
Abstract
Abstract
Objective:
To compare the effectiveness of Kinect Adventures games versus conventional physiotherapy to improve postural control (PC), gait, cardiorespiratory fitness, and cognition of the elderly. In addition, we evaluated the safety, acceptability, and adherence to the interventions.
Materials and Methods:
The study was a randomized clinical trial in which 46 elderly individuals were selected, mean age 69.3 (5.34) years. Participants were allocated to the Kinect Adventures Training Group (KATG) or the Conventional Physical Therapy Group (CPTG), 23 individuals in each group. Participants of both groups participated in 14 training sessions lasting 1 hour each, twice a week. The KATG practiced four Kinect Adventures games. The CPTG participated in conventional physiotherapy. The primary outcome was PC: Mini-Balance Evaluation Systems Test (Mini-BESTest), and secondary outcomes were gait: Functional Gait Assessment (FGA), cardiorespiratory fitness: Six-minute step test (6MST), and cognition: Montreal Cognitive Assessment (MoCA). Acceptability was assessed through a questionnaire created by the researchers themselves. Adherence was assessed by the “frequency of the number of elderly individuals who completed the interventions and safety through the presence of adverse effects.” Participants were assessed immediately pre- and posttreatment and fourth week after the end of the treatment. Statistical analysis was done through repeated-measures analysis of variance and Tukey post hoc test.
Results:
Both groups presented a significant improvement in the PC (Mini-BEST), gait (FGA), and cognition (MoCA) posttreatment that was maintained at fourth week after treatment (post hoc Tukey test; P < 0.05). Regarding cardiorespiratory fitness (6MST), the KATG presented improvement posttreatment and maintenance of the results in the fourth week after treatment. CPTG showed improvement only in fourth week after treatment (post hoc Tukey tests; P < 0.05). Regarding the acceptability, the questionnaire showed that both groups were satisfied with regard to the proposed interventions. There was 91% adherence in both training sessions. Regarding the safety, 34% and 26% of the individuals of the KATG and CPTG, respectively, presented adverse effects of delayed muscle pain in the lower limbs after the first session only.
Conclusion:
There were no significant differences between the KATG and CPTG; both interventions provided positive effects on PC, gait, cardiorespiratory fitness, and cognition of the elderly.
Introduction
T
Studies have shown that alterations in this important function may be associated with gait changes and cognition of the elderly. In addition, indirectly it is related to changes in the cardiorespiratory fitness and mood of these individuals. These impairments can influence the quality of life of this population.2,7,9,10
Studies have shown that physiotherapy through conventional exercises such as balance training,11–14 aerobic exercises, 15 motor coordination,15,16 muscle strength,15,16 and others is effective for minimizing these declines and may provide an increase in the functional reserve of the impaired function. Another modality that has recently been studied in both the prevention and rehabilitation of motor, cognitive, and cardiorespiratory functions of the elderly is virtual reality (VR). VR is defined as the simulation, in real time, of an environment, scenario, or activity where the individual can interact. 17 This technology aims to recreate the sensation of reality for the individual, promoting the capacity to constantly measure and evaluate their performance. 17 In addition, this modality uses virtual games with different cognitive, motor, and cardiorespiratory demands that allow feedback on performance and results of the individual.17–20
The main outcomes studied in research involving VR are as follows: gait,21,22 balance,20,21,23–27 number of falls,24,26,28 muscle strength,21,29 cognition, 30 depression, 28 cardiorespiratory fitness,29,31,32 and VR applicability. 32 One variable that has been extensively investigated in VR through the Kinect system is PC.23,27,33,34 Although there are an expressive number of studies in this area, recently a systematic review pointed out methodological gaps, such as small number of participants,18,35 lack of control group,18,35 poor description of the interventions,18,36 few intervention sessions,35,36 lack of follow-up,18,35 and outcomes assessed through clinical scales without good sensibility and specificity. 35
Another important issue about this feature is being aware of its advantages and disadvantages. It can be observed that the majority of studies involving this type of technology as a therapeutic modality only pay attention to the results, leaving aside the explicit description of the advantages and, mainly, the disadvantages. However, some studies were found in the literature that pointed out some of the benefits of this modality as a therapeutic resource: the motor requirement of virtual tasks of the system such as weight shifting, symmetric foot stepping, and controlled movements near the limits of stability, as well as the high number of repetitions and variability in a complex and motivating environment that provides visual and auditory feedback and reinforcement, which creates dynamic patient–task interaction. 37 Together, these advantages can improve the motor learning process and improve the acquisition or improvement of new motor task performance. 38 Moreover, due to the complexity of tasks that involve cognitive stimulation, as well as motor skills, VR could promote improved integration of motor and cognitive abilities that may contribute to increased independence in daily life compared with balance exercise training based on motor stimulation alone. 33 Still thinking of advantages dos Sandos Mendes et al., 38 drew attention to the performance of tasks that cannot feasibly be performed safely in a real-world environment; intensive repetition of complex tasks directed by visual and immediate feedback on performance and results; and a more motivating training environment. 39 Annesi and Mazas 40 and Lewis and Rosie 41 state that these devices (e.g., Nintendo®, Wii™, Microsoft Kinect for Xbox®, and Fitbit) are relatively inexpensive (A$80–400), widely available, and have been shown to enhance enjoyment of exercise.
Considering the disadvantages, the scientific field is scarce as mentioned above; studies do not explore this strand. However, we can suggest that commercial videogames were not developed specifically for the elderly or individuals with neurological alterations, which could hamper the applicability to these populations due to the possible complexity of tasks and highly challenging motor and cognitive demands. However, studies have shown that these interactive videogames are applicable and safe for these individuals.23,26,27,33,34 Another possible disadvantage could be the difficulty that elderly individuals can have to install and select the appropriate games for specific training.
The aim of this study was to compare the effects of Kinect Adventures games versus conventional physiotherapy on PC, gait, cardiorespiratory fitness, and cognition of community dwelling elderly people. In addition, we evaluated the acceptability, adherence, and safety of the interventions. Our clinical hypothesis was that intervention based on the Kinect Adventures games would be superior to conventional physiotherapy, for the following reasons: the games offer higher visual and auditory feedback, motivation, and cognitive demands than conventional physiotherapy. In addition, the score system related to the performance can increase the engagement of the participants.
Materials and Methods
Design
This study is a parallel group, single-blind randomized controlled trial, with two intervention groups as follows: Kinect Adventures games group (Kinect Adventures Training Group [KATG]) and Conventional Physical Therapy Exercises group (Conventional Physical Therapy Group [CPTG]). The current study was developed based on the Consolidated Standards of Reporting Trials (CONSORT} statement.
Randomization and masking
Patients were randomly assigned (1:1), with a secure remote, with a computer-generated block randomization procedure (block size of six) by a researcher not involved in the trial, to receive intervention based on Kinect Adventures games or conventional physiotherapy. Below is the flow diagram based on the CONSORT statement (Fig. 1).

Flow diagram.
Ethical approval and consent to participate
This study was approved by the Ethics Committee of the Medical School of the University of Sao Paulo, Brazil (1.184.941) (Certificate of Presentation for Ethical Appreciation [CAAE]: 45547415.8.0000.0065) (Attachment 1) and registered in the Brazilian Registry of Clinical Trials (RBR-4z4f48) in November/2015.
Study settings
The study was conducted at the Clinics Hospital of the School of Medicine of the University of São Paulo, Brazil.
Participants
Eligible participants were community dwelling elderly individuals living in the city of Sao Paulo, Brazil, aged between 60 and 80 years, both genders, capable of walking without assistance, with normal or corrected visual and auditory acuity, without any decompensated disease, capable of understanding and interacting with the Kinect games, but without previous experience with them, and who agreed to sign the Free and Informed Consent Term (see Supplementary Material at http://online.liebertpub.com/doi/suppl/10.1089/g4h.2017.0065). The issue of being able to understand and interact with the game was tested through a familiarization session. In this session the therapist presented the equipment and explained all the rules of each game. Subsequently, the subjects practiced two attempts at familiarization with each game, performed with the aid of the examiner to correct the movements and posture of the individuals through manual guidance and verbal commands, instructing them on the best and most correct way to perform the movement to achieve the goal of the game. To assess the inclusion or not of the individual, performance in the games in these familiarization sessions was used. The individual who scored zero in the familiarization session was excluded. The exclusion criteria were as follows: older adults who, during the period of the study, presented any clinical changes that could preclude the performance of physical exercises in an orthostatic position, such as cardiovascular, orthopedic, or neurological conditions, and older adults unable to interact with the games.
Administration of assessments
The same trained blind researcher evaluates participants of both groups at three moments: “pretreatment assessment,” “posttreatment assessment,” and “in the fourth week after treatment.” In the first evaluation the evaluator applied to the patient a free informed consent term, in which it also contained information on the possible benefits that the interventions may bring and possible damages and indemnities to patients, also emphasizing that the patient could withdraw from the research at any time without any contradictions. The benefits mentioned above are improvement in PC, gait, cardiorespiratory fitness, and cognition, while the possible damages are dizziness, nausea, imbalance, and fatigue. On this day the evaluator clarified all doubts regarding the research project and informed the volunteers that all data resulting from the survey be used for scientific purposes.
Interventions
The protocols were developed to guarantee the same intensity and quantity of exercises for both groups. The intensity of interventions proposed for both conventional physiotherapy and Kinect Adventures was adjusted to achieve moderate intensity, a level at which research in both areas is suggested as effective.42–45 As for the quantity, the two groups performed the same intervention period, a total of 14 sessions divided into two sessions a week, 60-minute duration each intervention, with the following interval between exercises: 2 minutes of activity and 2 minutes of rest. The goal of resting time was to avoid fatigue among participants. That is, the individuals performed the same intervention time and the same intensity. However, despite all this methodological care, it is not possible to guarantee that the intensity of the interventions was the same since the motor and cognitive demands of each training protocol are different.
The CPTG performed conventional physical therapy exercises in a group-training program of six participants supervised by a physical therapist. The CPTG protocol was based on other studies that aimed to train PC in the elderly11,16,46–49 and included seven different specific exercises lasting 10 minutes each: (1) warm-up; (2) static and dynamic balance; (3) endurance; (4) muscle strength; (5) motor coordination; (6) muscle stretching exercises; and (7) cool down. The best description of this training is as follows: (1) was performed by walking, (2a) static balance training was performed by means of exercise on the balance disc and circular balance board, (2b) dynamic balance training through two circuits: with unstable ground associated with upper and lower limb movements, and (3, 4) were performed by raising and lowering the front and lateral steps and performing plantar flexion. A shoulder adduction exercise was also performed by tightening a ball with the hands and hip adduction, tightening a ball between the knees, (5) consisted of a circuit where the patient had to move on their back, (6) consisted of global stretches, and (7) consisted of respiratory exercises and joint mobilizations of the cervical, upper, and lower limbs.
The KATG performed individual sessions through Xbox Kinect Adventures games. In each training session, the participants played four games and were allowed five attempts at each game, without interference from the physical therapist. Participants played the games in front of a 50′′ TV at a distance of 3 m from the 360 videogame console and Kinect sensor. Kinect games are based on the capture of the player's movements through cameras with infrared sensors. Thus, the movement of the player captured by the camera is reproduced by an avatar in the virtual environment. 17 Therefore, the elderly individuals interacted with the games through body movements according to the rules of each game. Overall, the games stimulate faster multidirectional movements and center of gravity control, through multidirectional steps, squats, jumps, coordinated movements of the upper and lower limbs, and trunk movements in three planes. 17 In addition, the games include cognitive demands such as fast decision making, environmental monitoring, selection of visual stimuli, inhibition of responses, and divided attention.17,18
Games were selected based on their motor and cognitive demands. The selected games promoted: (1) constant displacement of the patient's center of mass through movement of upper limbs; (2) transference of weight between lower limbs; (3) crouching; and (4) inclinations of the trunk. Motor stimulation demands balance reactions and continuous postural adjustments associated with fast movement of the limbs. The main cognitive demands of all games were: (1) visuospatial attention; (2) shifting of attention; (3) decision making; (4) fast reaction time; and (5) immediate planning and execution. In the first stage of the study, four patients played the Kinect Adventures games. These patients did not participate in any other phases of this study. In general, Kinect Adventures games use whole-body motion to allow the player to engage in various mini-games with the goal of obtaining the highest number of adventure points, which are collected in different ways. Adventure points earn medals and affect game progression. Three physical therapists performed a qualitative analysis of the patients' performance in each of the games, and the motor and cognitive requirements of the games were described.34,50,51
Regarding conventional physiotherapy, the training proposed was based on studies that used these training modalities specifically for the elderly, as already mentioned in the text in the chapter on interventions. Given this scenario, this question can be answered in future studies.
Below is a description of the four selected games: “Space Pop,” “20,000 Leaks,” “Reflex Ridge,” and “River Rush”. In the “20,000 Leaks” game the avatar of the player is inside a glass cube on the seabed, and fish and sharks begin to stick to the glass, which causes water to enter the cube. The player's goal is to plug the holes with their hands and feet, which require rapid limb movements. In the “Space Pop” game several bubbles appear on the screen, and the player must fly by flapping their arms like a bird to pop the bubbles. In the “Reflex Ridge” game the player moves around on a platform on a track and must avoid obstacles by rapidly shifting sideways or bending down. In the “River Rush” game the avatar of the player is in a boat and must move downstream. To move the boat, the player needs to move their body to each side.
Tables 1 and 2 describe the cognitive and motor demands of each training method.
Outcome measures
Sociodemographic data were collected from individuals, such as age, weight, height, body mass index, gender, number of diseases, and number of drugs. Physical activity level was measured through the International Physical Activity Questionnaire.
The primary outcome was PC, assessed by the Mini-Balance Evaluation Systems Test(Mini-BESTest), which consists of 14 items that focus on dynamic balance, comprising four areas as follows: (1) anticipatory postural adjustments; (2) postural responses; (3) sensory orientation; and (4) balance during walking. Each item is scored from zero to two; a score of zero indicates that a person is unable to perform the task, while a score of two is normal. 52
The secondary outcomes were gait evaluated by the Functional Gait Assessment (FGA), which assesses postural stability under various conditions of gait. 53 Cardiorespiratory Fitness, assessed by the six-minute step test (6MST) in which the subjects were instructed to walk up and down a step for 6 minutes, aiming at the highest possible number of steps in the time (free rhythm), without the support of the upper limbs, which remained stationary alongside the body. 54 The cognition was assessed by the Montreal Cognitive Assessment (MoCA) which is a brief cognitive evaluation test, specifically developed for the assessment of mild forms of cognitive impairment, which provides a quick measure of the global cognitive status of the subject.55,56 The acceptability was evaluated by means of a questionnaire elaborated by the researchers, in which participants answered the following questions: (1) “what did you think about the games/conventional physiotherapy”, (2) “which game/exercise did you like more”, (3) “which game/exercise did you find easiest”, (4) “which game/exercise did you find most difficult”, (5) “what did you think about the number of attempts of each game/exercise”, (6) “did you understand why it was required to perform every game/exercise”, (7) “did you feel any discomfort while playing the games/doing exercises”, (8) “did you feel motivated to perform the games/exercises”, (9) “did you notice any improvement in your balance, gait, breathing, or memory after these interventions”, (10) “would you imagine playing these games/doing these exercises at home”,(11) “would you indicate these games/exercises to someone else”, (12) “what did you think about the intervention duration”, and (13) “would you continue to carry out this intervention after the end of this project?”
Adherence was assessed by the frequency of the number of elderly individuals who completed the interventions and safety through the presence of adverse effects such as muscle pain in the lower limbs and or in the upper limbs, dizziness, nausea, vomiting, and falling.
The elderly of the two groups were assessed by a blinded assessor before and after the 14 training sessions and 30 days after the end of the intervention (follow-up), respectively, named “Pretreatment assessment,” “Posttreatment assessment,” and “Fourth week assessment after treatment.”
Sample size calculation and statistical analysis
Sample size calculation was based on the results of a pilot study in which we assessed the effects of Kinect Adventures games on PC of 10 community dwelling elderly people. A difference of 20% between pre- and postintervention of the Mini- BESTest score was adopted as a clinically important improvement. A sample of 46 elderly (23 per group) was estimated to provide a power of 80% to detect a significant intervention effect (two side, P = 0.05). To establish if there were any significant differences between the KATG and the CPTG at the baseline on levels of age, years of education, number of comorbidities, medication in use, and level of physical activity between groups, t-tests was conducted. A series of chi-square tests were conducted to establish if there was difference between groups and the demographic variables of relationship status and gender. The KATG and CPTG groups were compared in relation to pre, post, and follow-up, respectively, named “Pretreatment Assessment,” “Posttreatment assessment,” and “The fourth week assessment after treatment.” Changes in PC, gait, cardiorespiratory aptitude, and cognition were measured using repeated-measures analysis of variance (RM-ANOVA). All the effect sizes were calculated. The alpha of 0.05 was adopted to indicate statistical significance. All statistical analyses were performed with the Dell™ Statistica™ 13.0 software (2015).
Results
Participant characteristics at baseline
Demographic and clinical characteristics at baseline of the elderly participants in the two groups are presented in Table 3. There were no significant differences between the two groups. Forty-six individuals (12 men and 34 women) with a mean age of 69.3 (standard deviation 5.3) years participated in this study.
Mann–Whitney test; #probability ratio test.
SD, standard deviation; Q1, first quartile; Q3, third quartile; BMI, body mass index; IPAQ, International Physical Activity Questionnaire.
Primary and secondary outcomes
The mean values and standard deviations of the scores obtained in the Mini-BESTest, FGA, 6MST, and MoCA in the evaluations: “pretreatment assessment,” “posttreatment assessment,” and “fourth week assessment after treatment” and the mean difference between posttreatment assessment and pretreatment assessment and fourth week assessment after treatment and pretreatment assessment with 95% confidence interval can be observed in Table 4.
Post hoc Tukey tests: pretreatment × posttreatment and pretreatment × fourth week after treatment comparison: P < 0.005.
Post hoc Tukey tests: pretreatment × posttreatment and pretreatment × fourth week after treatment comparison: P < 0.001.
Post hoc Tukey tests: pretreatment × posttreatment and pretreatment × fourth week after treatment comparison: P < 0.05.
RM-ANOVA, repeated-measures analysis of variance; CI, confidence interval.
Primary outcomes
PC: Mini-BESTest
There was a significant effect of evaluation, without group effect or interaction between factors, in the Mini-BESTest (RM-ANOVA, P < 0.0001, Table 4; Fig. 2). Both groups showed improvement in the Mini-BESTest posttreatment assessment that was maintained at fourth week assessment after treatment (Tukey post hoc test, P < 0.05).
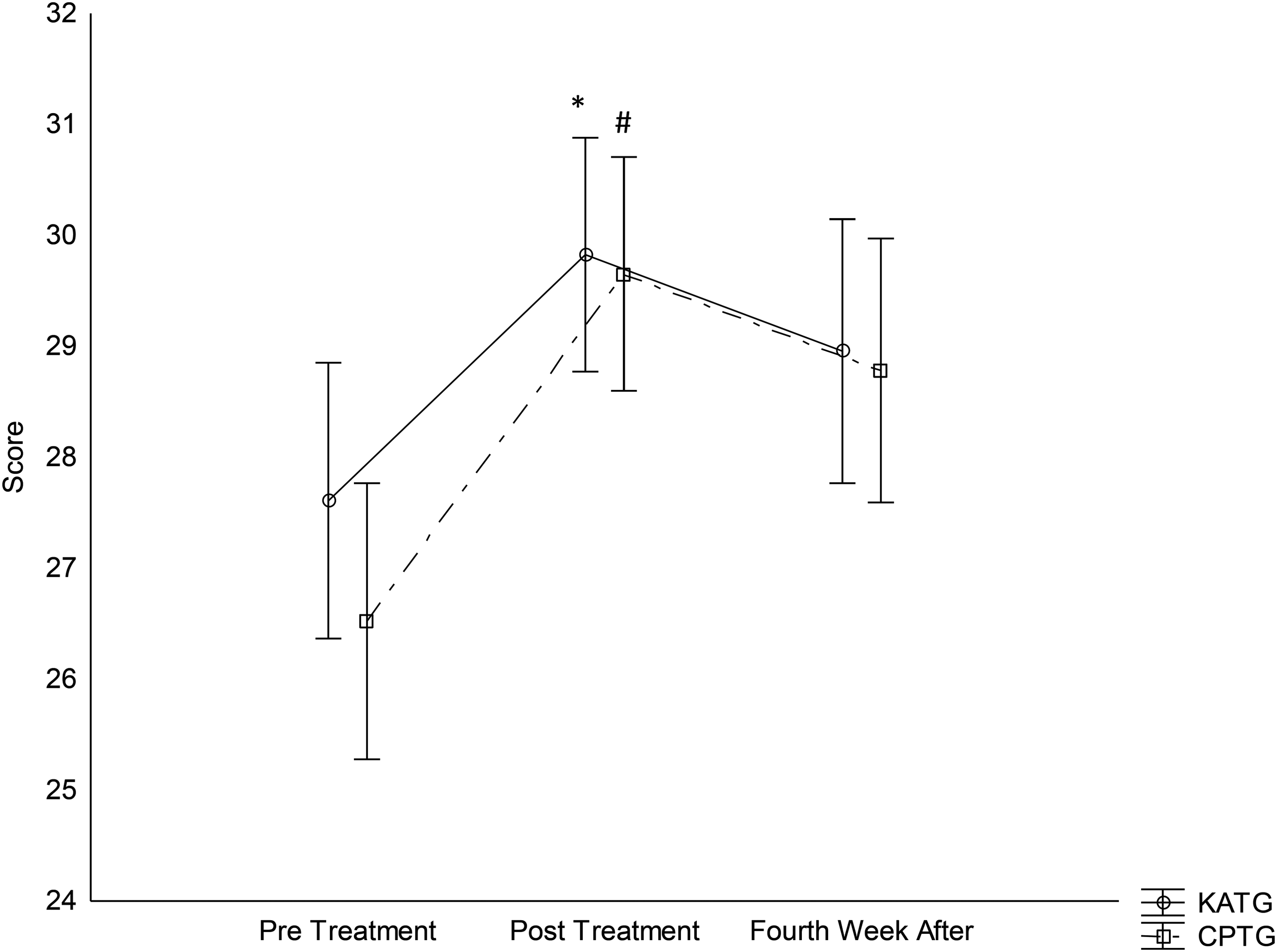
Postural control through Mini-Balance Evaluation Systems Test. Post hoc Tukey test: *P < 0.005; #P < 0.001
Secondary outcomes
Gait: FGA
There was a significant effect of evaluation, without group effect or interaction between factors, in the FGA (RM-ANOVA, P < 0.0001, Table 4). Both groups showed improvement in the FGA posttreatment assessment that was maintained at fourth week assessment after treatment (Tukey post hoc test, P < 0.05).
Cardiorespiratory fitness: 6MST
There was a significant effect of evaluation, without group effect or interaction between factors, in 6MST (RM-ANOVA, P < 0.0001, Table 4). The KATG showed improvement in 6MST posttreatment assessment that was maintained at fourth week assessment after treatment (Tukey post hoc test, P < 0.05). In contrast, the CPTG showed improvement in the 6MST in the fourth week assessment after treatment compared to pretreatment assessment (Tukey post hoc test, P < 0.05).
Cognition: MoCA
There was a significant effect of evaluation, without group effect or interaction between factors, in MoCA (RM-ANOVA, P < 0.0001, Table 4). Both groups showed improvement in the MoCA posttreatment assessment that was maintained at fourth week assessment after treatment (Tukey post hoc test, P < 0.05).
Acceptability
Regarding acceptability: (1) 91% of participants in the KATG group rated the intervention as optimal and 9% of this group rated it as very good. In the CPTG group, 86% of the elderly classified the intervention as optimal and 14% as very good. (2) Ninety-one percent of the elderly in the KATG group reported that they liked the game “20,000 Leaks” the most and 9% liked the “Space Pop” game. Eighty-nine percent of the elderly in the CPTG group liked the static and dynamic balance exercises and 11% the muscle strength exercises. (3) Eighty-three percent of KATG participants rated the game “20,000 Leaks” as the easiest, 9% the “Space Pop” game; and 8% “River Rush”. Eighty-seven of the participants in the CPTG group rated muscle strength exercises as the easiest and 13% motor coordination exercises. (4) Ninety-one percent of KATG participants ranked “Reflex Ridge” as the hardest and 9% “River Rush”. Regarding the CPTG, 86% classified static and dynamic balance exercises as the most difficult and 14% endurance exercises. (5) Both groups rated the number of trials as appropriate. (6) Both groups reported understanding what was required in both interventions. (7) 34% and 26% of the individuals in the KATG and CPTG, respectively, presented delayed muscle pain in the lower limbs after the first session only. (8) Both groups reported feeling motivated to perform the interventions. (9) Thirty-four percent and twenty-six percent of the individuals in the KATG and CPTG, respectively, presented delayed muscle pain in the lower limbs after the first session only. Eighty-six percent of participants in the KATG group reported improvement in balance, breathing, gait, and cognition and 14% in walking and breathing, while 91% of the elderly in the CPTG reported improvement in balance, gait, and cognition and 9% in respiration and gait. (10) One hundred percent of the KATG group reported imagining playing the game at home, while 91% of the CPTG reported performing the exercises at home, and 9% of the elderly would not like to perform the exercises at home. (11) One hundred percent of the elderly of both groups reported indicating the interventions to other people and finding the duration appropriate for them. (12) 87% of the KATG and 9% of the CPTG reported that the duration of the intervention was low, while 13% of KATG and 91% of the CPTG reported that the duration of the intervention was adequate. (13) One hundred percent of the elderly in both groups reported intending to continue the interventions.
Adherence and safety to training and adverse effects
Regarding the adverse effects, 34% and 26% of the individuals of the KATG and CPTG, respectively, presented delayed muscle pain in the lower limbs after the first session only. There was 91.31% adherence in both training sessions. These values can be seen in Figure 1.
Discussion
The objective of this study was to investigate the effectiveness of a VR based intervention through Kinect Adventures commercial games versus conventional physical therapy to improve PC, gait, cardiorespiratory fitness, and cognition of the community dwelling elderly. Our clinical hypothesis was that the VR intervention based on the Kinect Adventures games would be superior to conventional physiotherapy. However, the results showed that there was no difference between groups regarding the effectiveness to improve PC, gait, cardiorespiratory fitness, and cognition in which both interventions promoted positive effects on these outcomes. In other words, the main finding of this study was that the effect of the KATG was equal to that of the CPTG. Regarding the cost, the Kinect is more expensive as the intervention was performed individually while the conventional physical therapy was performed in a group of six individuals at the same time. Considering the cost of the Kinect, projector, the screen, and the individuals/therapist ratio, the intervention based on the Kinect can be considered more expensive than the conventional physical therapy.
We postulated that both groups promoted positive effects through different characteristics of the intervention. Conventional physical therapy could improve PC through high challenge balance exercises in group.11,49,57 On the other hand, the high cognitive and motor demands present in the Kinect Adventures games, as well as the visual and auditory feedback factors on performance and results,17,18,58 through an attentive external focus should not only have immediate effects on performance but also work as a learning facilitator.17,58
In fact, studies have shown that VR20,23,27,32 and conventional physical therapy11,49,57 can improve anticipatory postural adjustments, postural responses, sensory orientation, and balance during gait of the elderly.
In the current literature there are studies that corroborate with the present results. Bieryla and Dold 27 investigated the applicability of the Wii Balance Board compared to conventional balance training in the balance of the elderly. The research reported an improvement in the balance of the experimental group. In this study, the number of participants was small, requiring further studies. Karahan et al. 20 compared the effects of virtual games through the Xbox Kinect versus home-based balance training on the PC, functional mobility, and quality of life of these individuals. There was an improvement in both groups; however, the group that performed the games stood out. In a similar way Sato et al. 21 analyzed the effects of virtual games through the Xbox Kinect on the balance and muscle strength of the elderly. In this study, the experimental group performed the intervention through the Xbox Kinect, and the control group did not perform any activity. A superior improvement was observed in the experimental group in relation to the control group. Toulotte et al. 25 compared the efficacy of three protocols as follows: adapted physical activities; Wii Fit™; and adapted physical activities + Wii Fit on the balance of the elderly. They showed improvement in the three groups analyzed. Similarly, Yeşilyaprak et al. 26 investigated the effects of VR versus conventional balancing exercise on balance and risk of falls in people over 60 years old in nursing homes. The results were effective indicating that both groups presented statistically significant improvement in the analyzed variables and there was no difference between groups. Differing somewhat from the present study Ofli et al. 32 verified the effects of virtual games developed by the researchers on the balance, aerobic endurance physical fitness, muscle strength, and agility of the elderly through a pilot study. In this study, only the quality of life presented positive results. Similar results to the above study were also found in the study by Franco et al. 22 who compared the effects of the Nintendo Wii Fit versus an equilibrium workout on balance and risk of falls in the elderly.
In relation to cardiorespiratory fitness, the results were effective for the KATG at all moments of the evaluations. Already CPTG showed improvement only in the fourth week assessment after treatment, but there was no superiority between the groups. In the current literature, studies that investigated the effects of virtual games on cardiorespiratory fitness are more concentrated on children and adolescents. 59 The improvement reported in the present study may have occurred due to the cardiopulmonary demands of the games performed with interval training. 60 Four different games were played, and each game lasted ∼12.5 minutes followed by a 3 minute rest interval each time a game was changed. This training regimen could have contributed to the improved physical condition of the participants. 61 However, cardiac parameters were not monitored during the protocol. Ruivo 62 conducted a systematic review, in which the researcher investigated whether videogames are effective for the health of adults and the elderly and whether it can be used in the area of cardiac rehabilitation. The researchers showed that it was not possible to conclude the real effects of these games on cardiorespiratory fitness of this population due to the lack of studies in the area.
Kinect Adventures games stimulate anteroposterior and mediolateral displacement of the center of gravity, multidirectional steps, movements of the upper limbs, lowering, lifting, and moving the center of gravity laterally, multidirectional steps, movements of the lower limbs and head, anticipatory control of balance, upper limb movements appropriate to the orientation of the spheres, lowering the center of gravity, lateral steps to dodge, and jump lateral–lateral displacement of the center of gravity or lateral steps and jumps. 63 In general, these motor demands are frequently used in conventional balance training or aerobic training.11,15,47,48,64 We speculate that these motor requirements could be related to the improvement in PC and gait of the KATG. A systematic review of the health benefits of multicomponent training programs in seniors reported that multicomponent training has a significant beneficial effect on cardiorespiratory fitness, metabolic outcomes, and functional and cognitive performance of elderly individuals. 65
In addition, videogames can help elderly people to achieve the recommendation of the American College of Sports Medicine, which stresses aerobic activities taking into account the older adult's aerobic fitness, activities that maintain or increase flexibility, and balance exercises for older adults. 66
Despite their age, all participants in this study were able to understand and interact with the Kinect games. During the training sessions, the elderly progressively increased their scores in the games. As the scores are related to the success in performing the virtual tasks, we believe that the participants had the necessary ability and capacity to interact with the games. In fact, several studies have shown that videogames are feasible, acceptable, and safe for elderly people with or without neurological diseases.33,34,67,68
Regarding cognition, the studies that used VR to train this function show positive and motivating results. Toril et al. 69 conducted a meta-analysis to investigate the effects of videogame on the cognition of healthy elderly. The results indicated that this type of intervention produces positive effects in several cognitive functions, which mainly include reaction time, attention, memory, and global cognition. The findings suggest that cognitive and neural plasticity is maintained until some point of aging and, therefore, the importance of stimulating this crucial function during senescence, concluding that training older people using videogames effectively increases these cognitive functions.
Kueider et al. 70 produced a systematic review which stated that interventions using VR can improve the cognitive performance of community's seniors and that this improvement may last for 5 years. Good results were also found in the study by Nouchi et al., 71 in which researchers investigated the effect of Nintendo on elderly's cognition during a training period of only 4 weeks, 15 minutes per day, and concluded that the training was effective. Researchers have suggested that it is possible to improve this important function through short-time VR training.
Corroborating with these studies, Kayama et al. 72 investigated the effects on the cognition of community dwelling elderly produced by a 12-week training using a virtual game developed by the researchers. The results obtained were that these games are effective for improving cognition of elderly, mainly the executive domain.
Promising results were also obtained in the study of Park and Yim 73 in which researchers investigated the effectiveness of a three-dimensional VR program in community dwelling elderly's cognition, muscle strength, and balance. They concluded, this way, that the intervention was effective for all variables investigated.
What we can highlight in our study is that, although the intervention through the games Kinect Adventures is a training that involves the global movement of the body, that is, demanded a lot of motor demand associated with the cognitive, these games were effective for the cognition of the elderly. Thus, motor overload did not prevent cognitive gains, which give us confidence to affirm that it is indeed possible to train motor and cognitive functions in an integrated and joint way.
Our results showed that there was no difference between the groups regarding adherence and adverse events. Both groups presented excellent adherence and a low incidence of adverse events, suggesting that both interventions can be considered safe and feasible for elderly people. The adverse event of the participants in this study was delayed muscle pain in the lower limbs after the first session in both groups. Delayed-onset muscle soreness is a sensation of pain, stiffness, and muscle soreness, commonly experienced after unaccustomed strenuous exercises, particularly those involving eccentric contractions. Delayed-onset muscle soreness reaches its peak intensity of symptoms at 24–72 hours after cessation of exercise, sometimes requiring a week to recover.74,75 We speculate that the motor demand of both interventions could stimulate eccentric contractions during the training. The Kinect games required jumping, crouching, and fast displacement, which could stimulate eccentric muscle contraction. A similar requirement can be found in the conventional physical therapy group. Some exercises, for example, sit-to-stand as fast as possible, stimulate eccentric muscle contractions. Our results are in disagreement with the study of Pompeu et al., 34 in which there were no adverse events of using the same Kinect Adventures games in individuals with Parkinson's disease. Maybe because individuals with Parkinson's disease, due to their motor deficiencies, can present limitations to perform fast movements that can decrease the level of eccentric muscle contraction.
We assessed the acceptability of the interventions through a questionnaire based on questions about the perception of the participants regarding the games and conventional physical therapy. The acceptability of both groups was very good. Our results are in agreement with studies that evaluated the applicability and acceptability of virtual games.67,68,76,77
There are some advantages of videogames. One is that videogames are designed to be fun and motivating and, therefore, may increase the amount of time the user spends on the therapeutic activity. Hassett et al. 78 published a protocol in which they assessed the effects of the addition of affordable technology to usual care on physical activity and mobility in people with mobility limitations admitted to inpatient elderly and neurological rehabilitation units, compared to usual care in isolation. The authors speculate that affordable technology, including videogames, can increase the level of physical activity of elderly and neurological individuals.”
In relation to VR through Kinect Adventures, we can highlight that these games have different motor and cognitive abilities, such as multidirectional displacements, weight transfer, controlled movements close to stability limits, high number of repetitions, auditory and visual feedback, attention, planning, decision making, and concentration, and thus generate motivation and commitment in the tasks performed. 37 One study showed that the high demand of these cognitive and motor stimuli can promote a process of motor learning, thus facilitating the individual to transfer acquired skills to everyday life. 33 The activities are graded, structured, and provide detailed feedback on performance, thereby incorporating factors thought to be important in learning new skills. 79 We speculate that the challenge of the games to increase the scores and the reinforcement offered by the successful trials can provide more motivation and higher engagement of the participants. Another important advantage of the Kinect Adventures is the ability to control the demand and intensity of tasks easily and quickly. For example, it is possible to change the level of difficulty of the games in just a few seconds, and the demands can be changed by simply selecting different games. This advantage could facilitate the clinical use of the Kinect for different populations due to the ability to adjust the level of intensity and possibility of selecting the demand specifically to the characteristics of each individual.
Regarding the disadvantages, we can highlight that despite the effective results, commercial videogames were not developed specifically for the elderly or individuals with neurological alterations, which could hinder the applicability to these populations due to the possible complexity of tasks and highly challenging motor and cognitive demands.
As the world population is aging, studies on the socioeconomic and health consequences are proliferating. Little has been done on the effectiveness and impact elderly may benefit from the use of technology in their everyday life. The pilot study, implemented within a funded project aimed at identifying sustainable actions to promote Seniors' quality of life, intended to investigate this kind of interaction in terms of accessibility and acceptability that senior citizens experience with technological devices promoting motor and cognitive training. In the hypothesis, interfaces and technological artifacts, which still take in little account the seniors' physical characteristics (e.g., physiological limitations in sight, hearing, and movement) and cognitive processes (selective memory often driven by practical needs), can cause elderly to mistrust technology. Study participants were 20 with over 70-year-old people, who were observed and interviewed in context in a 2-hour training session regarding the technological device user experience. The results are presented with scenario-based techniques that help represent typologies of users in different use situations. Findings confirm the hypothesis, highlighting that elderly may accept technological artifacts when they perceive them as bringing benefits in terms of well-being and health.
However, studies showed that these interactive videogames are applicable and safe for these individuals.23,26,27,33,34
Another possible disadvantage could be the difficulty that elderly individuals have to install and select the appropriate games for specific training. One limitation of the Kinect games is that the system can be played individually or in pairs, while conventional physical therapy can be performed in a group. This factor can increase the cost of the videogame intervention and decrease social integration. As social isolation can negatively affect health and well-being, 80 we believe that interventions that stimulate social integration should be prioritized.
As Kinect Adventures training, conventional physiotherapy presents advantages and disadvantages. One advantage is the possibility to perform group session training favoring the interaction among participants. Other advantage of conventional physiotherapy is the better control of the intensity of the exercises. In contrast, conventional physiotherapy cannot provide augmented visual and auditory feedback at the same level that the videogames offer.
The results of the present study showed that both conventional physiotherapy and Kinect Adventures games provided positive effects on PC, gait, cardiorespiratory fitness, and the cognition of the elderly in the community. However, two methodological limitations occurred as follows: (1) it was not possible to blind participants on the type of intervention they received; and (2) the cardiorespiratory fitness variables were not monitored, which made it difficult to analyze the intensity of the intervention through Kinect Adventures games and detailed analysis of each game.
Conclusion
The results of this study suggested that both Kinect Adventures games and conventional physical therapy are acceptable and provided positive effects on the PC, gait, cardiorespiratory fitness, and cognition of the community dwelling elderly. Although the use of Kinect games is considered to be safe, all patients were supervised and received initial instructions from a physical therapist. In view of these findings, we can conclude that Kinect Adventures games could be a complementary and useful tool aimed at prevention of motor and cognitive changes in clinical practice with the elderly.
Footnotes
Acknowledgments
The authors thank all professionals who participated in this study: Adriana Cerqueira, Amanda Veronica de Souza, Aparecida Rosa Botelho, Fabiana Cassales Tosi, José Bussamra Filho, Juliana Magalhães, Maria do Socorro Morais Pereira Simões, Railla Pinheiro Alvarez, Rosemeyre Alcarde Nuvolini, Sara Novak, team of the Movement Study Laboratory of the Institute of Orthopedics and Traumatology of University of Sao Paulo, and all elderly volunteers.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.