
Abstract
There are an estimated 4.7 million cases of foodborne illness in Australia each year, but the contaminated food items that are the source of these illnesses are rarely identified. Current knowledge relies largely on the few foodborne outbreaks where the implicated food commodity was identified. To better understand which foods cause outbreaks, we analyzed 18 years of foodborne outbreak data collected in New South Wales (NSW) and classified the food dishes responsible for the outbreaks into standardized categories based on type of dish and preparation method. A total of 869 outbreaks were reported in NSW from 2000 to 2017. Outbreaks with a suspected contaminated food or dish reported (57.1%) underwent dish reclassification that assigned the implicated food into two groupings that characterized the food consumed into commonly understood dish types (e.g., sandwich, stew, etc.) and how it was prepared (e.g., sliced, heated, etc.). The dish type associated with the most outbreaks was sandwiches (18.8%) followed by desserts (13.1%) and then stir fries (9.1%). The dishes associated with more serious outbreak outcomes (higher numbers of cases, hospitalizations, and deaths per outbreak) were those associated with ready to eat fresh produce. Dish preparations that did not involve a cooking step also resulted in more serious outcomes. While identifying contaminated food is crucial for food safety reasons, people rarely consider these risks when eating. Food carries the combined risks posed by the ingredients and preparation method followed. Education of food business operators and consumers needs to promote a view of food safety risk that goes beyond unsafe commodities, encouraging a holistic perspective that considers ingredients and preparation methods.
Introduction
There are an estimated 4.7 million episodes of gastroenteritis per year in Australia which are attributed to contaminated food (Glass et al., 2023). The diversity of people’s diets makes identifying pathogen-transmitting foods challenging. Epidemiological investigation of foodborne outbreaks provides the best opportunity to determine the contaminated food by comparing what affected and unaffected individuals consumed.
The New South Wales (NSW) Health Department has collected summary data on each foodborne disease outbreak and entered it into a surveillance database since 2000. Previously, we reported that eggs were the most common food associated with outbreaks (12.4% of outbreaks) followed by fish (3.3%), chicken meat (2.5%), and mollusks (1.1%). However, 77.2% of foodborne outbreaks in NSW had no food source identified (Franklin et al., 2020). It is critical to understand this missing knowledge, as food safety agencies rely on the identification of contaminated food to stop current and prevent future outbreaks.
The analysis of historical foodborne outbreak data is limited to outbreaks where contaminated food commodities have been identified (Belanger et al., 2015; Gormley et al., 2011; Gould et al., 2013; Painter et al., 2013). While this approach is practical for targeting contamination at the primary production level and preventing the spread of the pathogen through the food supply chain, it overlooks the complexity of transmission of foodborne illness and the nature of contamination further down the supply chain.
Effective food safety relies on interventions across the entire supply chain (NSW Food Authority, 2015), including at the level of food retailers and consumers. Therefore, understanding not only the implicated commodities but also the specific dishes and food processing methods that contribute to outbreaks allows the development of targeted interventions and improved food safety practices.
The aims of this article were to better understand the causes of foodborne outbreaks by characterizing and categorizing the food sources of outbreaks in NSW. We reclassified the implicated foods into categories based on common dishes and food processing methods to identify the most frequent vehicles of outbreaks and those associated with the most severe outcomes, aiming to highlight potential food safety interventions.
Methods
Summary information on all foodborne outbreaks notified to NSW Health since 2000 was captured in a database. Medical professionals, laboratories, food safety regulators, and the public notify the NSW Health Department on cases of potential foodborne illness outbreaks. NSW Health Department also investigates potential outbreaks through analysis of routine surveillance data. Summary data collected on each outbreak include the outbreak setting, outbreak extent, mode of transmission, causative organism, results of epidemiological and environmental investigations, and the suspected causes of the outbreak. Data fields were not mandatory for reporting, so missing data is common for some variables. For this analysis, we analyzed data on all suspected foodborne outbreaks between 2000 and 2017. The case definition for suspected foodborne outbreaks was an incident where two or more persons experience a similar illness after consuming a common food or meal and evidence (analytical, epidemiological, or microbiological) implicated the meal as the source of the illness.
We described the etiology of outbreaks in a companion article (Franklin et al., 2020). Briefly, if the pathogen cause was not detected in the outbreak, we classified outbreaks into the three major types of foodborne pathogen outbreaks; bacterial toxin outbreaks (hereafter ‘Toxin outbreak’), bacterial pathogen outbreaks (‘Bacterial outbreak’), and viral-gastroenteritis pathogen outbreaks (‘Viral outbreak’) based on matching the symptom characteristics and epidemiology of those types of outbreak.
In this article, we reclassified the ‘food vehicle’ field for each outbreak using a standardized approach. Each food item was examined to determine its typical form as consumed, based on preparation method and dish format. For example, a ‘hamburger’ is assembled from uncooked and cooked components, into what is universally understood to be a sandwich (a dish of fillings served within bread). The food vehicles were assigned the dish category that corresponded to the final dish preparation method; for instance, lasagna contains a stewed sauce but is finished in the oven so was categorized as a baked dish. To ensure consistency, publicly available recipes, and restaurant menu descriptions were consulted using structured web searches. Categories and definitions were created inductively during the review process, aiming to reflect common food handling practices and known food safety risks. To minimize subjectivity, all dish and preparation method classifications were independently reviewed and verified by a second epidemiologist who was not involved in the original data coding.
Using the methodology described above and the ‘food vehicle’ field in outbreak reports, we created two parallel categorical variables to characterize the food consumed in an outbreak; the first one being the dish type (18 categories, Table 1) and the second variable preparation method (7 categories, Table 2), based on the heating and physical assembly that transforms the component foods into the dish consumed. For example, a salad made solely from raw ingredients was classified as cold preparation, while one with freshly cooked meat was categorized as semi-cooked. A simple roast chicken was considered baked, whereas a full roast meal with cooked vegetables was classified as hot preparation due to the final assembly of heated components.
Dish Type Categorization
Dish Preparation Process for Meals Attributed to Outbreaks
Outbreaks due to ciguatera and scombroid poisoning from fish were excluded from dish type analysis, as the toxin is present before food preparation. If an outbreak-linked meal contained multiple dish types and lacked a clear source, it was classified as ‘multiple’ dishes. Outbreaks that did not have a food vehicle identified remained classified as unknown. Multiple dishes and unknown outbreaks were not analyzed further.
We analyzed data using Stata 13.1 (StataCorp, 2013). The change in relative proportions over time was assessed using a Chi-squared test for trend. Comparisons of associations between outbreak characteristics (dish type and processing type) and outbreak severity measures were made using one-way ANOVA with Bonferroni post-test. The outbreak severity point estimation was calculated using combined Z-scores for the average number of people ill, hospitalized and who died during outbreaks for each dish type.
AI-assisted tools (ChatGPT, version GPT-4o, accessed on 17 February 2025) were used only for language refinement and readability improvements in article preparation. No AI-generated content, data analysis, or figure creation was included in this study. The authors manually reviewed all edits to ensure accuracy and integrity.
Results
There was a total of 869 foodborne outbreaks investigated in NSW between 2000 and 2017, affecting a total of 11,902 people. A full description of the pathogen breakdown can be found in the companion article (Franklin et al., 2020) but in short, bacterial outbreaks were the most common (315/869, 36.3%) primarily due to Salmonella contamination (267/869, 30.7%), followed by viral outbreaks (237/869, 27.3%) and toxin outbreaks (228/869, 26.2%). Over the 18-year period, we did not observe any significant trend in the types of dishes or preparation processes associated with foodborne outbreaks. Outbreak frequency by dish type fluctuated yearly without a clear pattern.
Dish types
A suspected contaminated food or dish was reported in 57.1% (496/869) of outbreaks with 94.4% (468/496) undergoing dish reclassification. From those outbreaks where we classified the type of dish, most outbreaks were associated with sandwiches (19.7%, 92/468) followed by desserts (13.9%, 65/468) and then sauces and dips (10.5%, 49/468) (Fig. 1A, B). Bacterial outbreaks were most commonly associated with dessert dishes (24.3%, 50/206) followed by sandwiches (20.9%, 43/206). Sandwiches were the dish most commonly associated with viral outbreaks (29.4%, 30/102) followed by salads (21.6%, 22/102). Toxin outbreaks were most commonly associated with stews (21.6%, 29/134) followed by stir fries (19.4%, 26/134).
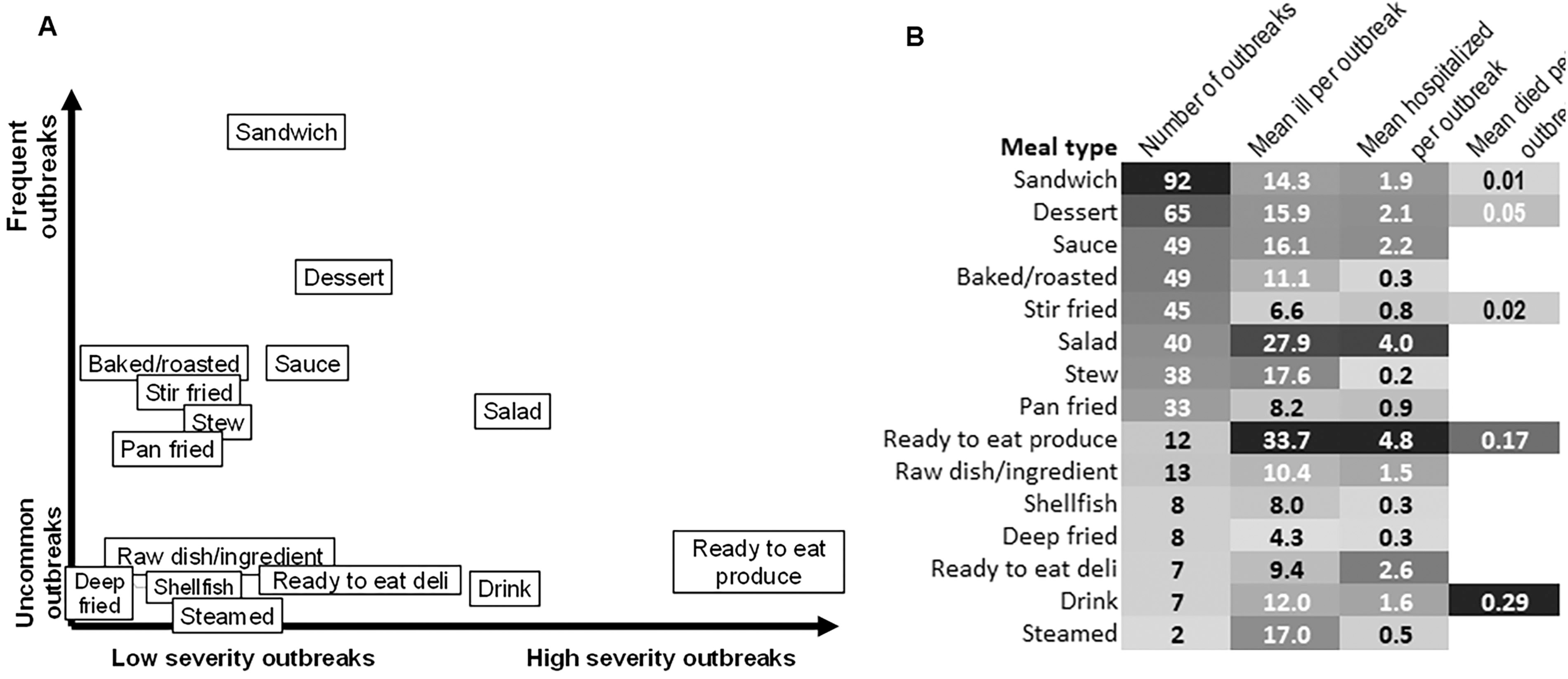
Outbreaks due to ready to eat fresh produce accounted for 1.4% (12/869) of the outbreaks but were the dishes associated with the highest mean number of people affected and hospitalized (Per outbreak: 33.7 persons ill, 4.8 hospitalized and 0.2 deaths) (Fig. 1B). The dishes associated with the smallest outbreaks and fewer severe outcomes were deep fried dishes (4.3 people ill and 0.3 hospitalizations per outbreak) and pan-fried dishes (8.1 people ill and 0.9 hospitalizations per outbreak). These differences did not reach statistical significance. (Fig. 1A, B).
Commercial kitchens were the most common preparation location for dishes causing foodborne outbreaks (78.0%, 678/869), accounting for 100% of the outbreaks due to deep-fried and steamed dishes, 97.8% (44/45) of the stir-fry outbreaks and 94.6% (87/93) of the sandwich outbreaks. Private kitchens were the second most common setting accounting for 8.9% (77/869) of outbreaks, with dish types identified in 54.5% (42/77) of cases. The most common dish type from a private kitchen was desserts (23.8%, 10/42) followed by pan-fried dishes (16.7%, 7/42).
Types of dishes causing outbreaks
The dish preparation method was available for 63.3% (550/869) of outbreaks. From those, dishes involving cold preparation were the most common (34.2%, 188/550) followed by hot preparation dishes (31.6%, 174/550) and semi-cooked preparation dishes (24.5%, 131/550) (Fig. 2A, B). Broken down by pathogen type, cold dishes were most frequently associated with bacterial outbreaks (45.4%, 109/240) and viral outbreaks (45.3%, 58/128), and hot dishes were the most common in toxin outbreaks (61.4%, 94/153). The majority (77.8%, 428/550) of dishes causing outbreaks involved the physical assembly of the dish just prior to serving (either post-cooking or using cold or uncooked ingredients).
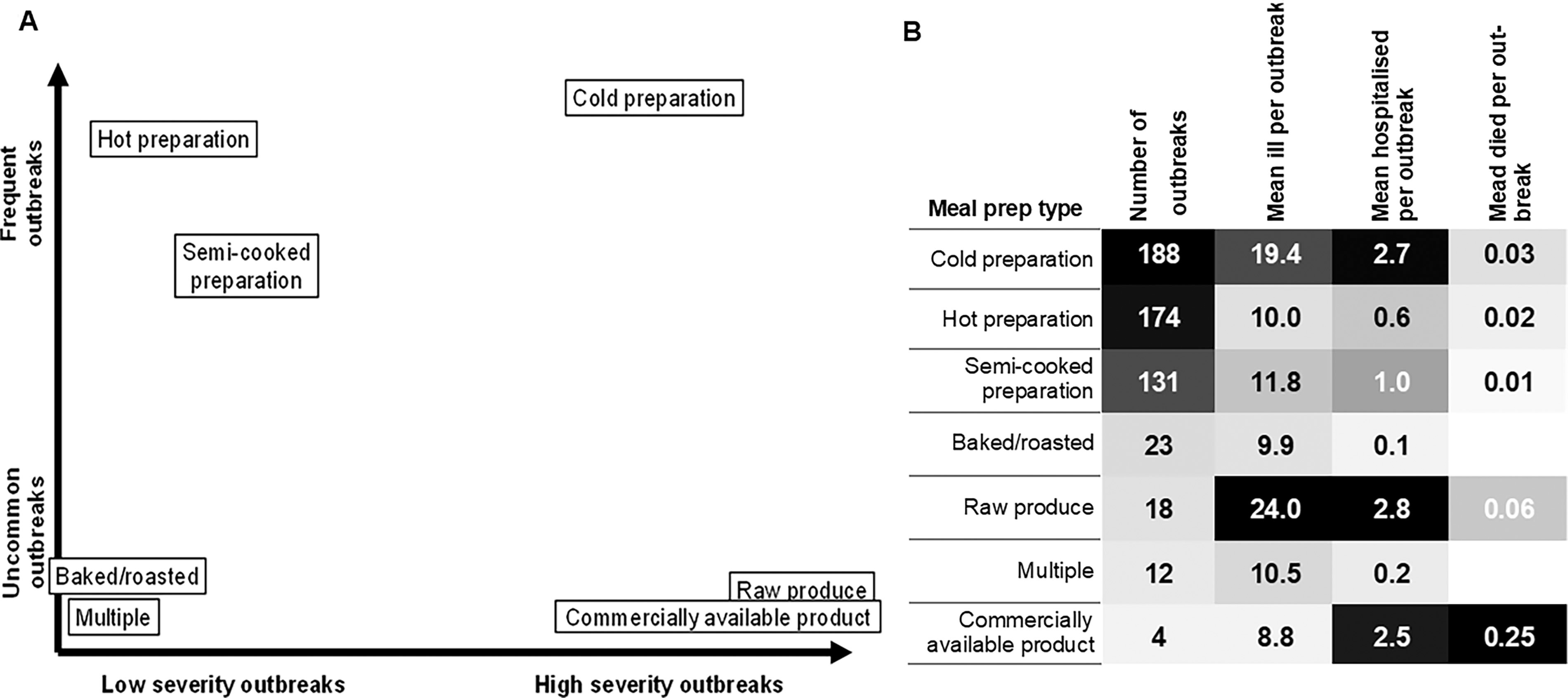
The dish preparation type associated with the most severe outcomes was raw produce (24.0 ill, 2.8 hospitalizations, and 0.06 deaths per outbreak) followed by cold preparation (19.4 ill, 2.7 hospitalizations, and 0.03 deaths per outbreak) and commercially available products (8.8 ill, 2.5 hospitalizations and 0.25 deaths per outbreak). The items associated with the least serious outcomes were those that were baked (9.9 ill and 0.1 hospitalized per outbreak) and hot preparation (10.1 ill, 0.6 hospitalized, and 0.02 deaths). Outbreaks involving cold preparation dishes were significantly larger (19.4 vs. 10.1 ill per outbreak, p = 0.015) and had significantly more hospitalizations (2.7 vs. 0.6, p = 0.004) than outbreaks involving hot preparation dishes (Fig. 2A, B).
In outbreaks associated with commercial kitchens, hot preparation was the most common method used to prepare dishes (32.7%, 146/446) followed closely by cold preparation (32.1%, 143/446). In private kitchens, cold preparation was the most common method associated with outbreaks (50.0%, 22/44), followed by hot preparation (20.5%, 9/44). In institutional kitchens, such as aged care facilities, hot preparation of food was the most common method seen in outbreaks (11/24, 44.0%).
Discussion
This study reexamined foodborne outbreak causes in NSW, revealing that sandwiches and desserts are the most common vehicles of outbreaks, with uncooked dishes leading to the most severe outcomes. Traditional food safety strategies often focus on food ingredients, overlooking the risks posed by the prepared dishes. Broadening food safety considerations to include a wider range of risk factors can help both food business operators (FBOs) and consumers adopt more effective preventive measures.
By classifying outbreak foods into specific dish types, we improved the data on food-related outbreaks in NSW from 22.8% (outbreaks that had a food commodity identified) to 57.1% of all outbreaks. A breakdown by preparation method showed that most outbreaks (77.8%) involved dishes that required manual handling before serving. Dishes and ingredients aren’t inherently risky, but rather, a dish is a sum of all risk factors during production. Representing a dish as both the type of food and the preparation process exposes the outbreak risk potential of the dish. The risk of pathogen persistence through the food chain is well known, such as in the case of Listeria monocytogenes, where the concept underpins all control recommendations and regulations(NSW Food Authority, 2019; Tompkin, 2002). Applying this idea of enduring risk to food dishes could enhance food safety behaviors that go beyond single ingredient-focused approaches.
In Australia, sandwiches have caused large outbreaks, often due to Salmonella-contaminated raw egg mayonnaise (Ford et al., 2018). We found sandwiches to be a potential risk for foodborne illness beyond the use of raw eggs, but also because of the high-risk processing steps involved in the assembly. The preparation of a sandwich involves many physical handling steps, each step increases contamination risks from the food handlers, kitchen implements, and preparation surfaces, often without a final cooking kill step being followed. This also applies to salads, which were the second most common dish associated with viral outbreaks. Desserts were most frequently linked to bacterial outbreaks, and similarly to sandwiches are known to be vehicles for contaminated raw or undercooked eggs (Moffatt et al., 2016). Desserts should also be considered a sum of the risks present in the bakery or kitchen that processed them, especially if assembled from cold or raw ingredients.
We found no significant trends in the types of dishes implicated in outbreaks over the study period. However, certain dishes were a more common cause of outbreaks in specific years, suggesting variability in risk factors over time. Long-term trends are unlikely when food habits change so often. Collaboration between public health and food safety regulators is essential to address emerging food risks. This was seen in 2015 when the NSW food regulators introduced a foodborne illness reduction strategy (NSW Food Authority, 2015) that responded directly to public health reports that eggs were the single largest cause of foodborne outbreaks in the state (NSW Ministry of Health, 2013; NSW Ministry of Health, 2014). For this issue, they introduced research with egg industry groups, microbial monitoring, training for food retailers as well as improvements in egg traceability. By 2021, the strategy had met its goal of reducing the rate of Salmonellosis by 32% in NSW (McLure et al., 2022). This strong working relationship and data sharing between public health and food regulators is essential to meet the ever-changing threat of food contamination.
A limitation of this analysis is that it only accounts for foodborne outbreaks that were reported to public health. Many outbreaks go unreported(Ford et al., 2023). Moreover, most foodborne illnesses are from single cases of disease, which would likely have different associated risks. Although we have no way to know what dishes cause these sporadic illnesses, equipping the public with the tools to prepare food safely themselves could help reduce these instances. People often link foodborne illness to specific items, like undercooked chicken. However, when preparing a chicken dish, the true risk lies in potential cross-contamination of the final dish or another dish, from surfaces coming in contact with raw chicken. Viewing meals as a sum of risks rather than a single ingredient would help the public recognize and prevent hazards.
The classification scheme we developed for this analysis was built from food items mentioned in outbreaks in the study period and used descriptions of dishes commonly recognized in English-speaking countries. This may have introduced overfitting and limited the scheme’s generalizability to other populations. As it is a new scheme there is also potential for subjectivity in the classification used, despite the review by an additional epidemiologist. In addition, being a completely new scheme means there are no previous studies to compare the findings to. Large summaries of foodborne outbreak data from other countries (Belanger et al., 2015; Gormley et al., 2011; Gould et al., 2013) report similar levels of outbreaks with implicated foods (57.6–75.6%) but report the food causes of outbreaks at the commodity level only.
Another potential limitation of the categorization scheme is its assumption that each category represents a uniform risk profile. This could be problematic, as a category like ‘sandwich’ for example, includes a wide range of food products prepared in diverse ways, each carrying distinct food safety and pathogen risks. We dealt with this problem by including a parallel classification scheme of ‘dish processing type’ to go with ‘dish type’. How a food is processed is integral to the risk posed by the food. By introducing a sub-classification based on processing type, we delineated the different food safety risks within each dish type. The more common classification scheme used in foodborne outbreak analysis is a hierarchical commodity scheme, which aims to attribute outbreaks to a single food commodity (Painter et al., 2009). Advocates of this scheme argue that it can be utilized in modeling to guide policymakers and health agencies on where to focus their efforts in preventing foodborne illnesses. However, limiting focus to the top of the food processing chain ignores the potential for effective food safety measures at the bottom of the chain, where meals are prepared. This approach disconnects food safety risks from the food that people eat, and it reduces the importance of implementing safety measures during meal preparation.
We found that the dish type with the most serious outcomes was ready to eat fresh produce. These outbreaks were typically large and geographically distributed, and cases did not have a dish recorded because the focus was on identifying the common commodity. In these types of outbreaks, developing a hypothesis by asking about the consumption of a very large list of commodities remains important. Having a dish-based level of questioning may also help in these types of investigations by allowing investigators to focus on commodities most likely to be associated with dishes that appear to be commonly consumed, for example focusing on fresh vegetables when salads are being commonly consumed. The other dish types associated with the most serious outcomes were those without a cooking step. This is not surprising since sufficient cooking kills enteric pathogens; however, it highlights that there needs to be greater emphasis and understanding that dishes involving uncooked foods can have a higher risk of foodborne illness.
Conclusion
Foods typically listed as a concern for foodborne illness include red meats, poultry, eggs, and seafood (NSW Department of Primary Industries, n.d.), with little focus on the prepared dish. While these items are risks for foodborne illness when foods are improperly cooked, we found that sandwiches and desserts are in fact the most common vehicles of foodborne outbreaks in NSW and that uncooked dishes of all kinds result in the most serious outcomes. FBOs and consumers need education about food safety risks involving a variety of food commodities. Helping people understand why a particular dish could be a vehicle for foodborne illness would be a valuable way to empower people to prevent illness.
Footnotes
Acknowledgments
The authors thank the OzFoodNet Network, which is funded by the Australian Government Department of Health. The authors also thank the NSW public health network which investigated these outbreaks, in conjunction with the NSW Department of Primary Industries.
Data Sharing Statement
The data used in this study was obtained under the provisions of the NSW Public Health Act 2010. Due to privacy, confidentiality, and legislative restrictions, these data cannot be shared publicly.
Ethics Statement
This study did not require ethical approval as it was conducted using routinely collected notifiable disease surveillance data under the provisions of the NSW Public Health Act 2010. The analysis was performed as part of public health practice, and no identifiable individual data were used. In accordance with NSW Health policies, ethics approval was not required for this study.
Authors’ Contributions
N.F.: Conceptualization, methodology, software, formal analysis, data curation, writing—original draft, writing—reviewing and editing, visualization. K.G.: Writing—reviewing and editing, supervision. M.K.: Writing—reviewing and editing, supervision. K.H.: Writing—reviewing and editing, supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.