cautiously monitored for postophthalmic changes. 19
Surprisingly, in our study cohort with a mean age of 61.2 years, we could not identify a positive association between age and IOP, inconsistent with findings from other epidemiological studies. 20 Age, despite its causal relation with high blood pressure, might not significantly impact IOP; however, caution should still be taken while performing RARP, as most patients undergoing RARP are older than 60 years, and the prevalence of glaucoma increases with age. 21
Although our results were derived from apparently healthy patients on ophthalmic assessment, we infer that a careful increase in the abdominal insufflation pressure can prevent the incidence of adverse physiological effects associated with increased IOP. This assumption is based on the understanding that after accounting for between−patient and within−patient variability, our mixed-effects method showed that a change in 1 mm Hg of abdominal insufflation pressure is associated with a 0.35 mm Hg increase in IOP (95% CI = 0.29–0.40, p < 0.001), holding all other variables constant (Table 2).
An increase in IOP poses a clinical concern as it increases the risk of vision loss due to ION. 22 The increasing use of RARP requires careful consideration of potential complications, one of which is ION—a rare but serious condition linked to elevated IOP. During RARP, the steep Trendelenburg position and abdominal insufflation can raise IOP, potentially decreasing blood flow to the optic nerve, which increases the risk of ION and vision loss. 23 Although a direct causal relationship between elevated IOP and postoperative visual dysfunction has not been clarified to date, it has been reported that transient focal visual field defects occur in 28% of nonglaucoma patients after RARP operation. 7 Although, not captured in this study, literature does show the return of this increased IOP to baseline. In a study by Kondo et al., the baseline intraocular pressure was restored at 30 minutes after the supine position was reassumed, however, the authors did not describe any impact of insufflation on IOP and return to baseline of IOP. 24 Although the measure of IOP changes associated with insufflation provide insights into the clinical issue of retinal safety, future studies to examine actual retinal blood flow will be of great value to understand the true clinical implications of these pressure changes on retinal health.
Based on our study and previous evidence, preoperative ocular assessments are crucial for elderly, obese, and hypertensive patients due to high risk of glaucoma. 25 Postoperative ION after laparoscopic procedures, particularly those requiring steep Trendelenburg positioning and under high abdominal insufflation pressures, underscores the need for surgeons to understand and master these techniques to reduce the risk of ION occurrence. An important tangential is that the pathological changes that occur when abdominal insufflation pressure exceeds 12 mm Hg, a widely used pressure in laparoscopic surgical procedures, gradually affect various organs. 26 Literature has shown some studies that observed the impact of increasing abdominal insufflation pressure on the thorax, cranium, and eyes. 27 Furthermore, one report showed that transient visual field loss may occur in as much as 28% of subjects undergoing RARP in steep Trendelenburg position. 7
ION is associated with prolonged durations of ischemia to retinal neurons and the optic nerve due to a combination of relatively low blood pressure during operation and elevated IOP because of positioning and intraperitoneal gas. 28,29 Hayreh et al. have shown that retinal damage is irreversible after 97 minutes of central retinal artery occlusion (CRAO). 30 While RARP does not produce as severe an ischemic event as CRAO, it produces prolonged periods of significant ocular under-perfusion that may cause lasting harm. 31 Oz et al. have shown (in animal models) that transient ischemia over shorter 5–10 minute periods also induce retinal degeneration. 32 The risk of developing ION is not uniform across patients, as some may tolerate elevation of IOP better than others, as has been observed in patients with hypotension. 14,33
The strengths of our study include the relatively new concept of the study, finding an association of IOP with insufflation pressure as well as the prospective, longitudinal assessment of important factors; abdominal insufflation pressure, age, BMI, and systolic blood pressure with IOP measurements, which were discussed minimally in a few prior studies. We also used the patients without a prior history of glaucoma or any other eye diseases to control for any potential confounders. Our study also has several limitations. First, this is a single-center and single-arm study, limiting the generalizability of our findings. Second, the study did not account for the effect of choice of anesthetic drugs and respiratory pressures on IOP during the RARP. Similarly, our study was also limited in measuring the rate of return of the IOP to baseline, excluding the glaucoma patients from the study, and the small sample size might have limited our results regarding the impact of age on IOP.
In conclusion, this is the first prospective study to underscore the importance of optimal abdominal insufflation pressure during RARP at a 30ο Trendelenburg position to mitigate potential optic nerve stress. Although no ocular complication was observed, these findings suggest that IOP during RARP in the 30ο Trendelenburg position increases linearly and significantly with an increase in abdominal insufflation pressure and may pose patients with insufflation-related ophthalmic complications.
Footnotes
Authors’ Contribution
A.K.: Writing—original draft (lead), formal analysis (lead), writing—reviewing and editing (equal role), and data curation (equal role). S.W.: Methodology (equal role), writing—reviewing and editing (supporting role), data curation (lead), and conceptualization (supporting role). O.S.: Conceptualization (equal role), methodology (equal role), and writing—review and editing (supporting role). A.R.: Conceptualization (supporting role) and writing—reviewing and editing (supporting role). M.M.S.: Conceptualization (lead), writing—reviewing and editing (lead), and supervision (lead).
Author Disclosure Statement
The authors declare no conflicts of interest related to this research study, in the authorship, or publication of this article. All authors confirm that this work has been conducted in accordance with the ethical standards and that there are no financial, professional, or personal relationships that could be perceived as influencing the presented work.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Figure S1