
Abstract
During May and June 2009 an outbreak of Cyclospora cayetanensis infection involving 12 laboratory-confirmed and 6 probable cases was detected in Stockholm County, Sweden. Imported sugar snap peas from Guatemala were the suspected vehicle, based on information obtained from patient questionnaires. This is the first reported outbreak of cyclosporiasis in Sweden and the second in Europe.
Introduction
C
Methods
Outbreak investigation
In June 2009, seven cases of Cyclospora infection were identified at the Karolinska Solna University Laboratory, Stockholm, Sweden. Since, only four to five cases are usually diagnosed at this laboratory each year, a request was sent to the other three parasitological laboratories in Stockholm to report any cases of cyclosporiasis to the Department of Communicable Disease Control and Prevention. The same request was made by the Swedish Institute for Infectious Disease Control (SMI) to the majority of laboratories in Sweden that perform parasitological analyses. Seven further cases of Cyclospora infection were subsequently reported from the three laboratories in Stockholm County. Consequently, a total of 14 cases were identified. No additional cases were reported by laboratories outside of Stockholm County.
A questionnaire was sent by post to all 14 patients with a laboratory-confirmed diagnosis of Cyclospora. Because previously reported outbreaks of Cyclospora infections in other countries were linked to imported fresh fruit and vegetables (Mansfield and Gajadhar, 2004; Warren, 2009; Ortega and Sanchez, 2010), detailed questions regarding their consumption of these products and from which stores they were bought were included in the questionnaire. Questions about symptoms, travels abroad 14 days before symptoms, and if any household contact had developed gastrointestinal symptoms during the same period were also included. If a household contact had developed symptoms, the question was raised if the contact had been abroad 14 days before onset of symptoms. The response rate was 100%.
Case definitions
A confirmed domestic case was defined as a patient with onset of gastrointestinal symptoms during 23 May to 3 June and in whom Cyclospora oocysts were detected in a stool sample and who had no history of travel abroad 14 days before the appearance of symptoms.
A probable domestic case was defined as a household contact of a confirmed case who had both developed gastrointestinal symptoms and consumed the same food during 23 May to 3 June, had not been abroad 14 days before the appearance of symptoms, and had not been tested for Cyclospora infection.
Microbiological analyses
The initial diagnosis was performed by routine microscopy of wet mounts after formol/ethyl acetate concentration and based on the identification of unsporulated oocysts compatible in size and shape with those of Cyclospora. Available samples from 10 of the patients were sent to SMI for complementary analyses. Cyclospora oocysts were confirmed by SMI in all of these 10 samples both by modified Ziehl-Neelsen staining and ultraviolet fluorescence microscopy (Mansfield and Gajadhar, 2004).
Besides routine parasitological examination, fecal specimens were also cultured for bacterial enteropathogens (Campylobacter, Salmonella, Shigella, and Yersinia enterocolitica) with the use of standard methods.
Results
Questionnaire study
Of the 14 laboratory-confirmed cases, 12 (8 women and 4 men) had not been abroad 14 days before the infection and thus met the case definition as a confirmed domestic case. Two patients had been in Peru and developed symptoms 6 days after their return to Sweden. It is therefore likely that these two patients acquired the infection in Peru. The median age of the 12 confirmed domestic cases was 48 years (range 16–60 years). They were all healthy and free of gastrointestinal symptoms before this infection. The most common symptoms consisted of diarrhea (100%), nausea (100%), abdominal pain (75%), low-grade fever (66%), and initial vomiting (33%). One patient was hospitalized due to dehydration. Gastrointestinal symptoms had lasted for >2 weeks in all cases when the diagnosis was confirmed.
Six household contacts of laboratory-confirmed cases, who had consumed the same food items, developed gastrointestinal symptoms. These household contacts did not receive a separate questionnaire, but we identified them as probable cases. Since they had recovered when the questionnaires were answered by the confirmed cases, we did not request fecal samples from the household contacts. Moreover, they had not visited any health-care institution because of diarrhea and were thus not tested. All 12 confirmed and 6 probable domestic cases fell ill within the period 24 May and 2 June (Fig. 1).
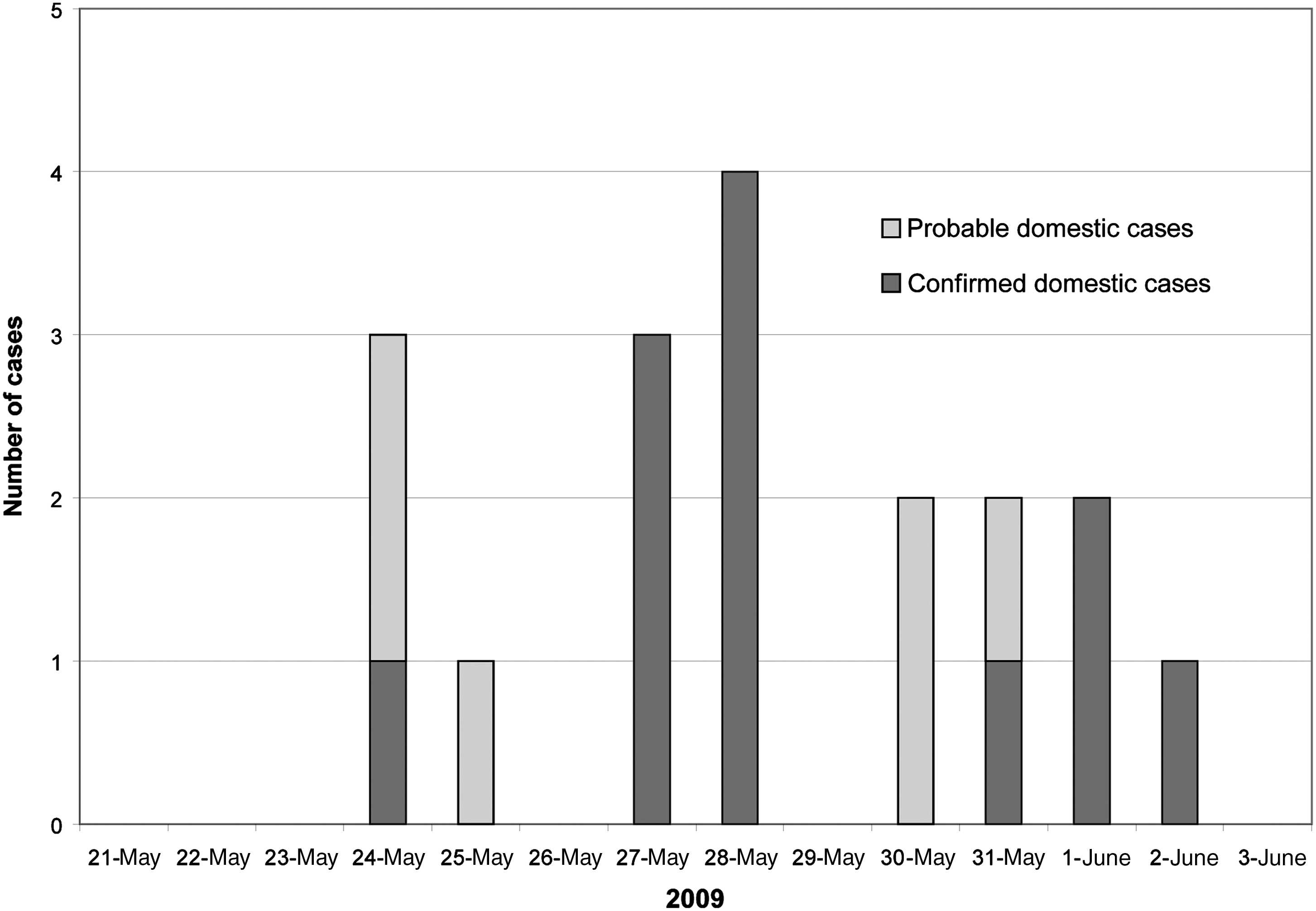
Domestic cases of cyclosporiasis by date of onset of symptoms, Stockholm May–June 2009 (n = 18).
All stool specimens were negative for bacterial enteropathogens.
Environmental analysis
The rates of consumption of different vegetables and fruit in the week before onset of symptoms are shown in Table 1. Eleven of the 12 confirmed cases (92%) and all 6 household contacts had consumed sugar snap peas, which were bought from three different grocery stores belonging to the same chain. The sugar snap peas were eaten raw without any previous heating. One patient was unaware whether he had eaten this food item or not. Only municipal drinking water had been consumed by the patients.
The local environmental health office was informed about the cluster of cases and the results from the questionnaire. Since sugar snap peas was the only food item consumed by almost all the cases, the investigating health officers traced the peas that had been delivered to the different stores between 11 and 23 May. They found that the sugar snap peas were produced in Kenya, Guatemala, and Zambia, and that Guatemala was the only country of origin found in common for all grocery stores named by the patients. No sugar snap peas from Guatemala had been delivered outside of the Stockholm area. Unfortunately, no sugar snap peas from the suspected batches were available for laboratory analysis.
Discussion
The suspected food vehicle for this outbreak was sugar snap peas that had been imported from Guatemala and distributed to food stores in Stockholm County between 11 and 23 May. This suspicion is based on the facts that this food item was consumed by all but one patient (this very patient did not remember if he had consumed sugar snap peas within 2 weeks of onset of disease) and offered for sale only in a limited number of stores, all named by the patients. Moreover, the outbreak affected only the Stockholm County, the only area in Sweden that was provided with Guatemalan sugar snap peas during the time of the outbreak. The study design did, however, not allow any reliable assessment of the source of infection, and a major limitation is that a case–control study was not performed. The focus was rather concentrated on case finding, the geographical distribution of cases, and symptoms. Another limitation is that, unfortunately, no sugar snap peas from Guatemala were left for analysis when the outbreak was identified.
Most reported foodborne outbreaks of cyclosporiasis have been attributed to fruit and vegetables like raspberries, basil, and salad (Mansfield and Gajadhar, 2004; Ortega and Sanchez, 2010). Guatemalan snow peas, which are similar to sugar snap peas, were linked to an outbreak in Pennsylvania in 2004 (CDC, 2004).
This is the second reported foodborne outbreak of Cyclospora infection in Europe. The first outbreak occurred in Germany in 2001, where salad was implicated as vehicle of infection (Kiehl et al., 2001). Sporadic cases have been described in people returning to Sweden from different parts of the world (Lebbad and Linder, 1993), but to our knowledge no domestic cases have been observed until now. Cyclosporiasis is not a notifiable infection in Sweden and the current outbreak would not have been detected if the laboratory personnel had not been observant and voluntarily reported the cluster.
Conclusions
This is the first reported foodborne outbreak of cyclosporiasis in Sweden. Globalization of food supply may contribute to future outbreaks of Cyclospora infections in Europe. Molecular typing and subtyping tools should be developed, standardized, and validated for investigation of such outbreaks. Increased awareness of this disease is needed from food suppliers, the public, health providers, and laboratory personnel.
Footnotes
Disclosure Statement
No competing financial interests exist.