
Abstract
Salmonella enterica serovar Weltevreden and Vibrio fluvialis were identified as etiological agents of a foodborne gastroenteritis outbreak after an Iftar feast in North Dumdum. Of the 278 cases admitted to the Infectious Diseases Hospital, Kolkata, 44 stool samples were tested for the enteric pathogens. Six were positive for Salmonella Weltevreden, 5 for Vibrio fluvialis, and 8 contained both of the pathogens. Consumption of mutton-ghogni might have been the likely vehicle of this outbreak. In the pulsed-field gel electrophoresis, Salmonella Weltevreden was identified as a single clone but the V. fluvialis strains were heterogeneous.
Introduction
F
Materials and Methods
Stool specimens were screened for enteric pathogens using standardized protocols (Panchalingam et al., 2012). Serotyping of Salmonella was done using commercial antisera (S&A Reagents Lab, Bangkok, Thailand). Three lactose-fermenting colonies confirmed as Escherichia coli by biochemical testing were tested in a multiplex polymerase chain reaction assay for the detection of three pathogroups (i.e., enterotoxigenic, enteropathogenic, and enteroaggregative E. coli) (Panchalingam et al., 2012). Polymerase chain reaction was also performed to detect the V. fluvialis spp. and virulence genes of V. cholerae following the methods described previously (Chakraborty et al., 2006; Chatterjee et al., 2009).
Antimicrobial susceptibility testing was performed using the disk-diffusion method with commercially available disks of ampicillin (10 μg), trimethoprim–sulfamethoxazole (25 μg), ciprofloxacin (5 μg), norfloxacin (10 μg), ofloxacin (5 μg), chloramphenicol (30 μg), nalidixic acid (30 μg), streptomycin (10 μg), tetracycline (30 μg), and erythromycin (15 μg) (Becton Dickinson, Sparks Glencoe, MD) in accordance with the criteria recommended by Clinical and Laboratory Standards Institute (CLSI, 2011). E. coli ATCC 25922 and Staphylococcus aureus ATCC 25923 were used as quality-control strains.
Pulsed-field gel electrophoresis was performed according to the PulseNet protocol (
National Institute of Cholera and Enteric Diseases Ethics Committee has approved this study (Ref.C-48/2012-T&E), and each participant/parent in the case of children gave written informed consent.
Results and Discussion
On July 30, 2012, 474 people attended an Iftar ceremony during the Ramzan month at Bankra, Birati, North Dumdum, West Bengal. More than 300 people developed symptoms of food poisoning including watery diarrhea, abdominal pain, vomiting, and fever after consumption of mutton-ghogni (composed of minced meat from cooked lamb with beans) along with other foods prepared by a caterer. Two hundred seventy-eight patients were referred and admitted in the Infectious Diseases Hospital (IDH), Kolkata due to severity diarrhea and dehydration (27 on July 30, 237 on July 31, and 14 on August 1). The age of the patients varied from 6 to 55 years, and adult male patients (male:female >6:1) were more infected than children (n=26). After the consumption of food in the evening, diarrheal symptoms appeared between 8 and 10 h later in the majority of the cases. Most of the patients recovered within 48 h after treatment at the IDH, but two patients aged 6 and 11 years died, probably due to encephalopathy coupled with acute diarrhea. Depending on the nature of dehydration, the patients were administered either intravenous fluid or oral rehydration solution, and ciprofloxacin and metronidazole were given in divided doses.
The source of infection was presumed to be mutton-ghogni that was consumed uniformly by all the patients. We could not obtain any served food items to identify the causative pathogen of this outbreak. Information on the mode of cooking revealed that the foods were prepared outdoors.
Microbiological analysis of 44 samples revealed that 6 (13.6%) were positive for Salmonella Weltevreden, 5 (11.4%) for V. fluvialis, and 8 (18.2%) with both of the pathogens. In addition, two samples each were positive for V. cholerae non-O1, non-O139 and enteropathogenic E. coli, and one was positive for heat-labile toxin-producing (LT)–enterotoxigenic E. coli. Concomitant infections during outbreaks have been rarely reported in the past (Chakraborty et al., 2001). To our knowledge, this is the first foodborne outbreak comprising both Salmonella Welteverdan and V. fluvialis in India. Salmonella Weltevreden is gaining global importance as a significant pathogen causing nontyphoidal salmonellosis. This serovar has been most frequently isolated from humans in India, Thailand, and Korea (Bangtrakulnonth et al., 2004; Antony et al., 2009; Kim et al., 2010). Recently, the prevalence status and clinical importance of V. fluvialis has been reported in Kolkata (Chowdhury et al., 2012).
Antimicrobial susceptibility testing of Salmonella Weltevreden showed that most of the strains were susceptible for all the antibiotics except for erythromycin. Most of the V. fluvialis strains were resistant to trimethoprim-sulfamethoxazole and erythromycin. The V. fluvialis strains did not harbor any virulence genes or the encoding regions of virulence-associated genes of other vibrios. Of the 10 V. fluvialis strains, eight were clonally related with overall pulsed-field gel electrophoresis similarity of more than 90%: two in cluster A and six in cluster B (Fig. 1A). These strains were different from a V. fluvialis strain isolated in 2008 in this region (cluster A). One V. fluvialis strain isolated during 2008 from a diarrheal patient had close lineage with strain IDH453 (96%), IDH4535, and IDH4536 (92%) in cluster A (Fig. 1A). All the Salmonella Weltevreden exhibited an identical XbaI profile and hence belong to the single clone (Fig. 1B). However, they varied from profiles of patient's strains isolated during 2010 and 2011 in Kolkata.
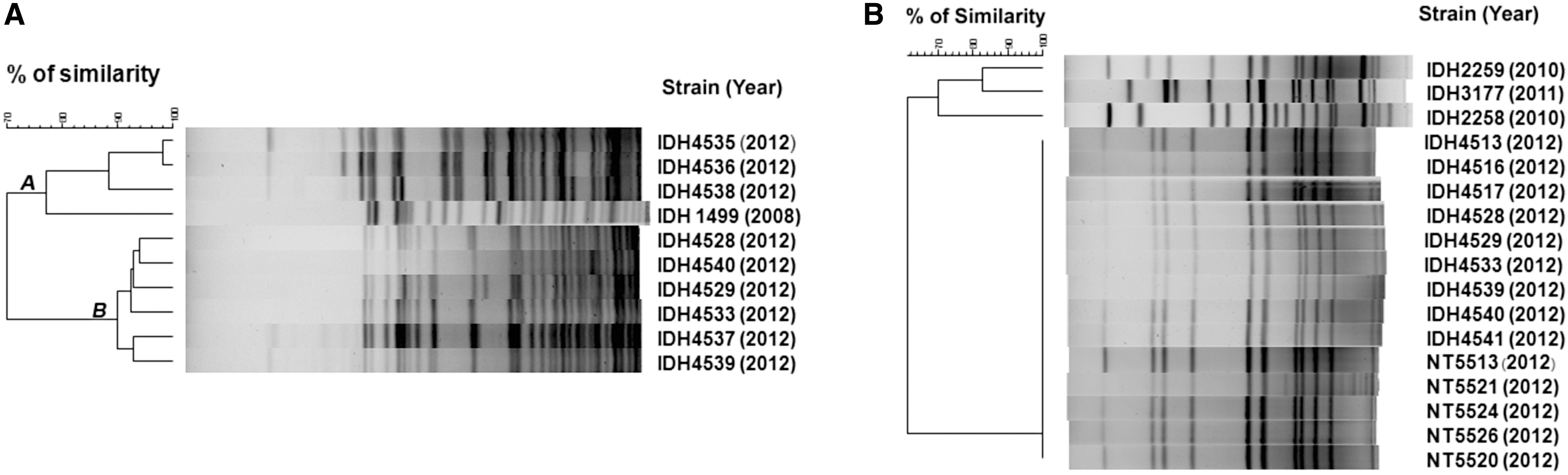
NotI-digested chromosomal DNA banding patterns of Vibrio fluvialis strains placed in two clusters A and B
The existing surveillance system has helped in the timely identification of causative pathogens in this outbreak. However, proper planning should be in place for the identification of the source of contamination and have the capability for performing case–control studies in the future outbreaks/epidemics.
Footnotes
Acknowledgment
This work was supported in part by the Indian Council of Medical Research, New Delhi, India and by the Japan Initiative for Global Research Network on Infectious Diseases, Ministry of Education, Culture, Sports, Science and Technology, Japan. AS was awarded Junior Research Fellowship by the National Academy of Sciences, Allahabad, India. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure Statement
No competing financial interests exist.