
Abstract
Shiga toxin–producing Escherichia coli O157:H7 (STEC O157) is the most commonly identified serotype of STEC in the United States. An estimated 63,000 STEC O157 infections occur annually. Infection typically results in diarrhea, bloody stool, abdominal cramps, and, in some cases, hemolytic uremic syndrome. Recent outbreaks of STEC O157 have increasingly been associated with consumption of leafy greens such as lettuce and spinach. We investigated an outbreak of STEC O157 associated with the consumption of bagged salad with cases clustered in various institutional settings. A case–control study was conducted among cases from selected schools with controls matched by school and grade. Seventeen cases from three U.S. states were identified. The median age of cases was 23 years (range: 3–88) and 13 (76%) were female. Six cases were hospitalized and two died. Onset dates ranged from April 29 to May 12, 2012. The matched case–control analysis identified a single significant food service exposure: consumption of lettuce provided by a school cafeteria (median odds ratio=9.4, 95% confidence interval: 1.4–∞, p=0.0469). The implicated bagged salad product was traced back to a single production facility. Implicated growing areas were scheduled for heightened inspection for the upcoming growing season. A combination of analytical epidemiologic studies among subclusters of cases, surveillance, and traceback implicated bagged salad in this outbreak investigation.
Introduction
STEC O157
In recent years, STEC O157 outbreaks have been increasingly linked to fresh leafy green products such as lettuce and spinach (Rangel et al., 2005; Gould et al., 2013).
Previous enteric disease outbreak investigations have benefitted from epidemiologic and traceback investigations of subclusters (Behravesh et al., 2011; Cavallaro et al., 2011). This report describes an investigation of a STEC O157 outbreak, including an analytic epidemiologic study among subclusters cases and product traceback, which implicated bagged salad as the vehicle.
Materials and Methods
The Tennessee Department of Health (TDH) conducts active surveillance for laboratory-confirmed cases of STEC O157 infection as part of the Centers for Disease Control and Prevention's (CDC) Foodborne Diseases Active Surveillance Network. STEC O157 isolates are submitted to the public health laboratory and undergo molecular subtyping by two-enzyme pulsed-field gel electrophoresis (PFGE). Further characterization by multiple-locus variable-number tandem repeat analysis (MLVA) is performed at CDC when additional subtyping discrimination is necessary to advance an investigation. Persons with laboratory-confirmed infections are interviewed using a standard case-report form to collect demographic and illness information, as well as information about risk factors and potential links to other cases.
In this investigation, a confirmed case was defined as an individual with isolation of STEC O157 PFGE pattern “A,” with matching MLVA type, and illness onset (or specimen collection date, if onset date was unknown) since April 15, 2012. A probable case was defined as an individual with diarrhea lasting ≥2 days since April 15, 2012, who was epidemiologically linked to a confirmed case.
A matched case–control study was conducted. Seven confirmed and probable cases from four Tennessee schools (Schools A, B, C, and D) were enrolled in the case–control study. Three or four controls were matched on school and grade to each case. The case–control questionnaire included 43 exposures common among ≥25% of cases from initial standardized interviews. Matched odds ratios were calculated by conditional logistic regression.
Menus and invoices were requested from the involved food service facilities. Traceback investigations were conducted by TDH and the U.S. Food and Drug Administration (FDA).
Results
On May 3, 2012, TDH identified a cluster of five STEC O157 cases from two day care facilities with shared management. By May 17, 2012, we had identified a cluster of 14 STEC O157 isolates with indistinguishable PFGE patterns. Upon review of the national data, there were 17 matching isolates from 3 states: Tennessee, Georgia, and Ohio. MLVA testing was requested to further characterize the outbreak strain. Testing determined the Tennessee, Georgia, and Ohio cases were also indistinguishable by MLVA. One sputum isolate from a Tennessee case was processed in the same hood at the same time as a stool specimen from another case. This was determined to be a contamination event; therefore, the sputum isolate was excluded from the outbreak. Among the 16 outbreak cases with indistinguishable PFGE and MLVA patterns, 13 were Tennessee residents, 2 were Georgia residents, and 1 was an Ohio resident. Additionally, one probable case was identified in Tennessee. Illness onset dates ranged from April 29 to May 12, 2012 (Fig. 1). Median age among cases was 23 years (range: 3–88 years) and the majority (13, 76%) were female. Six cases were hospitalized and there were 2 deaths (age range: 77–88).
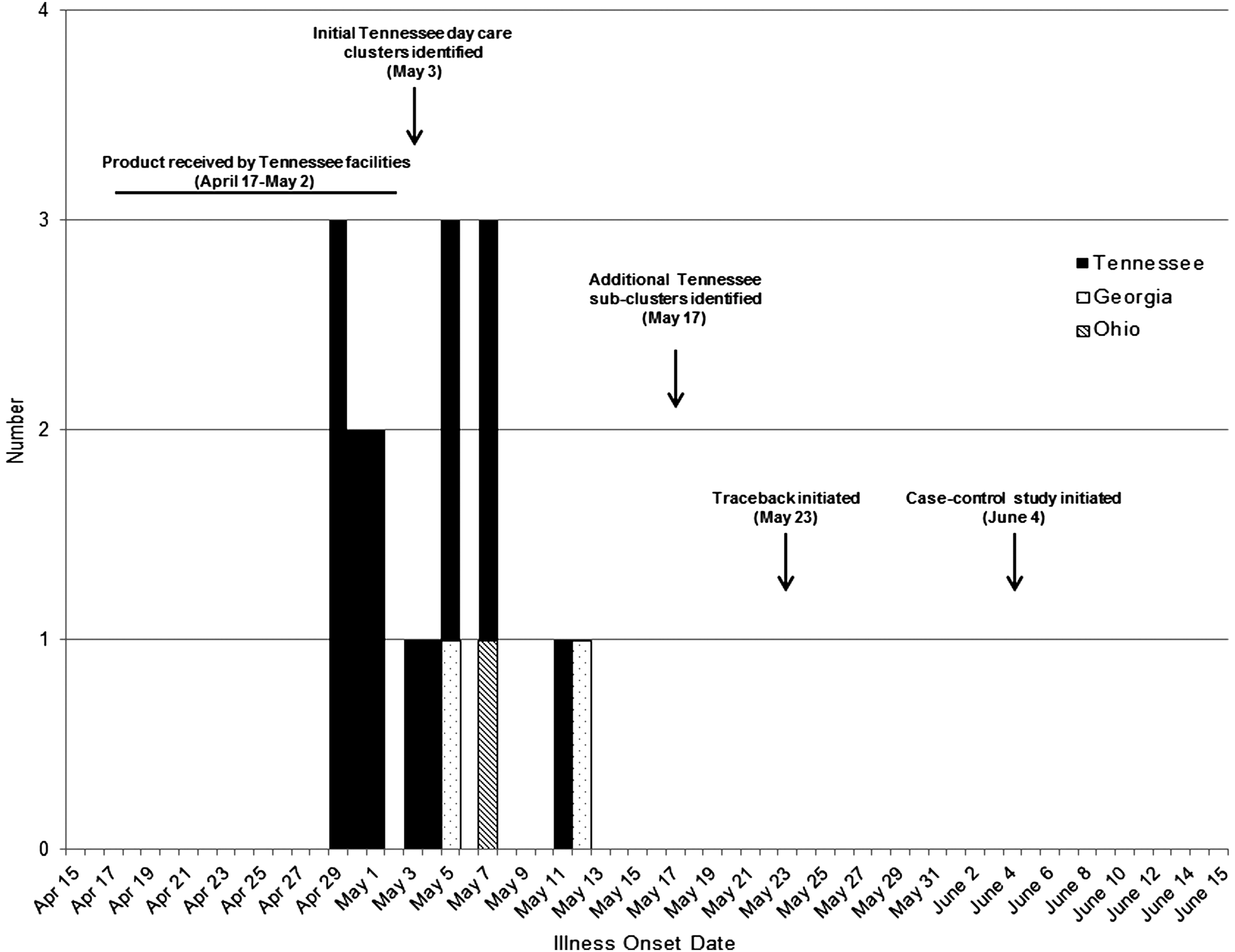
Shiga toxin–producing Escherichia coli O157:H7 outbreak-associated infections by illness onset date, April 15–June 15, 2012, United States.
Among the Tennessee cases, four institutional subclusters were identified. Four cases attended School A, 2 cases attended Schools B and C, whose food service was provided by the same caterer, 3 cases attended Daycare 1, and 2 cases attended Daycare 2. All three cases in Ohio and Georgia were reported to reside in long-term care facilities and consume food in that institutional setting.
The matched case–control study conducted among 7 cases from 4 Tennessee subclusters and 22 controls identified a single significant exposure within these school settings. Four of 7 cases included in the case–control study and 4 of 22 controls reported consumption of lettuce provided by the school cafeteria (median odds ratio=9.4, 95% confidence interval: 1.4–∞, p=0.0469). Traceback identified a bagged salad product in common among the Tennessee institutions. Subsequent FDA traceback also identified a specific bagged salad product from a single producer. This bagged salad product contained romaine, iceberg lettuce, cabbage, and carrots. Additionally, the surviving Georgia case consumed food at facilities that received the implicated bagged salad product. Food histories were not available for cases that died; however, both cases resided in long-term care facilities that received the implicated product. Based on institutions' invoice dates, data obtained from the producer indicated that a single day of production could account for the outbreak. The source of contamination is unknown; however, FDA identified specific growing areas for follow-up inspections during the next harvest season.
Discussion
We investigated an outbreak of STEC O157 associated with consumption of bagged salad served in institutional settings. Multiple lines of evidence implicated the product including descriptive epidemiology, matched case–control analysis, and traceback. Early in the investigation, a produce vehicle, specifically lettuce, was suspected based on temporal and demographic characteristics of the cases. Our descriptive epidemiologic findings indicated that 76% of cases were female, a demographic previously shown to be consistent with consumption of produce in other outbreak investigations (Ackers et al., 1998). Temporally, cases were largely clustered over a 9-day timeframe consistent with a produce food vehicle with a short shelf life. The matched case–control analyses identified a single exposure with a significant matched odds ratio. We enrolled 7 cases from 4 schools using 22 school- and grade-matched controls to assess the risk of foods in common across the institutional subclusters. The bagged salad product was identified in food service records. Although the traceback was complex and resource intensive, it confirmed the source of infection. Because the outbreak was over and no ongoing risk was identified, no recall of the implicated product occurred. FDA reported that field staff would schedule heightened inspections of the suspected produce-growing areas identified during this investigation.
This brief report highlights two important methods in foodborne disease outbreak investigations: subcluster investigations and traceback. In previous foodborne disease outbreak investigations, subcluster investigations, including restaurant, event, and institutional setting clusters, have been important in identifying transmission vehicles (Behravesh et al., 2011; Cavallaro et al., 2011). Additionally, investigation of outlier and unusual cases such as the matching O157 isolate from a sputum specimen can aid in epidemiologic investigations. Utilizing multiple epidemiologic approaches can be important to fully investigate a foodborne outbreak, especially when multiple geographic areas are involved. Thorough investigation of small outbreaks can identify potential problems in production areas facilitating risk assessment and risk mitigation.
Footnotes
Acknowledgments
The authors would like to thank Ellen Salehi from the Ohio Department of Health, Hope Dishman from the Georgia Department of Health, and the Tennessee Department of Health FoodCORE staff for their assistance in this investigation. This report was supported in part by an appointment to the Applied Epidemiology Fellowship Program administered by the Council of State and Territorial Epidemiologists (CSTE) and funded by the Centers for Disease Control and Prevention (CDC) Cooperative Agreement Number 5U38HM000414-5.
Disclosure Statement
No competing financial interests exist.