
Abstract
Abstract
Introduction
S
Despite the expansive nature of the published literature, there is no clear methodological consensus with respect to assessing differential air pollution exposures by socio-demographic characteristics. Several challenges in comparing research findings on systematic racial or socioeconomic disparities in air pollution exposure include the use of different geographical units of analyses (e.g., regional, census tract, and ZIP code level), different analytic methodologies, difficulties in disentangling race and SES, and different measures of exposure.6,7,8 To date, much of the extant literature on environmental justice has been based on group level variables in the general population. 7 Less is known on how area-level SES predictors relate to ambient air pollution exposures in an already vulnerable subgroup. This is particularly important in studies that consider the effects of air pollution on respiratory health outcomes since ambient air pollution concentrations and pre-existing health conditions may be modified by area-level SES characteristics.
This article aimed to characterize and quantify the burden of ambient air pollution exposures experienced by a vulnerable subgroup of subjects with chronic obstructive pulmonary disease (COPD). We used both U.S. Environmental Protection Agency (EPA) Air Quality Systems (AQS) pollution data and results from the National Emphysema Treatment Trial (NETT) to detect differences in ambient air pollution exposure with area-level SES factors. Identifying whether there exists evidence of differential exposure in air pollution concentrations based area-level SES factors would contribute to a greater understanding of the potential health risk faced in an already susceptible population.
Methods
Study population
The NETT was a multicenter, randomized controlled trial with the objective of assessing whether lung volume reduction surgery (LVRS) in conjunction with medical therapy was a better long-term treatment for subjects with severe emphysema when compared to medical therapy alone.9,10 The major outcomes of interest in the study were post-treatment mortality and maximal exercise capacity. Additional outcomes of interest included lung function, as determined by spirometry, distance walked in six minutes and quality of life. During the period 1998–2002, a total of 1,218 participants were enrolled in the study, of which 608 were randomized to LVRS and medical management; 610 were randomized to traditional medical therapy alone, such as steroids and bronchodilators. 11
Radiologists characterized emphysema distribution and magnitude in the lungs with chest computed tomography (CT) scans and a visual scoring scale. The aim of the LVRS was to remove 25% to 35% of the lung, with a particular focus on the most affected areas. 9 Medical histories of all participants were collected at 6, 12, 24, 36, 48, and 60 months after baseline. Participants were followed for an average of 29.2 months.9,11
Air pollution data
We obtained pollution data from the U.S. EPA AQS database. 12 We restricted these data to average daily ozone levels (1997–2003), and average daily PM2.5 values (1999–2003). Because exact addresses were not available for NETT participants, we used ZIP codes to define participant place of residence. Participants were assigned residence at the centroid of their ZIP code, as determined by the 2000 census. Values from monitors within specific ZIP codes were used to interpolate pollutant concentrations at the centroid of the ZIP code, and were then merged with the NETT data. Only resident ZIP codes corresponding with kriged ZIP code specific pollution levels, were considered for the analysis, per Liao et al. 13 Air pollution data were estimated using log-normal kriging, a technique that allows for the estimation of pollutant values in areas that may not be monitored, in which data from nearby monitoring stations are weighted based on distance and number of monitored locations. Participants with the same ZIP code were assumed to share the same level of exposure. In these analyses, daily pollutant concentrations were averaged as a cumulative measure over the duration of the study.
Geographical units of analysis
Aggregate SES data were obtained from the 2000 U.S. Census Summary File 3 (SF3). 14 Variables were obtained at the ZIP code tabulation area (ZCTA) level. Although ZCTA codes are similar to ZIP codes in that they both share the same designation, ZIP codes were developed as a means to expedite postal delivery, whereas ZCTA codes were developed based on characteristics of Census blocks. The ZCTA code is determined by the U.S. Census by calculating the total number of addresses contained within the Census block boundaries. The Census Bureau then assigns the most frequently occurring ZIP code to the Census block tabulation area. In the case where no ZIP code data are available, values from a contiguous block are employed to assign the ZCTA code. Only one ZIP code is assigned to each Census block tabulation area regardless of its size.15,16
Socio-demographic variables
Measures of area-level socioeconomic deprivation (SED) have been common and effective ways to examine the effect of socioeconomic disparities on health. Indices such as the Carstairs score and the Townsend SED index have been utilized to capture and summarize multiple aspects of SES.17,18 In our study, we measured area-level SES with the use of the Townsend SED Index, which more readily allowed for the inclusion of Census data. This index was constructed with the following variables: percent of unemployed individuals aged 16 and older, percent renters, percent overcrowding (defined as more than one occupant per room), and percent of individuals that do not own a car. Values of all variables were obtained at the ZCTA level. Percent unemployed and percent overcrowding were log-transformed before being standardized. Percent renters and percent without a car were also standardized before being included in the overall score. Standardization was performed by subtracting the mean value from the variable of interest and dividing it by its standard deviation. These individual z-scores were then summed to yield the overall SED index value. The SED index value was then stratified and ranked by deciles. Additional ZCTA-level variables considered in the analyses included total population, median income, mean earnings, percent urban residents, and percent of individuals living below 200% of the federal poverty level (FPL).
Statistical analysis
Air pollution, Census, and NETT data were merged based on participant ZIP code. Bivariate analyses were performed to assess how ZIP code level variables correlated with cumulative ozone and PM2.5. ZIP code level variables that were significantly correlated (r>0.3, p-value<0.05) with pollutant concentrations were included in the linear models. Area-level SES variables that were highly correlated with the SED index were not included in the hierarchical models in order to minimize problems associated with multicollinearity. To model cumulative pollutant exposure, models were initially constructed with ZCTA-level SES factors alone, and then with interactions of ZCTA-level SES characteristics. We compared nested linear regression models using a likelihood ratio test or the likelihood-based Akaike's information criterion (AIC). 19 The final linear models included the following covariates: region of residence, SED index deciles, total number of people residing in the ZIP code, median income, and percent of people living below the poverty level in the ZIP code.
The PROC REG procedure was used for the linear regression models. All analyses were performed with SAS 9.2 (SAS Institute Inc, Cary, NC).
Ethics
Approval for this study was received from the Institutional Review Board at The Ohio State University. Because this was a secondary data analysis, no patient contact or consent was required.
Results
Of the original 1,218 participants, there were 1,204 subjects for whom there was complete ozone and PM2.5 data and whose ZIP codes were also designated in the U.S. Census SF3 database. There were a total of 1,128 unique ZIP codes.
Results of our analyses show evidence of an association between SES measures and air pollution. Specifically, individuals residing in ZIP codes that were in the lowest percentile of the SED index had increased PM2.5 exposures compared to those residing in the highest percentiles (Figure 1). Although there was more variability seen with cumulative ozone levels, it is still indicative of the trend line of increased exposure among those with a higher SED index (Figure 2). In the bivariate analyses, cumulative ozone was significantly correlated with median income (r=−0.22, p<0.01) and percent below 200% FPL (r=0.11, p<0.01). It was not however correlated with SED index (r=0.04, p=0.14) but it was significantly correlated with the ranked SED index (r=−0.07, p<0.05). Cumulative PM2.5 was significantly correlated with SED index (r=0.12, p<0.01), ranked SED index (r=−0.11, p<0.01), median income (r=0.11, p<0.01), and percent below 200% FPL (r=−0.1, p<0.01) (Table 1).
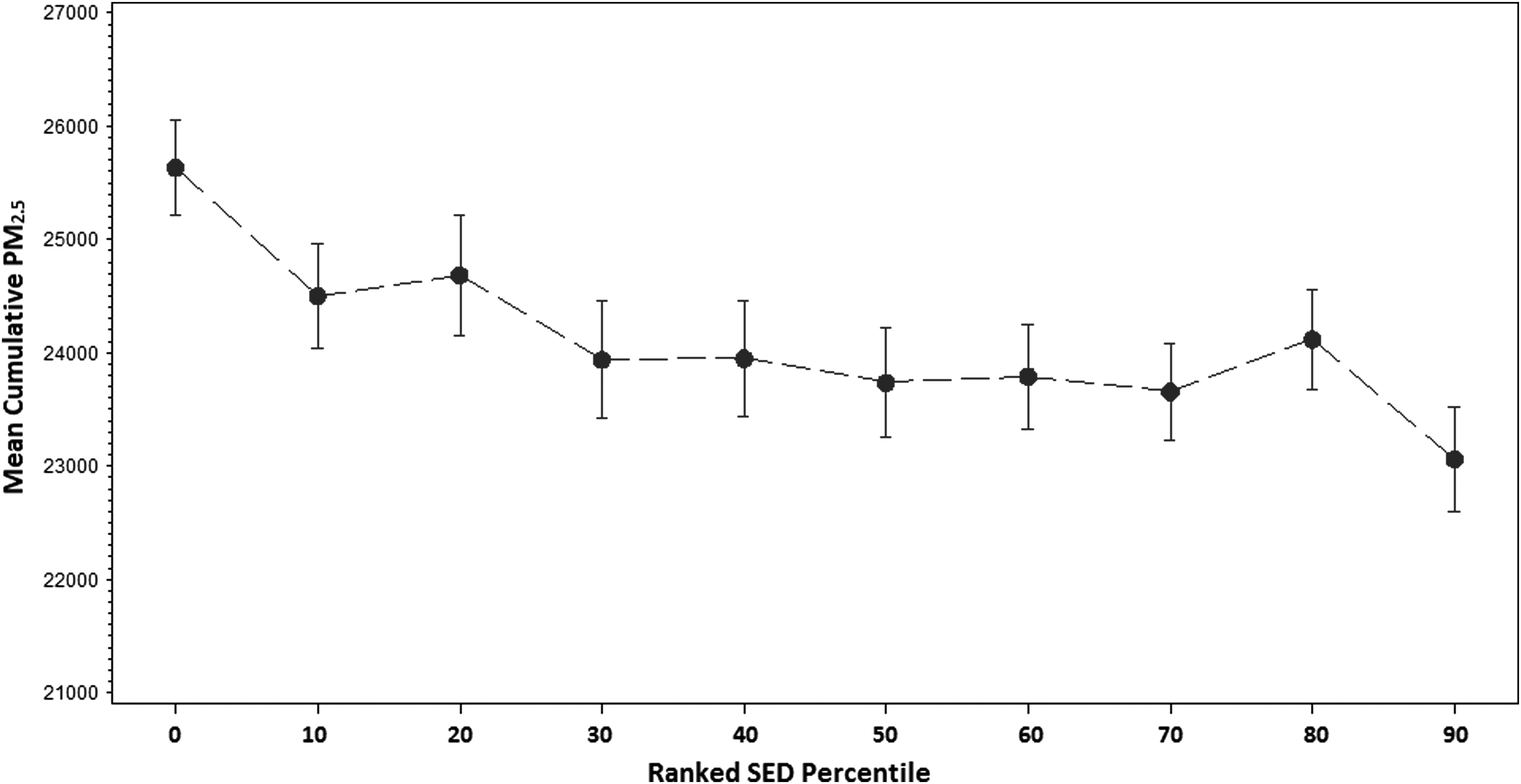
Mean cumulative PM2.5 by ranked SED index percentile. Mean cumulative PM2.5 were calculated and plotted against each ranked SED percentile. Error bars represent±1 standard error of the mean. PM2.5: particulate matter; SED: socioeconomic deprivation.
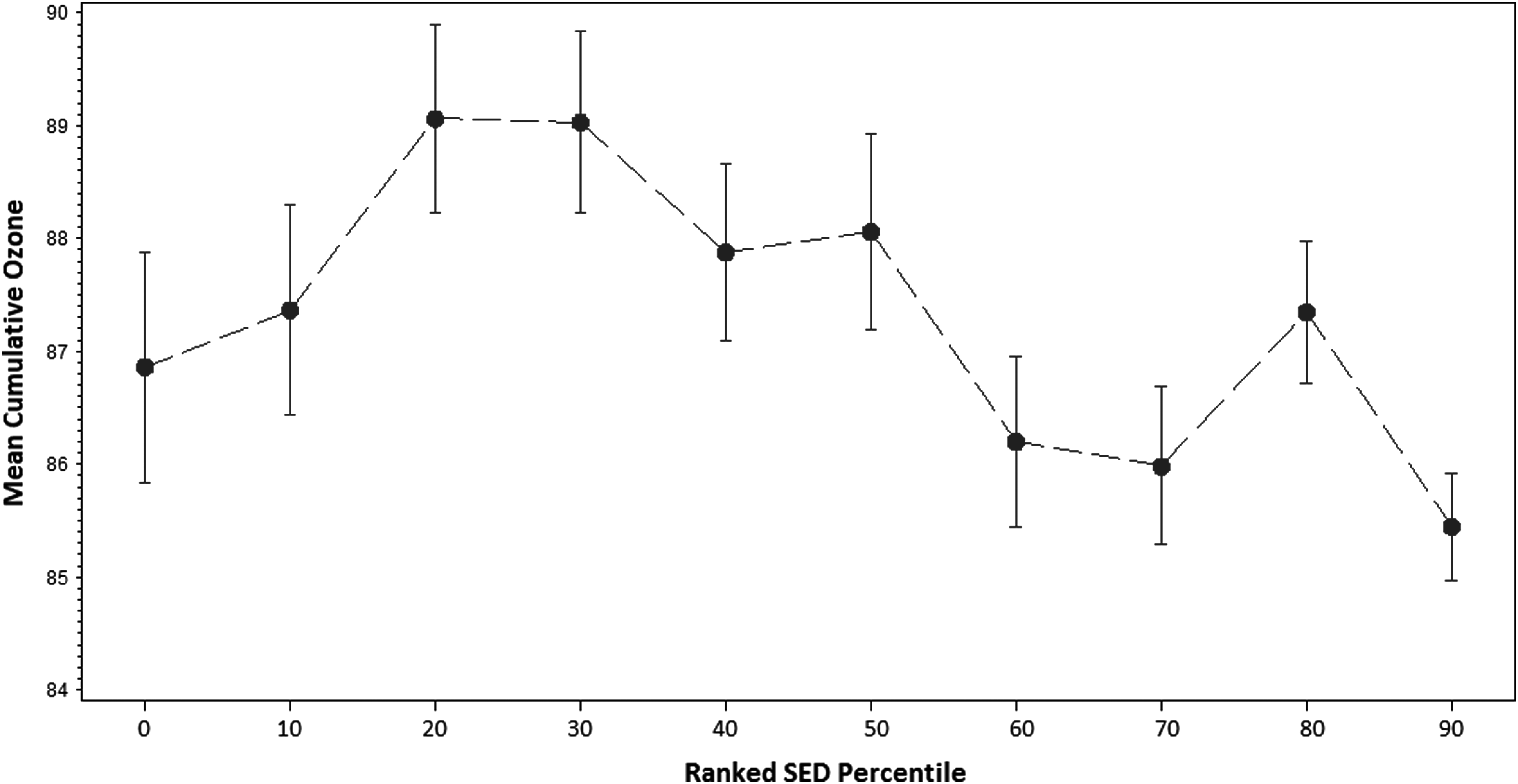
Mean cumulative ozone by SED index percentile. Mean cumulative ozone concentrations were calculated and plotted against each ranked SED percentile. Error bars represent±1 standard error of the mean. SED: socioeconomic deprivation.
SED: socioeconomic deprivation index; FPL: federal poverty level; PM2.5: particulate matter.
p-value<0.05.
In the cumulative pollutant regression models adjusted for region of residence, SED index deciles, total number of people residing in the ZIP code, median income, and percent of people living below the poverty level in the ZIP code, ranked SED index was significantly associated with cumulative PM2.5 (Table 2). Increasing SED index decile was associated with a decrease of 155.09 μg/m3 (standard error [SE]=58.11, p<0.01) in cumulative PM2.5. Individual level factors such as sex and region of residence were all significantly associated with increased cumulative PM2.5 exposure. Interestingly, median income was significantly associated with increased cumulative PM2.5 exposure, although the effect was relatively small (β=0.03, SE=0.01, p<0.01). Individual level age and education were not considered as covariates in the cumulative PM2.5 model as the model focused solely on ZIP-code-level variables.
PM2.5: particulate matter; SES: socioeconomic status; SE: standard error; SED: socioeconomic deprivation index.
For the cumulative ozone model, there was a significant negative effect of the ranked SED index (β=−0.32, p=0.02); however this occurred in the presence of a significant interaction between the ranked SED index and total population (Table 3). The only significant covariates in the model were median income, region of residence, and percent living below 200% FPL. Large effect estimates were seen for region of residence in both pollutant models.
SES: socioeconomic status; SE: standard error; SED: socioeconomic deprivation index.
Discussion
Our findings suggest there is a significant differential exposure to ambient ozone and PM2.5 exposures among persons with lower area-level measures of SES. As a measure of area-level SES, a higher SED index was clearly and strongly associated with increasing levels of ambient ozone and PM2.5. Utilizing pollution data from over 1,000 ZIP codes, the NETT study allowed us to assess differential ambient exposures on a national scale (Figure 3). Unlike many previous studies that examined air pollution disparities in the United States, our study is one of the few to consider the effects of Census-based area-level measures of SES on differential pollutant exposures. To date, it is also the only study to employ data from a cohort of individuals with severe respiratory disease. Although our study does not explicitly focus on the health effects related to differential exposures, it provides a preliminary estimate of the influence of SES factors on health in the context of a ubiquitous environmental risk factor, air pollution. In a group of already susceptible subjects, this differential exposure may be of particular concern in the evaluation of health outcomes.

Distribution of ZIP Codes for NETT Participants. Number of ZIP codes=1,128.NETT: National Emphysema Treatment Trial.
Environmental justice is usually defined in terms of differential exposure and differential susceptibility. As we studied an already vulnerable population, we could not assess differential susceptibility in our study. However, using the pathways illustrated in Figure 4, we can see how the presence of differential exposure in our study could relate to differential susceptibility in a healthy but otherwise similar population. Social epidemiologists have postulated that area-level factors exert independent effects on health outcomes. 20 Area-level indicators of SES may represent environmental factors such as safety, crowding, availability of healthy food sources, and a sense of community. One or both of these factors could influence differential air pollution exposure risk and differential susceptibility. Those with a lower area-level SES may also be more likely to experience disproportionately higher levels of ambient air pollution exposures due to closer residential proximity to high traffic roadways and industrial sites.1,3,6
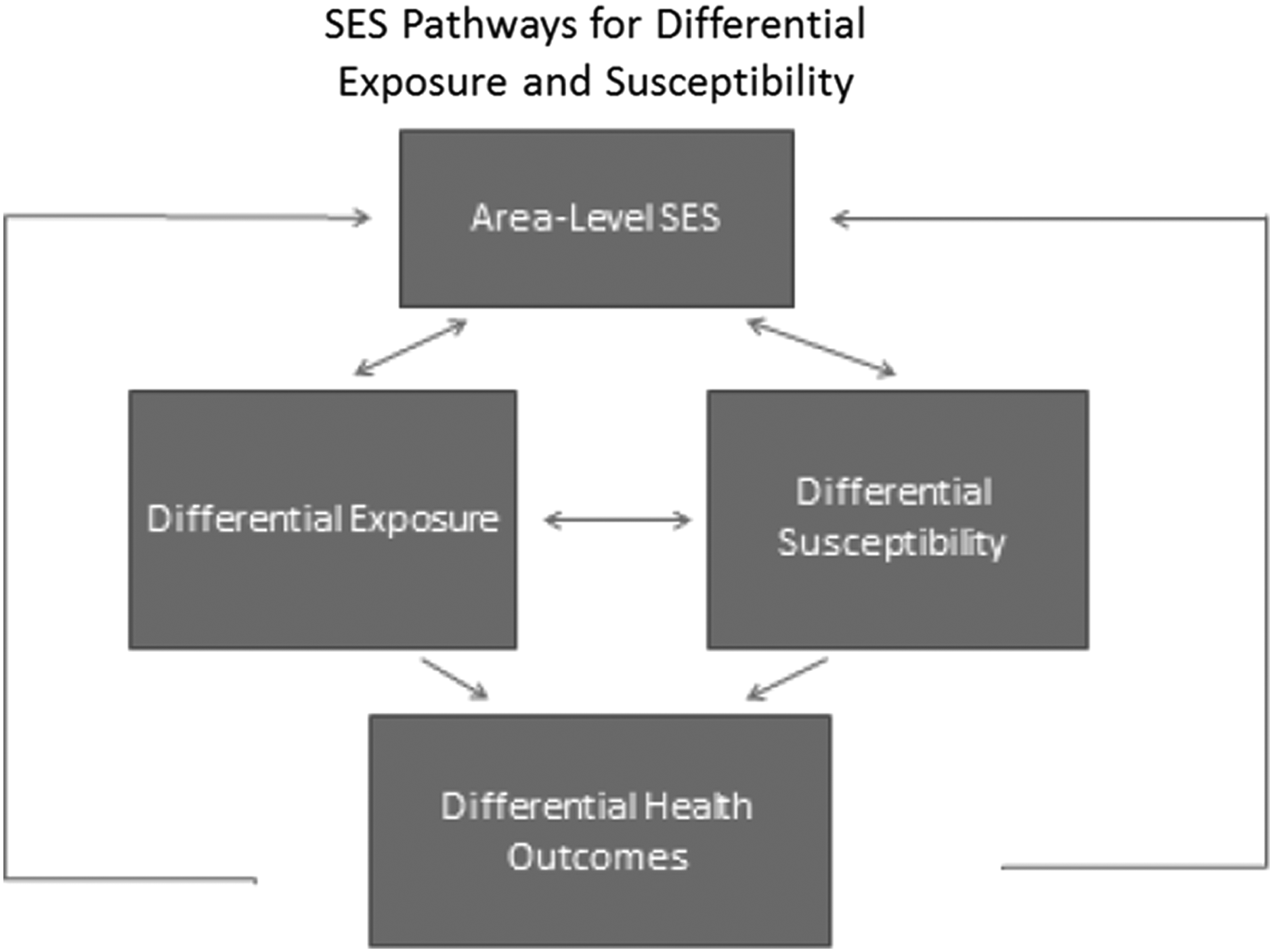
Area-level SES pathways for differential exposure and susceptibility. SES: socioeconomic status.
Comparing our findings to other studies, we found similarities in terms of overall conclusions. Studies by Marshall et al. and Su et al. reported a disproportionate burden of air pollution exposure among lower-income groups.21,22 A study by Young et al. described differential hazardous air pollution (HAP) exposures with respect to urbanization and neighborhood-level SED, reporting increasing exposure hazards with increasing levels of SED. 23 Despite similar findings, several of the existing studies have focused on the relationship between SES and proximity to hazardous sites and facilities rather than with summary measures of exposure. 6 In addition, these studies have tended to focus on relatively small geographic areas and disparate group level variables (e.g., census tract), thereby making direct comparisons problematic.
Strengths
Our measure of air pollution exposure was particularly well-suited for this type of study. Typically, spatial autocorrelation is a limitation that is often present in other environmental studies. Air pollution data are particularly subject to this limitation since measures of air quality in nearby communities are not independent of each other. The term spatial autocorrelation in the context of air pollution can be aptly described with the statement “everything is related to everything else, but near things are more related than distant things.” 24 Failure to account for this spatial autocorrelation would bias the results by assuming independence in air pollution values when in fact there is not. Our study, which relies on kriged air pollution data, is not subject to this limitation. The kriging methodology is highly dependent on the spatial autocorrelation structure in the data for its prediction or interpolation of air pollution values.25,13,24 Secondly, we chose to evaluate air pollution exposure with a cumulative rather than a mean value. Using a cumulative measure allowed us to take into account all the daily exposure data as well as capture ranges of low to high exposure concentrations. Relying strictly on a mean value would mask some of the extreme values especially since we are dealing with several years' worth of pollution data. Lastly, the large geographic area covered by the NETT study participants also allows for the generalizability of our findings to populations across the U.S.
Limitations
Although we observed an association between area-level SES and air pollution exposure, we could not assess a similar relationship between individual measures of SES and differential air pollution exposure. Since our exposure was obtained at the ecological level, we could not include individual level measures of SES in our regression analyses. However, since ambient pollutant concentrations were kriged to the centroid of the ZIP code, assessing the relationship between individual-level SES and ZIP code-level concentrations could have been subject to considerable bias. The largely small cluster sizes, ranging from one to three, may have not been representative of the individuals residing within that ZIP code. Since our sample population tended to be largely Caucasian, older, and male, it is likely that their individual-level SES characteristics could have differed considerably from others in their ZIP codes.
As stated previously, much of the literature on environmental justice has been based on ecological or aggregate data. Dependence on ecological data to assess evidence of differential exposure or susceptibility limits one's ability to extrapolate results to the individual level. Control for confounding is also difficult when dealing with purely ecological data, since adjusting for confounders in group level data can be subject to bias or misspecification. 26 Confounders at the group-level may not be confounders when examined at the individual-level and the examination of individual-level variables as confounders or effect modifiers cannot be evaluated in strictly ecological studies. 27 Employing two separate measures of SES in our study would have permitted the multilevel specification of individual and contextual effects on differential exposures.
One important limitation associated with using ZCTAs to evaluate ZIP code-specific SES characteristics for NETT participants is that although they share the same designation, there is no clear spatial correlation between ZCTAs and ZIP codes. 16 In addition, there are several pitfalls in utilizing ZIP codes as geographical units of analyses. ZIP code boundaries can overlap, be included within other ZIP codes or may be discontinued or newly created over time. 28 They can also encompass vast geographical areas and have an average population of approximately 30,000. The development of ZCTA codes as Census groupings arose as a result of the increased use of ZIP codes by public health researchers and investigators.15,28 ZCTA codes, unlike ZIP codes, are restricted to Census block groups (average population: 1,000). 28 In terms of our study, there is potentially significant spatial mismatch in the individuals selected and their representation within the given ZIP code. It is possible that they may reside in an area assigned one ZCTA code but may actually have a different ZIP code. Area-level SES designations may then be inaccurate for these individuals.
The lack of racial/ethnic diversity in our sample did not allow us to assess racial disparities in exposure. Although important, racial and SES inequalities are not strictly functions of one another. Much of the literature on social disparities emphasizes the importance of distinguishing between SES- and racial-related health disparities. 29 It has been demonstrated that racial minorities are often at increased risk of adverse health outcomes and higher ambient exposures.30,31,32,33,34,35,36 They are also often more likely to have a lower SES. 31 However, studies have shown that SES and race have independent effects on health outcomes and employing one as a proxy for another may be an inadequate analytic choice. 29
Although not the aim of our analyses, we could not infer a causal relationship between SES and differential air pollution exposure. It is often difficult to determine which preceded which—environmental hazards or vulnerable populations. Since region of residence is a non-random selection and land values are typically lower in areas with a greater preponderance of manufacturing plants and waste treatment facilities, it is possible that those from a lower SES would live in areas that contain more of these environmental hazards. 30 It is also possible that noxious facilities may be driven away from affluent neighborhoods into poorer areas. 37
Another limitation of our study is the lack of information on personal exposures. For this research, we relied on kriged ambient air pollutant concentrations as proxies for personal exposure. Spatial heterogeneity in exposure could have impacted how closely these ambient concentrations correlated with personal exposures. In our study however, this limitation may not be as significant since the heterogeneity in the distribution of ambient pollutant exposure varies greatly by pollutant type. Specifically, PM2.5 has been shown to have a rather uniform distribution in urban areas due to the predominant influence of small, long-range transport particles. 38 This is particularly applicable to our study as our sample was largely urban. Like PM2.5, ozone has also been shown to have a homogenous distribution over large areas. 39 Thus, this limitation may be relatively minor within our sample population.
Lastly, our analyses did not consider the potential multiplicative or additive effects of multiple pollutants. Bivariate correlations revealed a moderate association between ozone and PM2.5. However, simultaneous consideration of both pollutants in our model would have been inappropriate, as the availability of pollution data was not equal for both pollutants. Ozone data were available from 1998–2003, whereas PM2.5 were only available from 1999–2003. The disparity in the duration of exposure between pollutants would have complicated controlling for possible interactive effects.
Conclusion
The implications of our study are multifold. We found evidence of an environmental justice equity issue in a vulnerable population. This differential pollutant exposure was shown to be strongly associated with area-level SES. Our study which utilized area-level SES descriptors, over a large geographical area, may enable researchers to more readily compare findings and results. Investigators may also consider applying a similar air pollution kriging methodology in the secondary analysis of health studies with large geographical cohorts. The availability of air pollution data from monitoring databases readily allows for the assessment of differential ambient air pollution in geographically diverse study populations. Specifically, our results speak more directly in support of environmental inequality rather than environmental justice. Characterizing whether this inequality is socially unjust is less clear and subject to further research.
Footnotes
Author Disclosure Statement
The author has no conflicts of interest or financial ties to disclose.