
Abstract
In 2007, Romania, the largest southeastern European country, reported the highest notification rate of botulism cases in the European Union (0.18 per 100,000 inhabitants), which was 18 times higher than the reported rate in the United States (0.01 per 100,000 inhabitants). This report aims to analyze published and unpublished surveillance data on foodborne botulism in Romania from 1980 to 2009 in the context of political and economical changes that occurred in the former communist countries. The mean annual incidence rate of botulism cases was significantly lower during the late communist period, 1980–1989 (0.06±0.03 cases per 100,000 inhabitants), than during the years 1990–1999 (0.1±0.04 cases per 100,000 inhabitants, p=0.01) and 2000–2009 (0.12±0.04 cases per 100,000 inhabitants, p<0.01). The highest incidence rates were registered in 1998 and 2007 (0.18 cases per 100,000 inhabitants), whereas the lowest incidence rate was registered in 1983 (0.02 cases per 100,000 inhabitants). The disease was usually associated with the consumption of home prepared meat products (mainly raw sausages, smoked-dried meat). Most of the laboratory-confirmed cases tested positive for type B toxin (99%). During 2007–2009, the incidence was particularly high in northwestern and western Romania (0.5 and 0.3 cases per 100,000 inhabitants, respectively). The fatality rate was 60% before 1995 and decreased to 12.2±8.5% during 1999–2009. The general ascending trend of infection rates throughout the period studied demonstrates the need for the implementation of correct public health and educational measures to fully prevent this severe disease.
Introduction
B
There are three forms of human botulism: foodborne, wound, and intestinal (infant and adult). Foodborne botulism, the most common form, is caused by eating food containing preformed BoNT. Because C. botulinum is ubiquitous in the environment, spores routinely contaminate food and survive standard cooking practices that do not exceed 100°C. C. botulinum cells produce BoNT only under particular conditions that include an anaerobic, low-salt, low-acid environment. Home-preserved foods often attain these conditions and, therefore, present a high risk for botulism (Varma et al., 2004).
In Romania, the largest southeastern European country (approximately 23 million human inhabitants), botulism became a statutory notifiable disease in 1978, but the first case reports were published in 1968 and 1976 (Vita et al., 1968; Barcan and Pitigoi, 1976).
In 2007, Romania reported the highest notification rate of botulism cases in the European Union (0.18 per 100,000 inhabitants), which was six times higher than the overall notification rate (0.03 per 100,000 inhabitants) (European Centre for Disease Prevention and Control, 2010), and 18 times higher than the rate in the United States (0.01 per 100,000 inhabitants) (Sobel et al., 2004).
This report aims to analyze the surveillance data on foodborne botulism in Romania from 1980 to 2009 in the context of political and economical changes that occurred in the former communist countries.
Materials and Methods
Suspected and confirmed botulism cases are reported to the National Center for Communicable Disease Surveillance and Control in Bucharest, Romania. We have reviewed surveillance data, and published and unpublished reports from 1980 to 2009 (The Epidemiology and Control of Communicable Diseases Unit—National Program for Surveillance and Control of Infectious Diseases, 1998; National Center of Communicable Diseases Prevention and Control, 2008, 2009, 2010; National Institute of Statistics, 2008; Steiner, 2010; World Health Organization, 2010). Outbreaks were not documented separately in the surveillance data.
A case of foodborne botulism is defined as a compatible illness in a person whose serum, stool, or gastric secretions tested positive for the botulinum toxin; a compatible clinical illness in a person who ate food that tested positive for botulinum toxin; a compatible illness in a person who ate food that was also eaten by a person with a laboratory-confirmed case; or a designation of the illness as foodborne botulism by the reporting regional health department (The Commission of the European Communities, 2008).
Statistical analysis was performed using the SPSS version 17.0 for Windows (SPSS, Chicago, IL). Descriptive statistics (percentage, mean±standard deviation) were calculated for each variable as appropriate. Comparisons between subgroups were made by means of Mann–Whitney U statistics for quantitative data. Trends over time for the incidence rates of botulism cases were determined by linear regression analysis. A p-value of less than 0.05 was regarded as statistically significant.
Results
Over a 30-year period (1980–2009), the mean number of cases with botulism was 20±9 per year with a mean annual incidence rate of 0.09±0.04 cases per 100,000 inhabitants. The highest incidence rates were registered in 1998 and 2007 (0.18 cases per 100,000 inhabitants), whereas the lowest incidence rate was registered in 1983 (0.02 cases per 100,000 inhabitants) (Fig. 1). There was a general ascending trend of infection rates throughout the time period studied, and this increase was statistically significant (R 2=0.38, p<0.001) (Fig. 1).
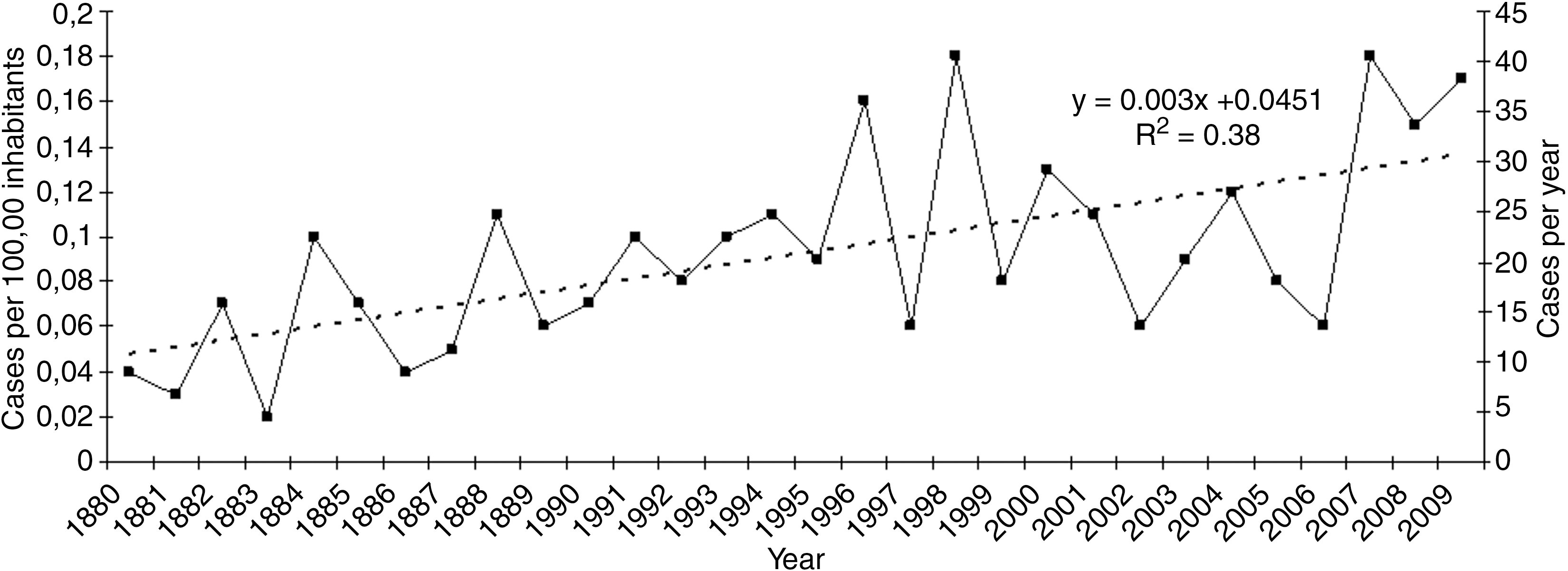
Number of botulism cases and cases per 100,000 persons in Romania, 1980–2009. Data are derived from routine, passive national surveillance. Data are presented as one trendline because the incidence and absolute case count trendlines are indistinguishable.
The mean annual incidence rate of botulism cases was significantly lower during 1980–1989 (0.06±0.03 cases per 100,000 inhabitants) than during 1990–1999 (0.1±0.04 cases per 100,000 inhabitants, p=0.01) and 2000–2009 (0.12±0.04 cases per 100,000 inhabitants, p<0.01).
Of 249 botulism cases diagnosed during the period between 2000 and 2009, 100 (40.2%) were laboratory-confirmed as follows: 99 tested positive for type B toxin and 1 sample was positive for type E toxin (in 2007, related to fish products).
The incidence of botulism cases was three times higher in 2007 than in 2006 (0.18 vs. 0.06 cases per 100,000 inhabitants) and since then the rates have remained constantly high (Fig. 1). During the period between 2007 and 2009, the incidence was particularly high in northwestern and western Romania (0.5 and 0.3 cases per 100,000 inhabitants, respectively) (Fig. 2). The highest mean incidence rates were registered in May and June (0.03 cases per 100,000 inhabitants) and the lowest were registered in October and November (0.003 cases per 100,000 inhabitants) (Fig. 3). Of 106 cases diagnosed during 2007–2009, 86 (81.1%) were associated with the consumption of home-prepared meat products (mainly raw sausages, smoked-dried meat), whereas industrially canned products were involved in 20 cases (18.9%). Most of the patients were in the age group of 15–64 years (86.8%, n=92), followed by those aged 5–14 years (8.5%, n=9) and over 65 years (4.7%, n=5).
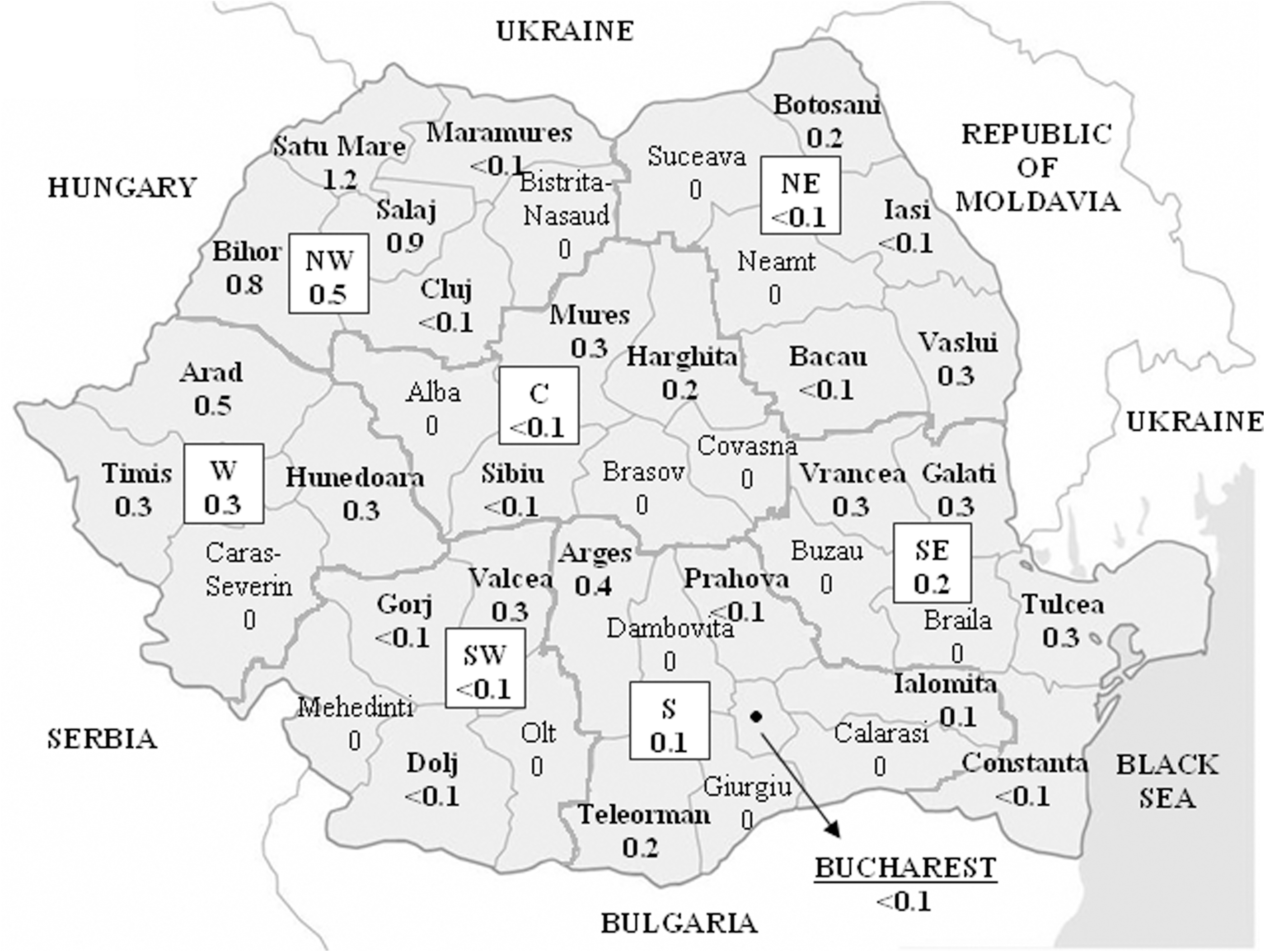
Map of Romania showing the mean annual incidence of botulism cases by county of residence and region per 100,000 persons, 2007–2009. C, central; NE, north-eastern; NW, north-western; S, south; SE, south-eastern; SW, south-western; W, western.
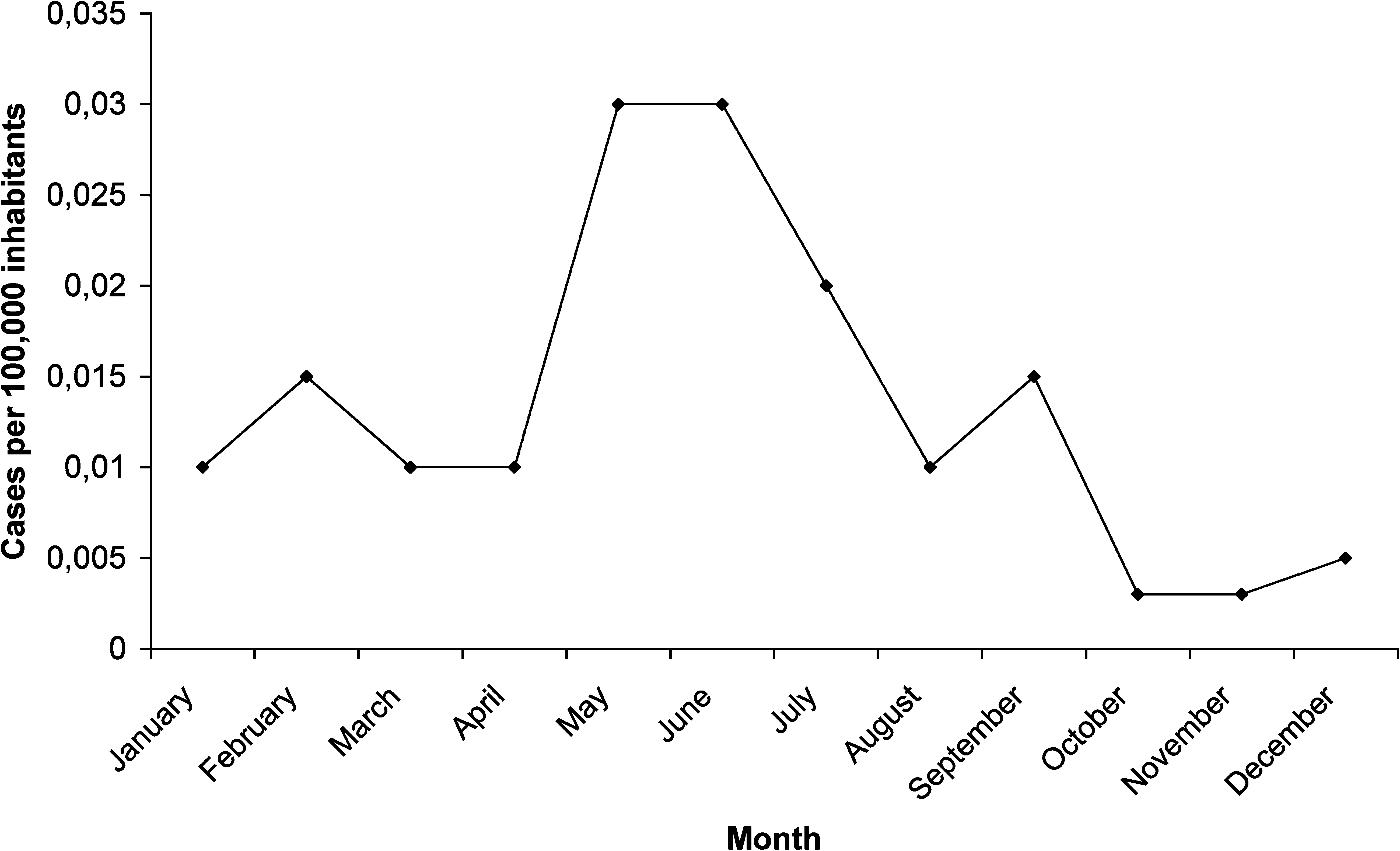
Monthly incidence rates of botulism cases per 100,000 persons in Romania, 2007–2009.
The fatality rate was 60% before 1995, and decreased to 12.2±8.5% during 1999–2009.
Discussion
During the 30-year study period, Romania went through important political and economical changes. The Romanian Revolution of December 1989 overthrew the communist regime. It is assumed that the increased incidence of botulism cases during the early post-communism period of 1990–1999 as compared to the communism period 1980–1989 may be explained by poverty, the main reminiscence of the communism period, which drove more persons to conserve food. A lack of reliable energy sources and cooking supplies made food preservation practices riskier, and food shortage forced people to rely on preserved food for a larger proportion of their diet. Why the rate of botulism increased during 2000–2009 remains unclear. Besides poverty, it may be partly due to the privatization of previously state-run farms and canning factories, where control of the technological processes became less strict.
Similar patterns of ascending trends of infection rates were registered in Azerbaijan (World Health Organization, 2010) and Georgia (Varma et al., 2004; World Health Organization, 2010), countries that declared independence from the collapsing Soviet Union in 1991 (Supplementary Material; Supplementary Data are available online at
In Romania, dependence on traditional products (mainly pork), preferentially home-prepared but also bought from the market, is based on culinary preferences, social factors, and, sometimes, inadequate awareness of attendant risks. The increased incidence rates of botulism registered in late spring and early summer are probably associated with an increased rate of the slaughtering of pigs in private farms and more intensive preparation of home-made products, as, at this time of the year, the winter provisions have usually been consumed. Warm weather facilitates the growth of C. botulinum and the production of BoNT (Dhaked et al., 2010).
Despite the fact that the incidence of botulism cases was among the highest in the western region of Romania during 2007–2009 (0.3 cases per 100,000 inhabitants), this value is four times lower than the figure reported in the same area during 1990–2007 (1.4 cases per 100,000 inhabitants) (Neghina et al., 2010), demonstrating an improvement in the public awareness of the conditions that have led to foodborne botulism in this region of Romania.
In this report, most of the cases with foodborne botulism were young and middle-aged adults. Nevertheless, persons of all ages are potentially susceptible to botulism. Also, there are no gender differences in susceptibility to this infection (Arnon et al., 2001).
The improvement of botulism-related healthcare policies in the early postcommunist period has significantly decreased the fatality rate for this disease in Romania.
Conclusions
Foodborne botulism remains a public health concern in Romania. The general ascending trend of infection rates throughout the time period studied demonstrates the need for the implementation of correct public health and educational measures in fully prevent this severe disease. Culinary, cultural, and social factors that keep the incidence low in some parts of the country should be identified and then translated into a public health message for the high-incidence areas.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.