
Abstract
Introduction:
Anatomical endoscopic enucleation of the prostate (AEEP) is considered a size-independent method for treating lower urinary tract symptoms (LUTS) secondary to benign prostatic obstruction (BPO) according to current international BPO guidelines. AEEP offers less perioperative morbidity compared with traditional transurethral resection of the prostate (TURP) or open prostatectomy while providing comparable long-term durability to open prostatectomy. The thulium fiber laser (TFL) is one prominent energy source for AEEP, which has been widely adopted around the world. We present a step-by-step surgical approach to thulium laser enucleation of the prostate (ThuLEP) using the TFL, describing a modified en-bloc technique for AEEP.
Materials and Methods:
In this video, a modified en-bloc technique is presented, performed by one surgeon (C.N.) at our institution.
Results:
In this example, the outcomes of the en-bloc technique are similar to those of traditional two- or three-lobe techniques.
Conclusions:
ThuLEP as a treatment for LUTS secondary to BPO results in excellent patient outcomes and can be offered as a treatment of choice for prostates of any size.
The ThuLEP Procedure
Thulium laser enucleation of the prostate (ThuLEP) combined with mechanical morcellation was described in 2010 as a safe and efficient procedure for the treatment of symptomatic benign prostatic obstruction (BPO) with good functional results and a low reoperation rate at intermediate-term follow-up. 1 Thereafter, this technique has been established as another minimally invasive procedure for the treatment of symptomatic BPO. It has been found that ThuLEP is a size-independent, safe, and effective procedure with low perioperative morbidity and good long-term results 2 –6 (Table 1).
Major published series of outcomes following ThuLEP
Data as mean.
At last follow-up.
BNC = bladder neck contracture; PVR = postvoid residual urine; IPSS = international prostate symptom score; Qmax = maximum urinary flow rate; QoL = quality of life; ThuLEP = thulium laser enucleation of the prostate.
Indications
The indications for any bladder outlet procedure are determined clinically according to the current guidelines of the American Urological Association, 7 –9 the European Association of Urology, 10 or the German Association of Urology. 10,11
Preoperative Preparation
The diagnosis of BPO is based on the patient’s history and the extent of complaints, which can be objectively assessed by maximum urinary flow rate, international prostate symptom score (IPSS), and postvoid residual urine (PVR). Absolute indications might include failed medical therapy for BPO, recurrent urinary tract infections (UTI), bladder stones, recurrent bleeding from bladder neck varicosis, and/or recurrent episodes of urinary retention. 11 If necessary (e.g., in cases of suspected urethral stricture or neurogenic bladder disease), cystoscopy or urodynamic testing might be performed. Preoperative assessment includes a physical examination with a digital rectal examination, prostate volume (PV) measurement by transrectal ultrasound (TRUS), uroflowmetry, measurement of PVR, IPSS, quality of life assessment, PSA assay, urine analysis, and urine culture.
PV measurement by TRUS might be helpful to predict the duration of surgery and operating room utilization, as well as for patient selection in resident/fellowship training. In addition, in cases of supersized prostates (>200 mL), a computed tomography scan or magnet resonance imaging might be more accurate for assessing PV than TRUS. A urine culture is mandatory to exclude a UTI. In patients with sterile urine, we recommend routine perioperative antibiotic prophylaxis with a second-generation cephalosporin until the catheter is removed; for those with a positive culture, antibiotics should be administered according to the antibiogram.
Patient Positioning
Patients are positioned in the dorsal lithotomy position with lower extremity pressure points padded to avoid potential neuropraxia (Fig. 1). 12

Patient positioning for maximal maneuverability of the resectoscope. Red arrows show the possible directions of the resectoscope during surgery.
Operating Room Setup
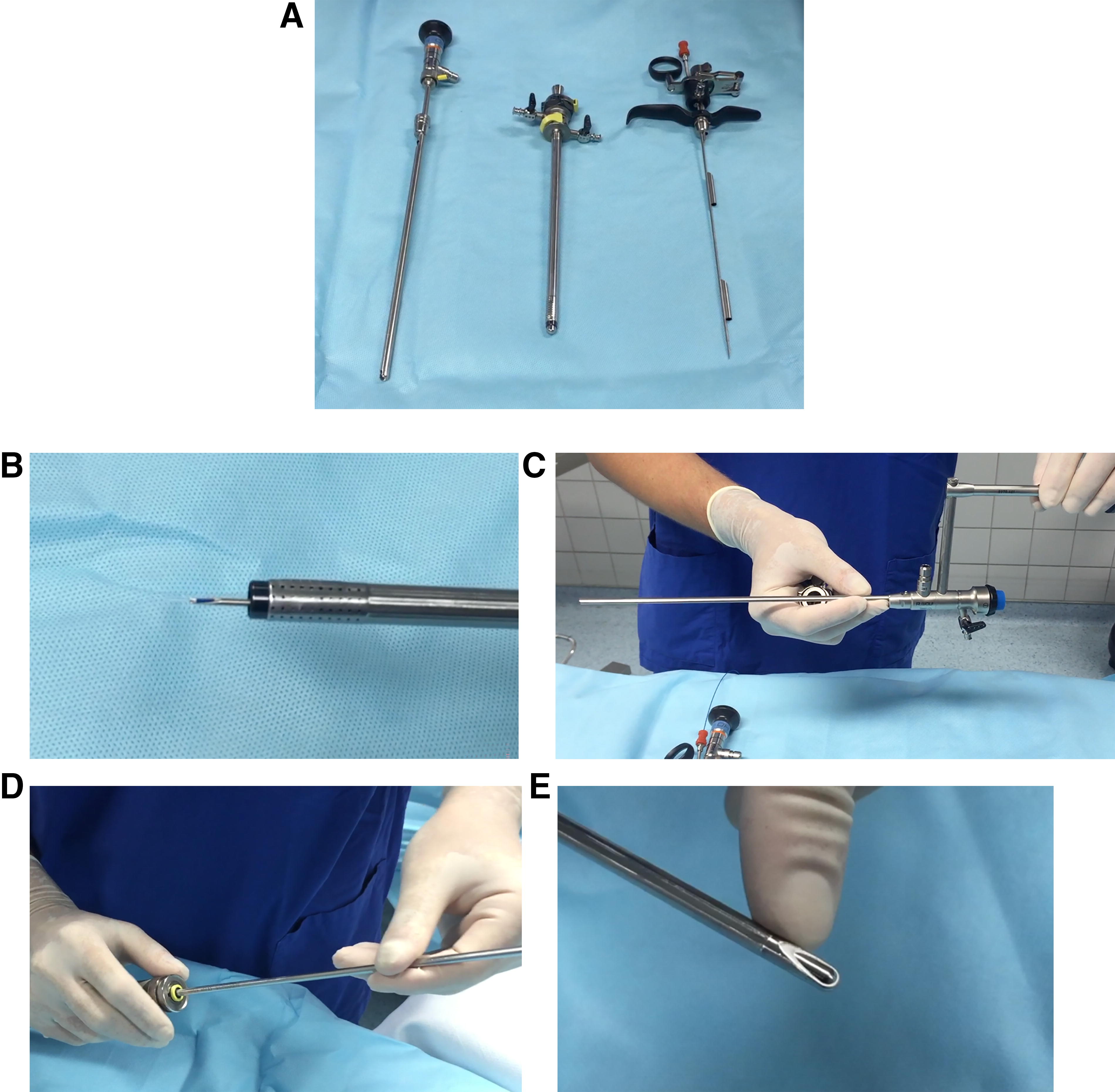
A 26 F continuous-flow laser resectoscope (Fig. 2A/B), in combination with a mechanical tissue morcellator (Fig. 2C–E) (Wolf Piranha®, Richard Wolf, Knittlingen, Germany), is used. The ThuLEP procedure is performed using a pulsed 60-W thulium fiber laser (Pulvis 60+, Richard Wolf, Knittlingen, Germany) at 60 W (2J, 30 Hz). A 550 µm bare-ended, reusable laser fiber is used, as this laser fiber diameter offers the best compromise regarding stability, handling, energy transmission, and irrigation (Fig. 2A, B). The laser settings remain unchanged during the enucleation procedure and are as follows: 2J/30 Hz for enucleation and 0.5J/60 Hz for coagulation. The enucleation procedure can be performed with or without active suction. All interventions are carried out using normal saline (10-L bags, 1 m above the table) as the irrigation fluid.
Surgical Steps
The urethra is calibrated to 26 F, and if necessary, an Otis urethrotome can be used to incise the distal penile urethra and meatus.
The laser resectoscope is introduced into the bladder with the obturator under direct vision using a 26 F continuous-flow resectoscope.
The initial cystoscopy is performed to define the prostate anatomy, the distal extent of the dissection, and the position of the ureteral orifices, and to decide whether to perform an en-bloc, bilobar, or trilobar technique.
In this procedure, we perform an en-bloc technique, starting with an incision around the verumontanum to define the level of enucleation (i.e., the prostatic pseudocapsule), followed by undermining the left, right, and middle lobes.
After defining the apex, an apical release of the apicomucosal strip is performed (left and right lobes). Once the adenoma is detached from the apex, an en-bloc antegrade dissection of the prostate is carried out (Fig. 3).
After retrograde opening of the bladder neck at 12 o’clock, the left adenoma, and then the right adenoma, is enucleated and mobilized to the 6 o’clock bottom position of the prostate fossa (Fig. 4).
Next, an en-bloc enucleation of the middle lobe, together with the lateral lobes, toward the bladder neck is performed. In large prostates, an en-bloc technique may be technically challenging, particularly if the bladder neck is too narrow for the size of the prostate gland. In such cases, a modification might involve switching from an en-bloc to a two-lobe technique. This would involve making an incision at 5 or 7 o’clock, enucleating one lobe, and then enucleating the middle lobe along with the remaining side lobe.
Once the en-bloc prostate adenoma is completely detached, it is placed into the bladder (Fig. 5).
Meticulous coagulation of the prostate fossa and its bleeders is then performed (Fig. 6).
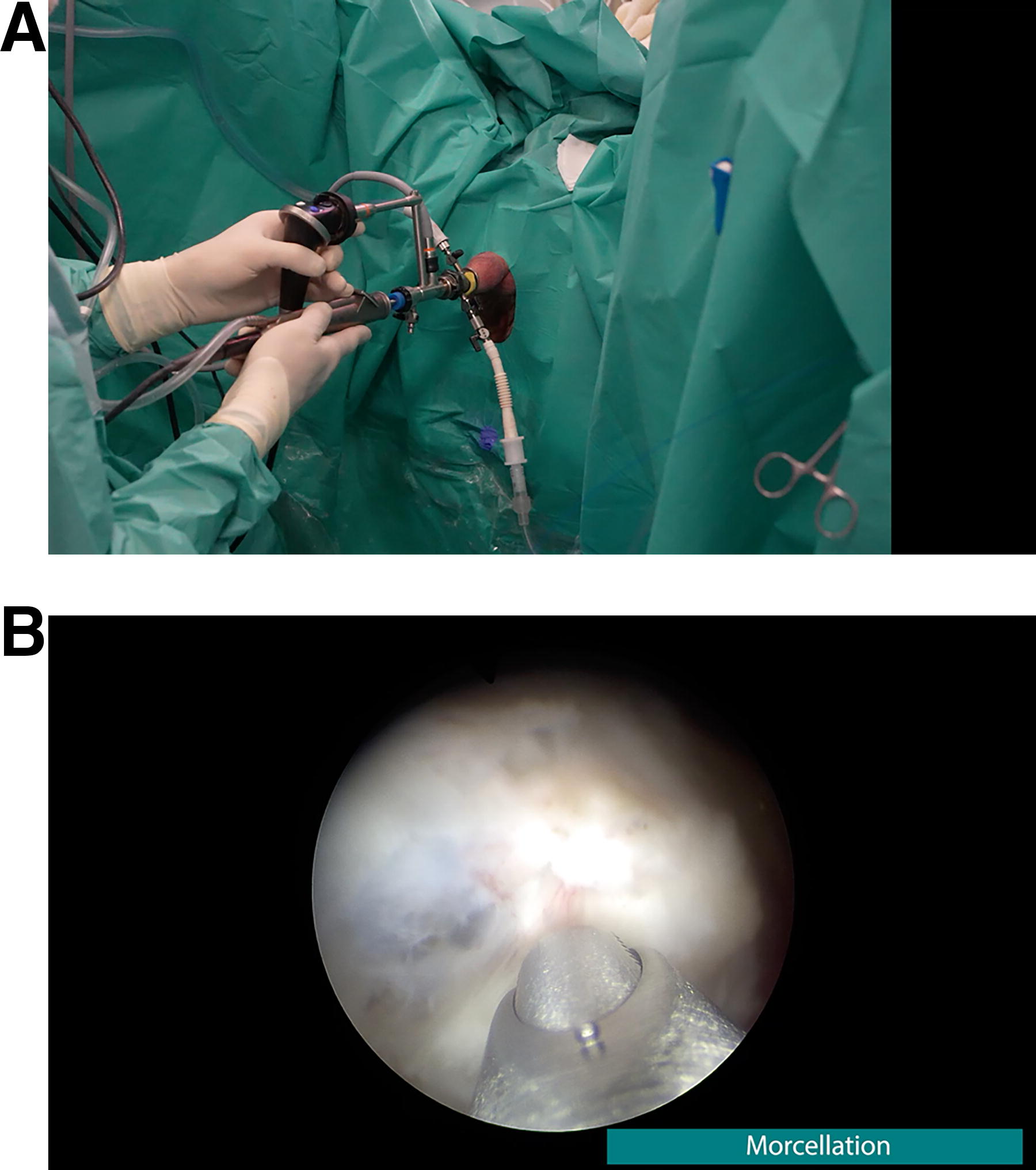
Morcellation is performed using the Wolf Piranha® Morcellator (Fig. 7a). The standard setting is 1500 oscillations per minute. In the case of dense tissue (e.g., “beach ball tissue”), the setting should be reduced to 850–1000 oscillations per minute. The bladder should be kept fully distended throughout the morcellation procedure to avoid suction of the bladder wall (Fig. 7b)
A final inspection of the prostate fossa should be conducted to ensure hemostasis and to verify that no prostate tissue has been overlooked, particularly in large glands.
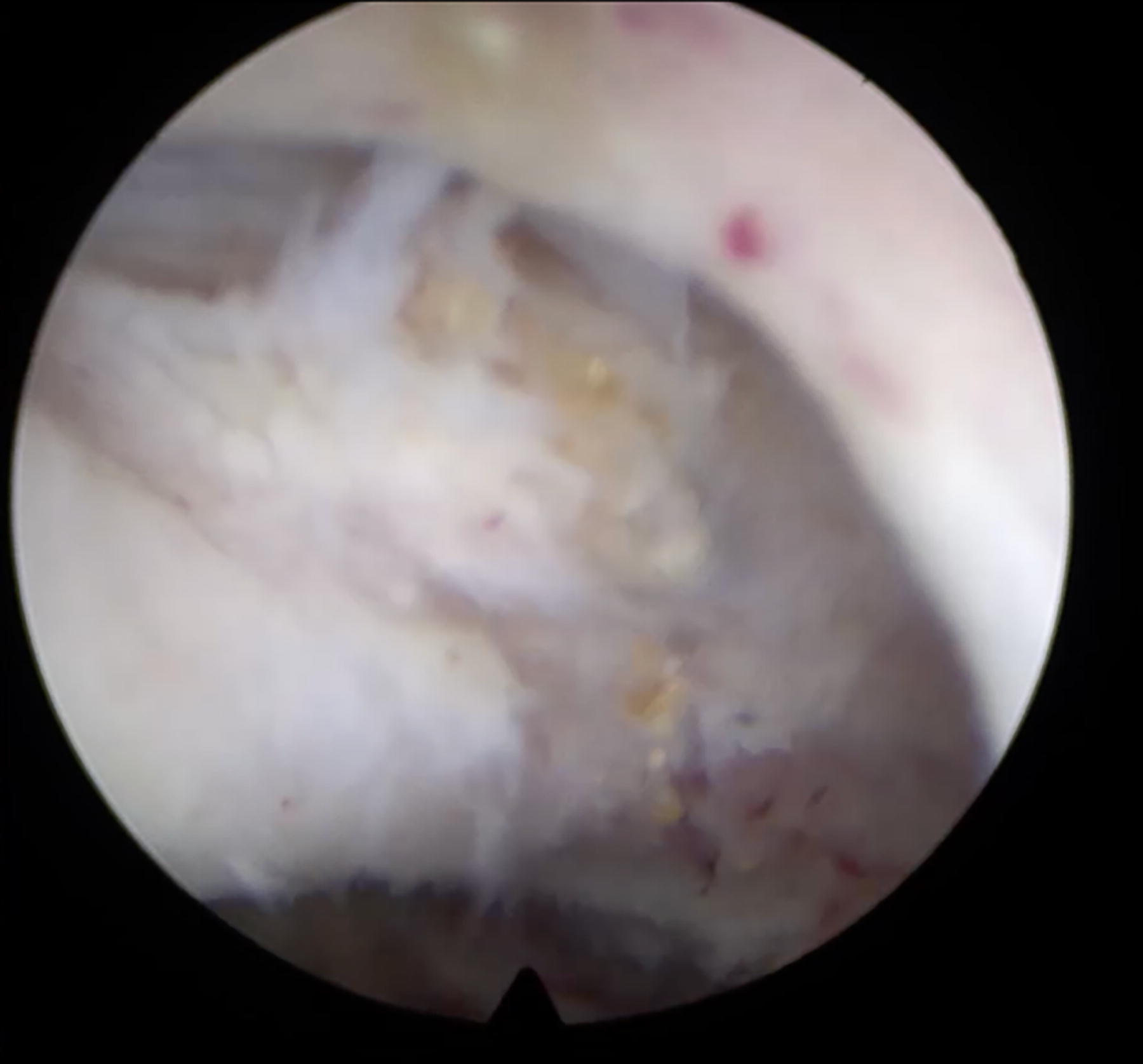
Release of the left lobe from the apicomucosal strip.
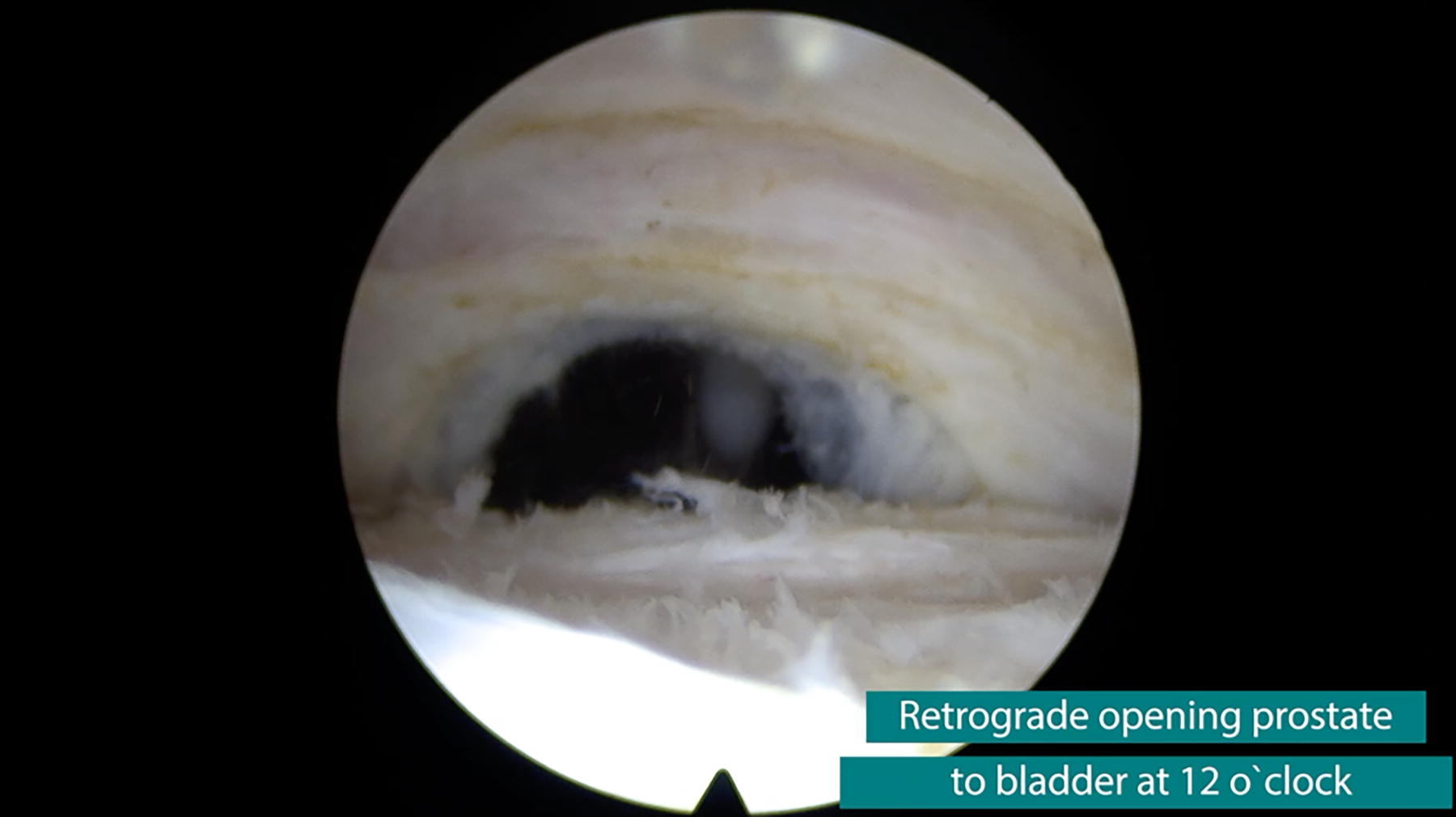
Retrograde opening of the bladder neck (via from apex to bladder neck).

Look from the prostate fossa to en-bloc released prostate in the bladder. The adenoma has rotated in the bladder at 180°. At the top, the midline between the lobes is visible, and at the bottom the commissure.
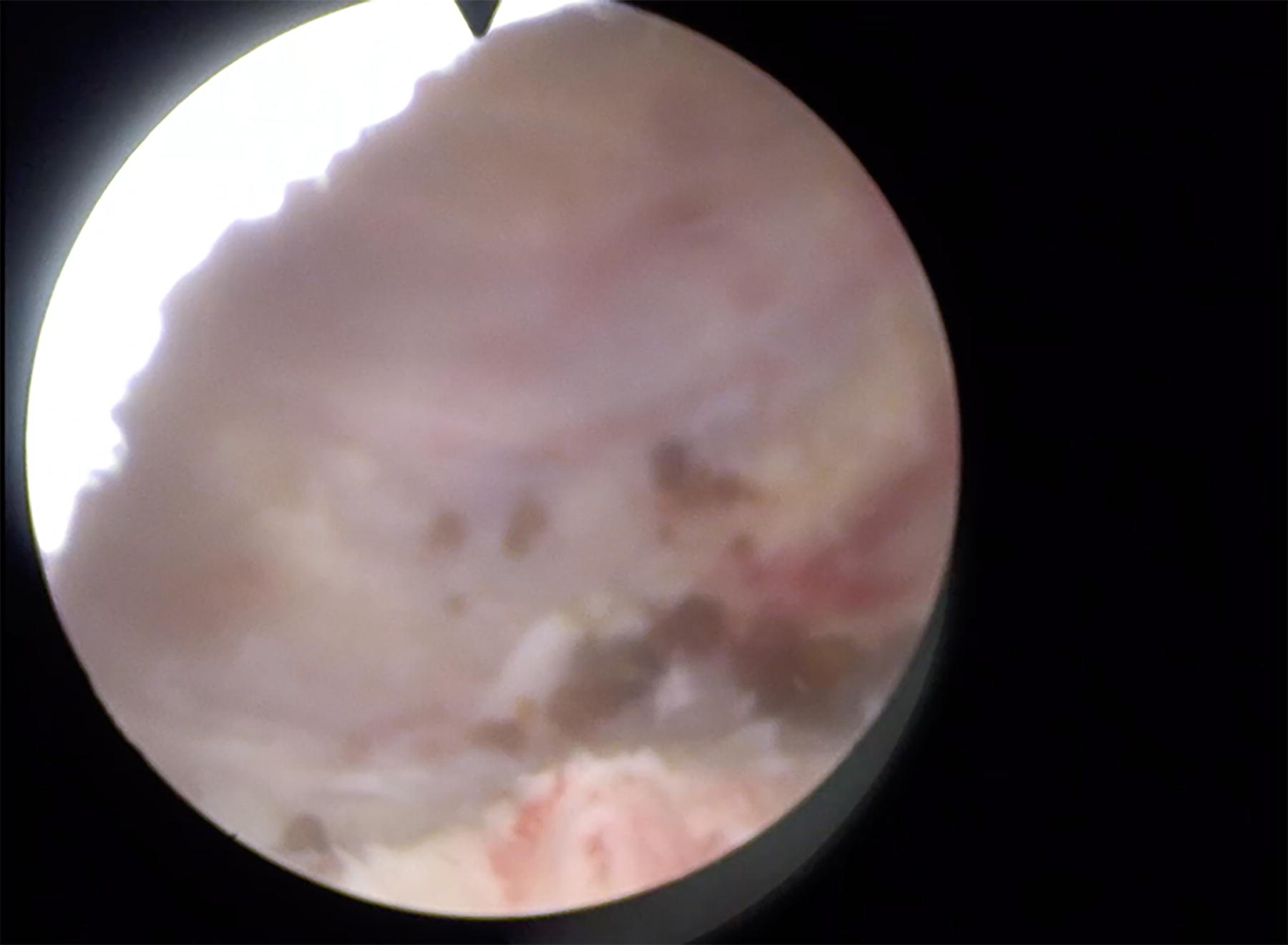
Look from the apex to the prostate fossa after enucleation.
Postoperative Care
At the end of surgery, a 22 F three-way Foley catheter is inserted and inflated in the bladder for continuous bladder irrigation (CBI). CBI is routinely discontinued the following day. If the urine is clear, the catheter is removed on the first postoperative day. If patients can void adequately, they are discharged on the first postoperative day. Antiplatelet treatment is routinely continued during surgery. However, direct oral anticoagulants as well as anticoagulant therapy are paused 2–7 days before surgery (depending on the medication) and then resumed after a week. Patients are instructed to avoid vigorous activity and heavy lifting (>5 kg) for one to two weeks.
Troubleshooting
Essentials for beginners
The ideal PV to learn the ThuLEP or AEEP procedure ranges between 50 and 80 mL, which is a PV most transurethral resection of the prostate (TURP) surgeons are familiar with and can easily switch to TURP if they encounter difficulties. In smaller prostates (<40 mL), the prostatic pseudocapsule is difficult to identify for beginners, whereas orientation in larger prostates (>100 mL) with large prostate fossae might be confusing for beginners (e.g., opening multiple layers). In addition, in larger prostates, because of the prolonged OR time (for beginners), the risk of fluid influx (NaCl 0.9%) increases, which can be counteracted with 20 mg of furosemide i.v. given hourly. In supersized prostates (>200 mL), there is an increased risk of requiring a staged procedure since the morcellation procedure sometimes significantly increases OR time (>3 hours) and, therefore, the risk of fluid absorption. A morcellation performed 1 or 2 days after ThuLEP is safer and significantly faster because of softened prostate tissue. However, in difficult cases, an open cystotomy (Sectio alta) is also a possible solution.
Capsular Perforation
Capsular perforation can occur at any stage of the learning curve and in procedures performed by expert surgeons. It is important to counteract any fluid absorption immediately by administering 20 mg of furosemide i.v. every hour during surgery to prevent fluid overload (isotonic hypervolemia). However, no correlation between long-term complications and capsular perforation has been published so far.
Significant Bleeding
Meticulous control of all bleeders in the prostate fossa is crucial before starting the morcellation procedure. Bleeding control follows the same principles as in TURP: control of arterial bleeders at 5 and 7 o’clock and at the apex. In larger glands (>100 mL), it is sometimes necessary to resect the bladder neck with bipolar/monopolar current because of extensive bleeders from bladder neck varicosis, which is difficult to control with laser energy. When using laser energy for bleeding control, the laser should be defocused from the bleeding vessels. In some cases, catheter traction at the bladder neck or in the prostate fossa might also be reasonable.
Bladder Perforation During Morcellation
The major cause of bladder injury during morcellation is impaired vision. Bladder injury can be avoided by morcellating in a fully distended bladder. It is crucial to address bleeders in the prostate fossa before starting the morcellation procedure. The tip of the morcellator should be kept in the center of the filled bladder. Upside-down morcellation should be avoided. The surgeon’s attention should also be on the irrigation fluid. Owing to the negative pressure of the morcellator, the bladder can empty very quickly if the irrigation fluid runs out.
Morcellator Malfunction
If the morcellator malfunctions, every part should be checked carefully. Sometimes the morcellator instruments need to be changed. If the morcellator still does not work, a secondary morcellation can be safely performed the next day.
Footnotes
Author Disclosure Statement
A.J.G.: None. C.N. and B.B.: Richard Wolf.
Funding Information
No funding was received for this article.