
Abstract
Anisakiasis is a parasitic disease acquired by humans when ingesting raw or undercooked fish infected with L3 larvae of the nematode genus Anisakis or Pseudoterranova. Here we report the first case of human anisakiasis in China. The patient, male, 56 years old, Dalian citizen, was admitted into the hospital with vomiting, peripheral umbilicus and abdominal distension, and frequent mucous diarrhea. The patient was examined using an electronic gastroscope, which displayed a parasite residing in the stomach, and subsequently gastroscope-assisted surgery was implemented. A white round worm was removed from the patient and stained. It was identified as L3 larvae of Anisakis. After the removal of the L3 larvae of Anisakis, the inflammation symptoms disappeared. As the first report of clinical case of Anisakis infection in China, the morphology of L3 Anisakis larvae from the patient is described and discussed. We conclude that anisakiasis should be considered in patients who have a habit of eating raw fish and who display associated symptoms.
Introduction
A
Case
On May 31, 2010, a 56-year-old male patient was sent to the hospital due to “frequent diarrhea for 1 month.” The patient's case history indicated intermittent abdominal navel distension without apparent inducement during the last 2 years, occasionally accompanied by mucous diarrhea, so the case was primarily diagnosed as colonic polyps, and was not given treatment. However, the patient's symptoms worsened, and he had frequent defecation (seven to eight times/day), accompanied by anal tenesmus and yellow stools without pus and blood. A medical examination of the patient showed body temperature of 36.2°C, pulse of 78 times/min, blood pressure of ll0/85 mm Hg, total white blood cell count of 5.93×109, 30.40% lymphocytes, and 3.5% eosinophilic cells. Abdominal and rectal examinations showed normal results, so this case was suspected as colon cancer. On June 3, 2010, when the patient was hospitalized, medical examination with an electronic gastroscope displayed the duodenal and gastric ulcer, moderate to severe chronic superficial gastritis, and mild sinus atrophy. More importantly, a parasite was observed in the stomach. The parasite was removed by a biopsy forceps (Fig. 1), and after removing the parasite, the patient's inflammation symptoms disappeared.
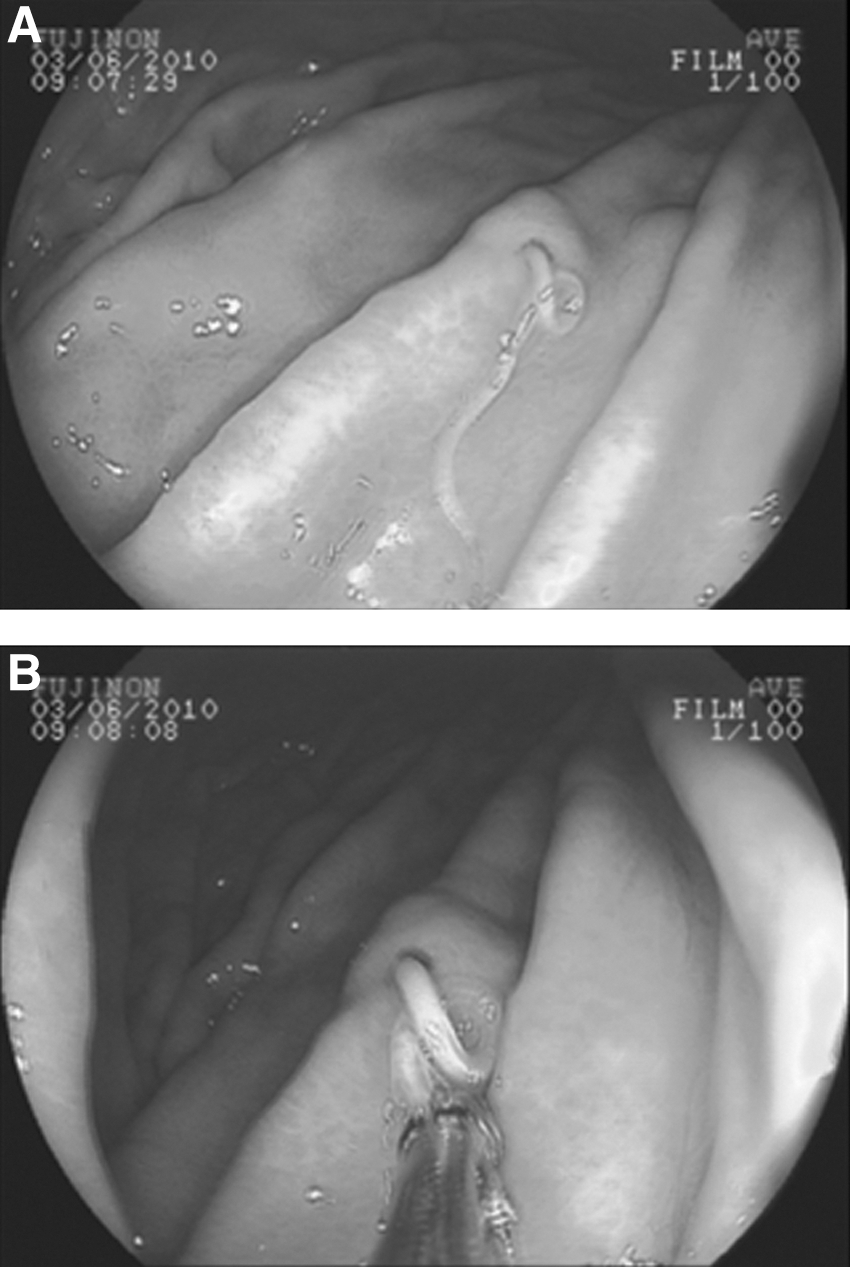
Viewing of Anisakis larvae in the patient's stomach.
Worm Identification
After cleaning the worm body, we observed the parasite under a dissecting microscope, stained the worm by alcoholic hydrochloric acid-carmine method (Snow, 1963), and soaked it in 2% hydrochloric acid alcohol for separation, dehydrated, and mounted on a slide. The worm had a cylindrical, milky white translucent body measuring 29.00 mm in length and 1.00 mm in diameter. The ends of the worm were tapering, most pronounced at the head end. After staining, we observed that the worm body surface had unconspicuous bands, head ridge, fusion of the lip block, and undifferentiated labellum (Fig. 2A). Between the esophagus and bowel, the ventriculus was unconspicuous (Fig. 2B). Larval tail was short, about 0.15 mm, slightly rounded at the top, and there were blurred corner protuberances (Fig. 2C and D). Based on the staining results, this worm was identified as larvae of Anisakis (Lymbery and Cheah, 2007).
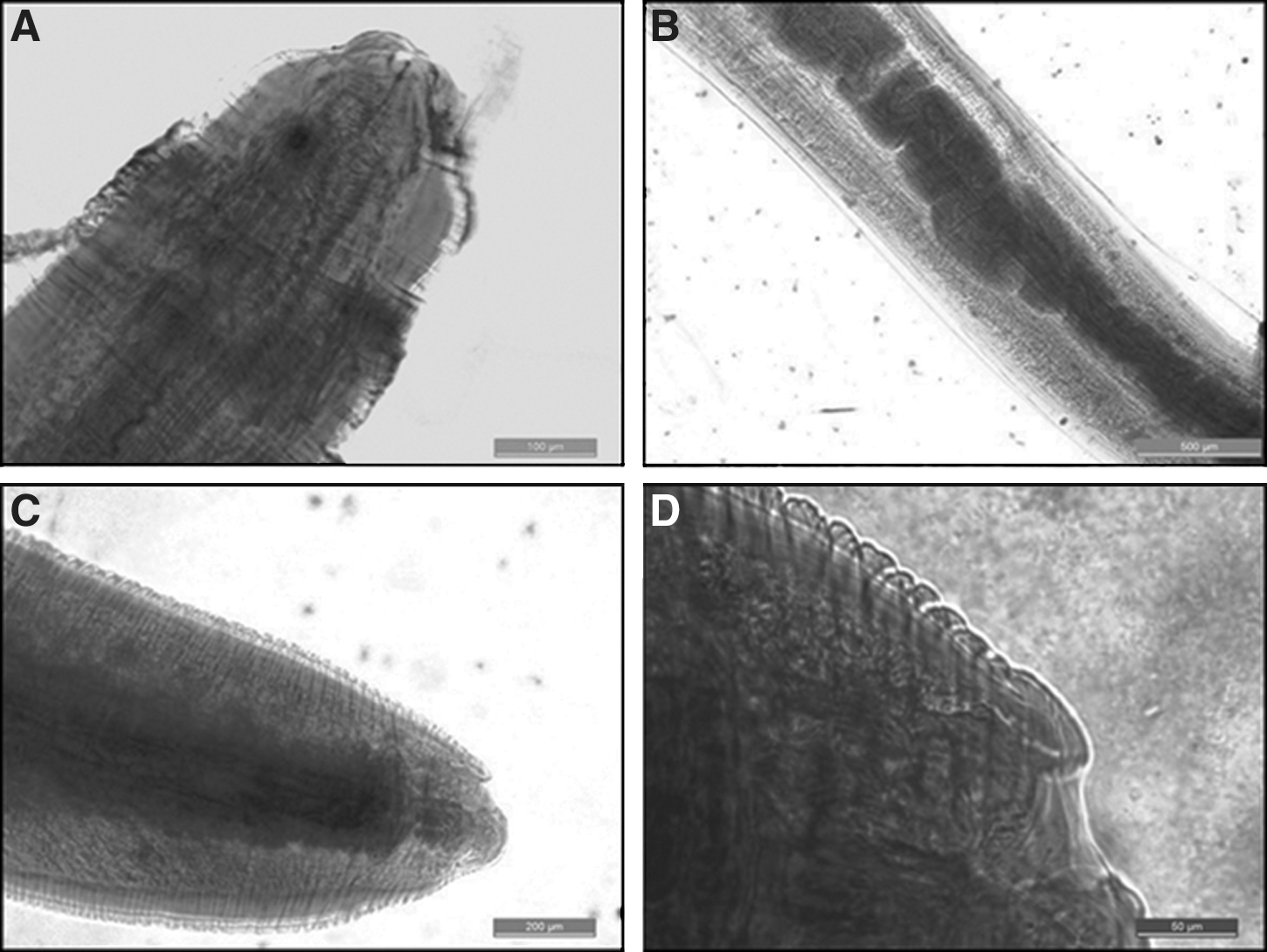
Species identification of the L3 Anisakis larvae.
Discussion
Anisakiasis is a foodborne parasitic disease and is also known as the “herringworm disease.” Ingested larvae can drill into the wall of the digestive tract of people, or migrate to other organs and cause acute symptoms, such as severe abdominal pain, nausea, vomiting, and diarrhea. When worms drill into organs or tissues, the worms are enveloped to form eosinophilic granuloma that can cause allergic symptoms (Kakizoe et al., 1995; Audicana and Kennedy, 2008). The human infection with Anisakis was first described in the 1960s by Van Thiel et al. Human cases were reported from 27 countries including Japan, the United States, South Korea, Holland, Italy, England, France, Germany, and the Pacific areas. Up to 31,000 human cases of Anisakis infection are reported globally (Sakanari and McKerrow, 1989; Desowitz, 1986), and Japan has the highest number, about 14,000 reported cases.
Clinically, symptoms of anisakiasis include functional disorder of the gastrointestinal tract in patients (Smith, 1999). The preliminary diagnosis depends on clinical symptoms of patients and history of eating fresh fish, but for a definite diagnosis, finding the larvae is required. Serological examination is used for chronic anisakiasis diagnosis, but is rarely employed in the acute phase. Kakizoe et al. analyzed 87 cases of gastric anisakiasis data and found that Anisakis is usually in the greater curvature with severe mucosal edema (Kakizoe et al., 1995). The worm infection sites present edema, plica hypertrophy, or diffuse edema, which is occasionally accompanied by bleeding or notable lesions. Patients usually visit hospitals because of persistent abdominal pain or intermittent abdominal pain, with increased white blood cells and eosinophilia cells. The people, in these 87 cases, had a history of ingestion of infective seafood.
We discovered found out this case of Anisakis infection by chance, which suggests that people lack awareness of Anisakis infection in China and also lack the clinical diagnosis methods for Anisakis infection. Considering that China has 1.3 billion people and approximately 14,500 km of mainland coastline, there should also be some potential human cases of Anisakis infection in China, where raw seafood are usually used as edible food. Our finding shows that Anisakis infection is present in China, and awareness of Anisakis infection should be helpful in clinical diagnosis.
Footnotes
Acknowledgment
This work was supported by National Natural Science Foundation of China (No. 81201563).
Disclosure Statement
No competing financial interests exist.