
Abstract
The objective of this study was to evaluate the human health impact of using fluoroquinolones to treat bovine respiratory disease (BRD) in dairy heifers less than 20 months of age. Specifically, this study quantified the probability of persistent symptoms in humans treated with a fluoroquinolone, for a fluoroquinolone-resistant Campylobacter, Salmonella, or multidrug-resistant (MDR) Salmonella infection acquired following the consumption of ground beef. To comply with a Food and Drug Administration requirement for approval of enrofloxacin use in dairy heifers, a binomial event tree was constructed following Food and Drug Administration guidance 152. Release was estimated from the slaughter of dairy cattle carrying fluoroquinolone-resistant bacteria attributed to the proposed use in dairy heifers. For exposure, human foodborne exposure to Campylobacter, Salmonella, and MDR Salmonella after consumption of ground beef was estimated. The consequence assessment included illness, fluoroquinolone treatment, and persistent symptoms in patients treated with a fluoroquinolone. Using best available data to estimate the parameters and probabilities of each event, stochastic simulation was used to represent uncertainty and variability in many of the parameters. A scenario analysis was performed to evaluate the uncertainty of the following parameters: (1) probability of resistance development in treated animals, (2) portion of illnesses attributable to ground beef, and (3) probability of persistent symptoms in patients 18 years of age and over treated with a fluoroquinolone. The population at risk was restricted to people 18 years of age and over, as fluoroquinolones are not labeled for treatment of gastroenteritis in children. The mean annual increased risk of cases in the U.S. population (18 years of age and over) where compromised fluoroquinolone treatment resulted in persistent symptoms was estimated to be 1 in 61 billion (one case every 293 years) for Salmonella, 1 in 33 billion (one case every 158 years) for MDR Salmonella, and 1 in 2.8 billion (one case every 13 years) for Campylobacter.
Introduction
T
Risk assessments have become an integral part of the approval process for antimicrobial drugs used in food-producing animals, and are required by the U.S. Food and Drug Administration's (FDA) Center for Veterinary Medicine (CVM) to evaluate the Human Food Safety of a proposed approval. While FDA guidelines outline a qualitative approach (FDA CVM, 2003a), we used a quantitative, event tree approach. A similar approach has previously been used to evaluate macrolide use in food animals (Hurd et al., 2004).
Enrofloxacin (Baytril®100; Bayer HealthCare LLC, Animal Health; Shawnee Mission, KS) was approved by the CVM in July 1998 for use in cattle for the treatment of bovine respiratory disease associated with Mannheimia haemolytica, Pasteurella multocida, and Histophilus somni. The original approval excluded the use of enrofloxacin in cattle intended for dairy production.
The objective of this study was to evaluate and quantify the human health risk of a new use for a commercially available fluoroquinolone in dairy heifers <20 months of age. The specific use would be only for treatment of respiratory disease in females <20 months old, as they are nonlactating.
Materials and Methods
A probabilistic risk assessment was conducted using a binomial event tree organized in accordance with the steps described in the U.S. FDA's Guidance Document (GD) 152, which include (1) release, (2) exposure via the foodborne route, and (3) consequence. For release, the emergence or selection of resistant bacteria attributed to the proposed use of enrofloxacin in dairy heifers was estimated. For exposure, human foodborne exposure to Campylobacter, Salmonella, and multidrug-resistant (MDR) Salmonella after consumption of ground beef was estimated. The consequence assessment included illness, fluoroquinolone treatment, and persistent symptoms in patients treated with a fluoroquinolone. Available data were used to estimate the parameters and distributions of each event. The population at risk was restricted to 18 years of age and over, as fluoroquinolones are not labeled for use to treat gastroenteritis in children.
Antimicrobial susceptibility testing results
Antimicrobial resistance guidelines used in this study were based on the laboratory results taken from published peer-reviewed journal articles referenced in this article. When testing details were provided, the laboratories conducting the tests followed the procedures used in the National Antimicrobial Resistance Monitoring System (NARMS) testing program and were current for the time of their studies. The interpretive criterion for susceptibility testing Salmonella spp. for fluoroquinolones is ≤1, 2, and ≥4 μg/mL for susceptible, intermediate, and resistant isolates, respectively. The same interpretive criterion is used for Campylobacter even though there are no approved CLSI/NCCLS laboratory standards (FDA CVM, 2003b, 2003c; USDA ARS, 2003).
Modeling approach
A quantitative, event tree modeling approach was used for this risk assessment. Event tree models typically identify sequences of events leading from an initiating event (animal antimicrobial use) to human health risk. In this model, the probabilities were modeled as either deterministic or stochastic parameters, depending on data reliability and availability. Deterministic parameters were represented by single, discrete point estimates, whereas stochastic parameters were represented by statistical distributions. Monte Carlo simulations were performed to create probability distributions of the model outcome (i.e., the “risk”). The model was built, and simulations performed using Microsoft Excel® 2002 (Microsoft Corp., Redmond, WA) and @Risk® 4.5 (Palisade Corp., Ithaca, NY). The outcome was defined as fluoroquinolone-resistant Salmonella or Campylobacter infections in humans resulting in persistent symptoms after physician treatment with fluoroquinolones.
Three unique features of this model were (1) potential transfers of fluoroquinolone-resistant foodborne bacteria from fluoroquinolone-treated dairy heifers to untreated cows and heifers within a farm, due to commingling; (2) potential transfers of fluoroquinolone-resistant foodborne bacteria from dairy heifers originating from farms with fluoroquinolone-treated dairy heifers to other farms that may acquire those animals, and that may as a consequence harbor fluoroquinolone-resistant foodborne bacteria; and (3) cross-contamination, during the mixing process, of ground beef containing fluoroquinolone-resistant pathogens originating from treated dairy heifers <20 months of age with ground beef free of fluoroquinolone-resistant foodborne pathogens.
The model simulated the effect of potential resistance transfer between animals and farms, regardless of the mechanism of resistance development within the treated animal. It modeled the spread between animals by allowing untreated herd mates to develop resistance and by modeling the movement of treated animals to other herds not using enrofloxacin with subsequent resistance spread to cows.
Summary of assumptions
Key assumptions made in the model are presented below. Most are conservative, that is, risk increasing. Ground beef is the major route of concern since pathogens in milk will be inactivated by pasteurization. Whole cuts are infrequently contaminated and usually cooked sufficiently. This assumption was consistent with FDA guidance via personal communication. MDR Salmonella are similar to other Salmonella except for the on-farm prevalence; the probability that a person will get ill from contaminated ground beef; the probability that the ill person will seek medical attention and be prescribed an antibiotic; and the probability that persistent symptoms will occur. With the exception of on-farm prevalence, all these parameters were increased compared to other Salmonella. MDR Salmonella illness was modeled as more likely to create illness and a doctor's visit and antimicrobial treatment. All foodborne Campylobacter have a 100% probability of resistance development in treated animals; this is an unrealistic but conservative assumption, due to lack of data otherwise. Background sensitivity/susceptibility for all three bacterial types is 100%; that is, there is no background resistance and all Salmonella or Campylobacter present in treated animals or herdmates could develop resistance due to enrofloxacin use. Fluoroquinolone-resistant Salmonella (excluding MDR) or Campylobacter have the same likelihood of creating illness as their susceptible counterparts. The number of illnesses resulting from consumption of contaminated meat is roughly proportional to the amount of contaminated meat consumed. No modeling of dose–response relationships was directly included due to lack of data on the doses presented to the consumer.
The last assumption is similar to that used by FDA (FDA CVM, 2000; Bartholomew et al., 2005) for the evaluation of the impact on human health of fluoroquinolone-resistant Campylobacter attributed to the consumption of chicken. Although there are other published modeling approaches, this risk increasing assumption provides an upper bound on the estimates (Cox, 2005). FDA evaluated the impact of historical fluoroquinolone use in chickens and it was assumed that all currently observed resistance to fluoroquinolones on the carcasses of chickens was due to use of fluoroquinolones in chickens. However, for this analysis, fluoroquinolones had not been approved previously for use in dairy cattle intended for milk production of any age. Therefore, current fluoroquinolone resistance in Campylobacter spp. and Salmonella spp. could not be attributed to use of fluoroquinolones in dairy heifers <20 months of age (Fig. 1).
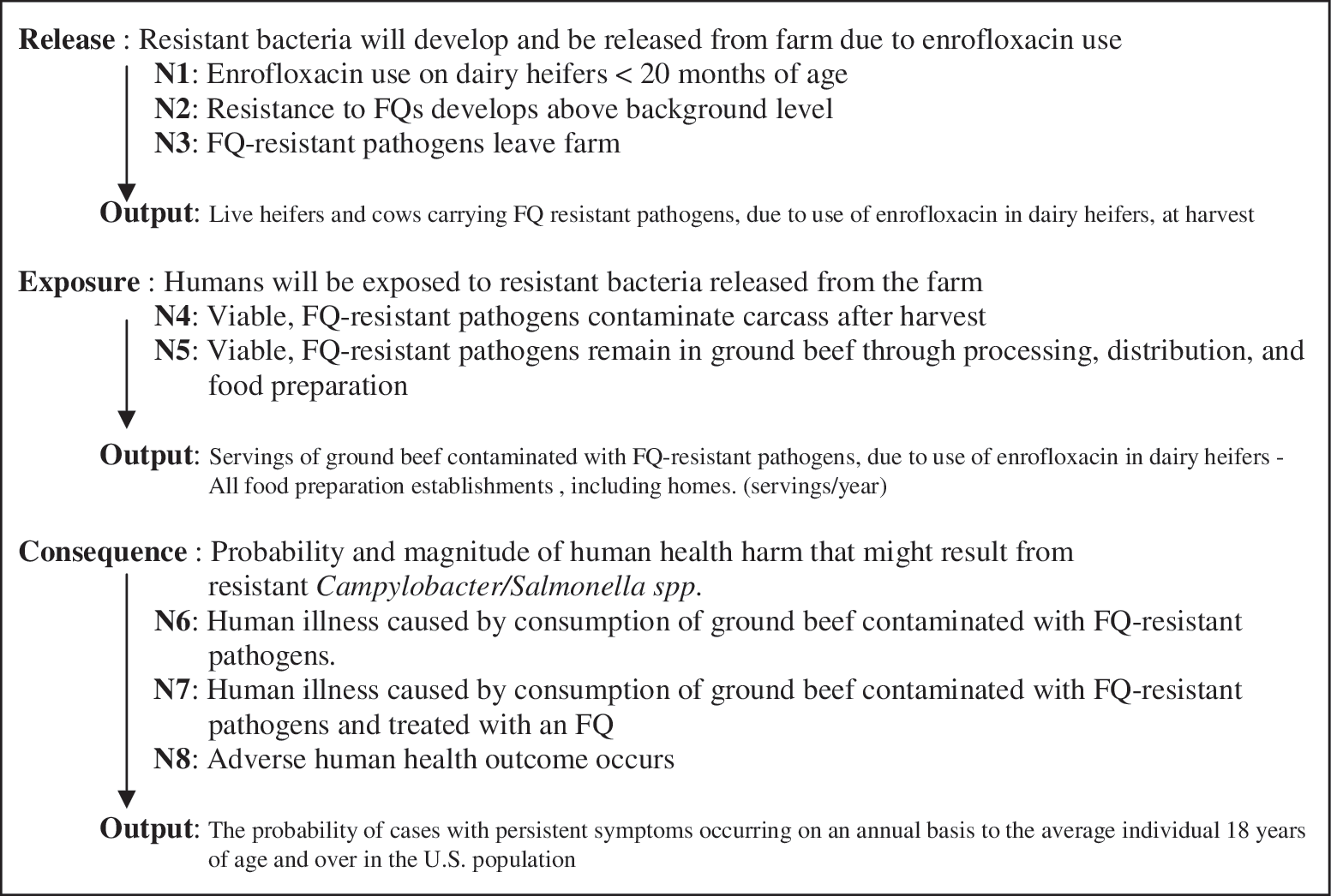
Release
Node 1 (Table 1) is the initiating event of enrofloxacin treatment of dairy heifers <20 months of age for respiratory disease. Node 2 (Tables 2 and 3) is development of resistance in Salmonella or Campylobacter residing within the treated heifer, as a function of the bacterial prevalence and the probability of resistance development in those bacteria. The potential for resistant organisms to pass through the herd, including milking cows, not just treated animals, through commingling with treated dairy heifers was evaluated. Commingling increases risk by increasing the number of animals that may eventually carry resistant organisms or plasmids when heifers and cows go to market. Additionally, it considers the possibility that herds receiving animals from treated herds may be exposed to resistant bacteria after commingling with the purchased animals. Output from Node 2 is the number of live animals (cows and heifers) in treated and untreated herds that may be carrying resistant organisms. In Node 3 (Table 4) resistant bacteria leave the farm in cows or heifers as they are culled to the slaughter market. In agreement with FDA, milk was not considered as a release route, as pasteurization will kill the bacteria of concern (Walstra et al., 2006).
MDR, multidrug resistant.
Exposure
In Node 4 (Table 5), viable resistant bacteria remain on the carcass after slaughter. The output of Node 4 is the number of carcasses contaminated with fluoroquinolone-resistant organisms. Node 5 (Tables 6 and 7): the most likely route of delivering resistant bacteria from beef carcasses through processing, distribution, and preparation to the consumer is through ground beef. Node 5 estimates the number of servings that will be contaminated with resistant bacteria delivered to the consumer fresh via retail or cooked via food manufacturing, food service, and quick serve restaurants. Other data that can be applied to this parameter for Salmonella include the NARMS retail data. However, given the low number of Salmonella and Campylobacter isolates, in this study, NARMS data were considered as supplementary evidence showing a very low probability of resistance development in treated cattle. The NARMS retail meat sampling data reported only 19 Salmonella isolates and 1 Campylobacter isolate from 1522 ground beef samples in 2002 and 2003; none were resistant to ciprofloxacin (FDA CVM, 2003b, 2003c).
Consequence
In Node 6 (Table 8) ground beef from meat that has not been properly handled or prepared is consumed and causes illness, and in Node 7 (Table 9) the ill person (18 years of age and over) is treated with a fluoroquinolone-class antibiotic. In Node 8 (Table 10) symptoms persist when human illness is treated with a fluoroquinolone. The outcome of Nodes 6 through 8 is the number of cases of human illness where persistent symptoms occurred after treatment with a fluoroquinolone and where illness was caused by consumption of ground beef contaminated with fluoroquinolone-resistant Campylobacter or Salmonella due to use of enrofloxacin in dairy heifers <20 months of age.
FDA, Food and Drug Administration.
Sensitivity analysis was performed to estimate the effect of uncertainty of some assumptions on the final results. Three parameters were evaluated by running 27 alternative scenarios for each bacteria using high, medium, and low estimates for each parameter. These included (1) Node 2, combinations of observed resistance to fluoroquinolones in animals treated with enrofloxacin (% of positive animals carrying resistant isolates), Campylobacter (100%, 75%, and 50%), Salmonella, and MDR Salmonella (100%, 20%, and 2%) with observed resistance to fluoroquinolones in animals not treated with enrofloxacin (% of positive animals carrying resistant isolates) Campylobacter (20%, 15%, and 10%), Salmonella, and MDR Salmonella (16.8%, 3.3%, and 0.3%); (2) Node 6, the ratio of illnesses attributed to beef per contaminated serving of ground beef after food preparation, Campylobacter (0.0062, 0.0005, and 0.0028), Salmonella (0.0324, 0.0056, and 0.0165), and MDR Salmonella (0.3284, 0.0566, and 0.1656); and (3) Node 8, probability that symptoms persist when human illness is treated with a fluoroquinolone for each parameter, Campylobacter, Salmonella, and MDR Salmonella (100%, 10%, 36%). The alternative scenarios were run using baseline values for all other parameters in the model.
Results
Table 11 summarizes the estimated risk of fluoroquinolone treatment failure (persistent symptoms) in humans treated for foodborne diseases resulting from consumption of ground beef originating from dairy heifers treated with enrofloxacin. Results are reported in two forms: expected frequency of a treatment failure case in the at risk population (18 years and older) and probability of the event happening to the average person in that population.
Baseline and worst-case scenario results are based on conditions and population assumptions at the time of the analysis.
Baseline scenarios
For Campylobacter the model predicts that on average one case of persistent symptoms would occur every 13 years using the baseline scenario. The mode for all simulations was one case every 18 years; 50% of all simulations predicted a risk of less than the mode. The 95% confidence interval on this distribution was one case every 38.3 years to every 6.5 years. The left skewed distribution shows that there is a remote chance of one case every 4 years for the baseline scenario.
For Salmonella the model predicts that one case of persistent symptoms would occur every 293 years, on average, using the baseline scenario. The mode for all simulations was one case every 501.2 years. The 95% confidence interval on this distribution was one case every 129.3 to every 1060.8 years.
For MDR Salmonella the model predicts that one case of persistent symptoms would occur every 158 years, on average, using the baseline scenario. The mode for all simulations was less than one case every 292 years. The 95% confidence interval on this distribution was one case every 67.8–647.2 years.
Worst-case scenarios
Worst-case scenarios are reported where all treated animals develop resistance, where underreporting, attribution, and carcass contamination are at their maximum, and where the probability of persistent symptoms in treated patients is 100%.
The worst-case scenario for Campylobacter estimates a mean risk of only one case every 2.2 years. The upper-bound (95th percentile) estimate from the worst-case scenario shows that one case of persistent symptoms might occur every 1.1 years, a risk of 1 in 210 million and qualitatively describable as “very low.”
The worst-case scenario for Salmonella estimates a mean risk of one case every 1.4 years. The upper-bound (95th percentile) estimate from the worst-case scenario shows one case of persistent illness every 0.7 years
The worst-case scenario for MDR Salmonella estimates a mean risk of one case every 0.8 years. The upper-bound (95th percentile) estimate from the worst-case scenario shows one case of persistent illness every 0.4 years.
Discussion
Multiple conservative, parameter estimations were used throughout the model. Some of the parameters, such as attribution (Node 6), resistance development in untreated herd mates (Node 2), and probability of persistent symptoms (Node 8), should be at or near zero. Unrealistically, this model did not place much of the probability density near zero. Therefore, the mean frequency baseline results shown in Table 11 should be viewed as upper bounds on the risk or worst case.
Additionally, the multiple scenarios simulated showed that even with all the worst case and unlikely assumptions we made, the risks were very low. For example, the worst case assumes that MDR Salmonella would always (100%) develop resistance in treated heifers, are 10 times more likely to cause human illness, and would always (100%) produce persistent symptoms in treated patients. Clearly, these are unrealistic assumptions, especially given the low to zero levels of ciprofloxacin resistance being reported by NARMS after Baytril100 use in beef cattle since 1999 (FDA CVM, 2003c).
The sensitivity analysis showed that results were most sensitive to changes in Node 6 (Ratio of Illnesses Attributed to Beef per Contaminated Serving of Ground Beef Following Food Preparation). Assumptions made about the portion of all foodborne illness attributable to a specific commodity should be made carefully. This finding is not surprising given that this one parameter reflects many illness impacting processes such as handling, cooking, and bacterial dose. Additionally, the importance of this parameter demonstrates the important role of standard food hygiene practices in reducing antibiotic resistance risk. Risk would increase if there were to be a highly virulent and prevalent pathogen whose source was predominately meat.
The approach used in Node 6 (Table 8) relies upon what is observed and known about the level of foodborne illness attributed to ground beef relative to the estimated number of servings of ground beef that were contaminated with each of the foodborne pathogens modeled. It assumes that the number of illnesses resulting from consumption of contaminated meat is roughly proportional to the amount of contaminated meat consumed if the level of contamination is held fixed (Bartholomew et al., 2005). Key processes between the farm and the consumer were modeled to project the relative increase in the number of servings of ground beef contaminated by fluoroquinolone-resistant Campylobacter, Salmonella, or MDR Salmonella. The ratio of illnesses attributed to beef per contaminated serving of ground beef after food preparation is modeled in a separate spreadsheet used to perform a separate Monte Carlo simulation to estimate a distribution for this ratio. The distribution was then sampled to run the main model.
We do not distinguish among different levels of contamination (e.g., 1 CFU per ton, which might cause no harm, vs. 1 billion CFUs per oz, which presumably would be much more hazardous). In reality, it is plausible that average levels of contamination cause little or no harm, and that our estimates are upper bounds, driven by occasional pockets of high concentrations, rather than by average levels of contamination.
The purpose of Node 1 was to estimate the number of dairy operations where Baytril100 would be used if approved for respiratory disease treatment in dairy heifers <20 months of age. It is important to understand the structure of the U.S. dairy industry and the management of replacement heifers to understand the potential risk of Baytril100 use in dairy replacement heifers; heifers are raised to enter the milking herd, not the food chain. Very few dairy heifers are sold for slaughter because of their value for milk production and breeding. Most illness and treatment occurs during the first few months of life, long before they begin milking. Heifers are commingled with others of similar age and are sometimes sold to other farms. Heifers are often kept in separate facilities from milking cows until the time of their first calving when milking begins.
MDR serovars of Salmonella such as Newport and Typhimurium DT104 are of concern to human health for two reasons. They are thought more likely to acquire resistance to antibiotics like enrofloxacin and to cause human illness that is difficult to treat. To address these concerns, it was assumed that any MDR Salmonella would have a higher probability of resistance acquisition on-farm. Additionally, two other parameters were increased compared to nonresistant Salmonella: the probability that an ill patient will seek medical attention and the probability that an antibiotic will be prescribed (Node 7).
Uniquely, this model considers not only the development of resistance in treated herds, but also the transfer of resistant bacteria or genetic determinants through the movement of cattle to operations that are not using enrofloxacin. Other models focus on resistance development in treated animals only.
Our model focused on foodborne transmission of fluoroquinolone-resistant Salmonella and Campylobacter via ground beef. Routes of transmission other than foodborne were not considered in the model because the majority of dairy cattle meat goes into ground beef and pasteurization eliminates pathogens in milk (NCBA, 2004; Walstra et al., 2006).
Quantitative risk assessment is a widely used method to evaluate the probability of specific hazards and guide policy decisions. For this model we used an event tree approach that allowed inclusion of stochastic elements to account for biological variability and uncertainty for key parameters. Models, quantitative or qualitative, always have weaknesses. The key question is whether these weaknesses consistently over- or underestimate (bias) the risk. We used several approaches to insure that the model results would represent conservative (higher) risk estimates, to evaluate the effect of parameters for which little scientific data were available and to account for indirect transmission pathways.
This study was conducted to fulfill CVM's requirement to complete a risk assessment for all new antimicrobial products and uses. The model presented in this article takes into account any potential resistant organisms introduced into the dairy herd from treated heifers, including spread through commingling with the potential of entering the food supply from slaughtered dairy cows.
While FDA GD 152 recommends a qualitative risk assessment approach, the “FDA does not intend to exclude quantitative risk assessment in favor of a qualitative process” (FDA CVM, 2003a). The qualitative risk of using injectable antimicrobials in treating individual food-producing animals is inherently low. When reliable information is available, the use of a quantitative model allows a detailed study of multiple risk factors. Since fluoroquinolones are considered critically important to human health, the merging of quantitative estimates with qualitative classifications allows reviewers to gain additional insight into the magnitude of qualitative risk classifications.
Conclusions
Mean annual risk estimates of 1 in 2.8 billion, 61.4 billion, and 33.1 billion for Campylobacter, Salmonella, and MDR Salmonella, respectively, can be considered qualitatively very low. These estimates are arguably conservative and upper-bounded due to the multiple conservative parameter estimates incorporated into the model such as the inclusion of resistance spread to commingled and untreated herd mates, the potential movement of resistance bacteria with sold dairy heifers, and the mixing of ground beef. This modeled risk is hypothetical and the actual risk could well be even lower.
Footnotes
Acknowledgments
Special thanks go to Pam Triplett and Ruth Lamley, Bayer Animal Health, for input on organization of the article and references and Sasidhar Malladi, Iowa State University, for mathematical modeling assistance.
Disclosure Statement
At the time the Risk Assessment was conducted, Drs. Hurd, Holtkamp, Dickson, and Warnick were paid by Bayer Animal Health as Consultants and Dr. Vaughn was employed by Bayer Animal Health. Dr. Vaughn was paid by Bayer Animal Health to oversee the writing and submission of this paper, after retiring from Bayer Animal Health.