
Abstract
Abstract
Objective:
Finding suitable and engaging ways for older people living in long-term care (LTC) to engage in physical activity, to maintain function is challenging. There is a need to explore the use of exergames for LTC residents who have mobility and cognitive impairments. We investigated the effect of a group-based Xbox Kinect (Microsoft Corp., Redmond, WA) exergame program on mobility in LTC residents with and without cognitive impairment.
Methods:
Facilities were randomly assigned to the intervention (four facilities, n = 29, aged 84.7 ± 7.4 years) or control group (five facilities, n = 36, aged 85.8 ± 7.2 years). The intervention group played Xbox Kinect exergames twice weekly for 8 weeks. The control group continued usual activities. The primary outcome measure was mobility, assessed pre- and postintervention using the de Morton Mobility Index (DEMMI).
Results:
DEMMI scores improved in residents who played exergames, although this did not reach significance (P = 0.06). There was no interaction between cognition scores and DEMMI scores (P = 0.86). Participants attended an average of 55% of scheduled exergames sessions.
Conclusion:
The trend toward improvement in mobility, as well as attendance rates indicate that the Xbox Kinect exergames were engaging for a proportion of residents. On this basis, further exergames development for LTC residents warrants attention.
Introduction
E
Exergames offer promise, because they address the motivation and enjoyment aspects of physical activity. We have found that exergames increase energy expenditure in community-dwelling older people, with the energy cost equivalent to light intensity physical activity. 10 Exergames can also improve balance and mobility in community-dwelling older people.11,12 Whether exergames might also benefit LTC residents, who are generally older and more disabled has received less attention. Two studies using dance games13,14 and one using Wii-Fit™ 15 showed improvements in gait parameters and balance in LTC residents. Improvements in balance and mobility were also demonstrated following the use of exergames for rehabilitation of hospitalized older people. 16
However, with the exception of one pilot study 15 studies have excluded participants with cognitive impairment. Given that 40% of LTC residents have moderate to severe cognitive impairment,17,18 their inclusion in studies of LTC is important. On this basis, the aim of this trial was to examine whether a group-based exergame program could improve mobility in LTC residents, including those with and without cognitive impairment.
Methods
A two-arm cluster randomized controlled trial design was used to determine whether an exergame program could improve mobility of LTC residents. The trial was conducted between March 2014 and June 2015 after receiving ethical approval from the Institutional Ethics Committee. Written informed consent was obtained from each facility and from all participants, or in the case of those unable to give informed consent their enduring power of attorney/next of kin, before study commencement. The trial was registered with the Australian New Zealand Clinical Trials Registry (Trial registration number ACTRN12614000116628).
Participants and recruitment
Nine low-level dependency LTC facilities in one city were recruited through advertisements in a national LTC facility newsletter and by direct approach to the LTC management. Low-level dependency residents are those who need assistance with most instrumental activities of daily living and some activities of daily living but usually can ambulate and feed themselves. Residents, identified by facility staff as eligible, were invited to participate.
Eligible residents were those aged 65 years or over, who could mobilize independently with or without a walking aid, and who were deemed able to understand the study measure instructions. We excluded residents who were acutely unwell; or had a visual impairment, such that they could not see a large television screen as required for the intervention.
Randomization and blinding
After collection of baseline data, a biostatistician not involved in the study randomized facilities to the intervention or control group using computer-generated random numbers. The allocation was emailed to the principal investigator to ensure allocation concealment. We randomized by facility (cluster) to avoid contamination between intervention and control groups. It was not possible to blind study participants to the intervention. Outcome assessors were blinded to intervention group status.
Intervention group
Intervention group participants were invited to join a twice-weekly group-based exergame program over an 8-week period, 11 with sessions lasting ∼35 minutes. The frequency and duration of exercise classes concurs with exercise recommendations for older adults in LTC. 3 The exergame sessions were in addition to any other physical activity sessions participants normally attended. Usual physical activities were generally nonweight-bearing low intensity activities (Table 1). Attendance was voluntary, although participants were invited to attend each session. Group size in each facility ranged from six to eight participants.
CG, control group; IG, intervention group.
We used Xbox Kinect® (Microsoft Corp., Redmond, WA) with the fitness package “Your Shape Fitness Evolved, 2012 Aging with Grace.” We chose this exercise package because it included simple lower and upper limb exercises that an older person could follow, and because we could use the exercises in a group format. The exergame program was supervised to ensure the safety of participants. We used a group format because supervision of individual sessions would be time and cost prohibitive.
A physical therapist or qualified exercise science instructor trained in delivering the exergame program supervised all exergame sessions. Residents were positioned so they could see the monitor. The instructor, identified by the Kinect sensor, stood at the back of the class. This meant that residents focused on the avatar rather than the instructor, copied the avatar's movements and listened to the feedback. Lower limb exercises included side and forward stepping, knee lifts, half squats, and squat punches. Upper limb exercises included shoulder forward arm raises, abduction, squat punches, and cross punches. Hand-held weights (0.5–1 kg) were added to upper limb activities when deemed appropriate. The instructor encouraged participants to undertake the exercises while standing. The number of repetitions were progressed each session, depending on individual resident's abilities. If a participant was tired or showed discomfort the instructor would adapt the onscreen exercise for that individual, for example, reduce the pace, reduce the number of repetitions, or complete the exercise set seated.
Control group
Control group residents continued their usual activities, including participation in any physical activity sessions that they would normally attend. These were generally nonweight-bearing low intensity activities (Table 1).
Measurements
The primary outcome for the trial was change in the de Morton Mobility Index (DEMMI) score over time. The DEMMI entails observation of 15 mobility tasks, scored using a 100 point scale. 19 A higher score indicates better performance. The timed up-and-go (TUG) was investigated as a secondary outcome measure. 20 Both measures were assessed at baseline and at 8 weeks using the established protocols. Cognitive status was assessed at baseline using the abbreviated mental test score (AMTS). The AMTS is a set of 10 questions. A score of six or less suggests dementia.21,22 The same rater assessed all measures.
Participants' physical activity was measured using a body-worn sensor (Dynaport MoveMonitor, McRoberts, The Hague), which has been validated for use in people aged 80 years and over. 23 Physical activity was defined as the percentage of time spent upright (in ambulation or standing) over the waking day (between 10:00 a.m. and 8 p.m.), measured for 3 days at baseline (preintervention) and 8 weeks (postrandomization).
To monitor adherence and adverse events, instructors kept records of attendance at exergame sessions, reasons for nonattendance, any adverse events and exercises completed at each session.
Sample size
Sample size was calculated using data published for the primary outcome variable, the DEMMI. 24 To show a clinically relevant change of 10 points in the DEMMI, we required a sample size of 36 participants (80% power, 0.05 alpha) in each group. When adjusted for the design effect of a clustered sample, using an estimated intra-class correlation of 0.02, 41 participants were required in each group.
Statistical analysis
Descriptive analyses were carried out using chi-squared statistics for categorical variables. The Mann–Whitney rank sum statistics was applied to describe continuous variables, as the covariates did not fit a normal distribution. Distributions were the same between intervention and control groups. Linear mixed effects models were developed to evaluate the effects of the exergame training on mobility. This approach was used to account for the cluster design using multiple sites and repeated measures. 25 Unstructured covariance was applied for facility-level random effects. Random intercept was applied at the individual level. Results are reported using restricted maximum likelihood. A combination of Stata (College Park, TX) and Statistical Package for the Social Sciences (SPSS) v. 24 (IBM SPSS Statistics; IBM Corporation, Chicago, IL) was used to carry out analyses.
Results
Based on low dependency LTC facility occupancy rates at the time of the trial, 42% of residents (n = 87) were identified by staff as appropriate for the trial. The final study population consisted of 65 residents after excluding 22 residents (Fig. 1). Baseline characteristics were similar for both groups (Table 2).
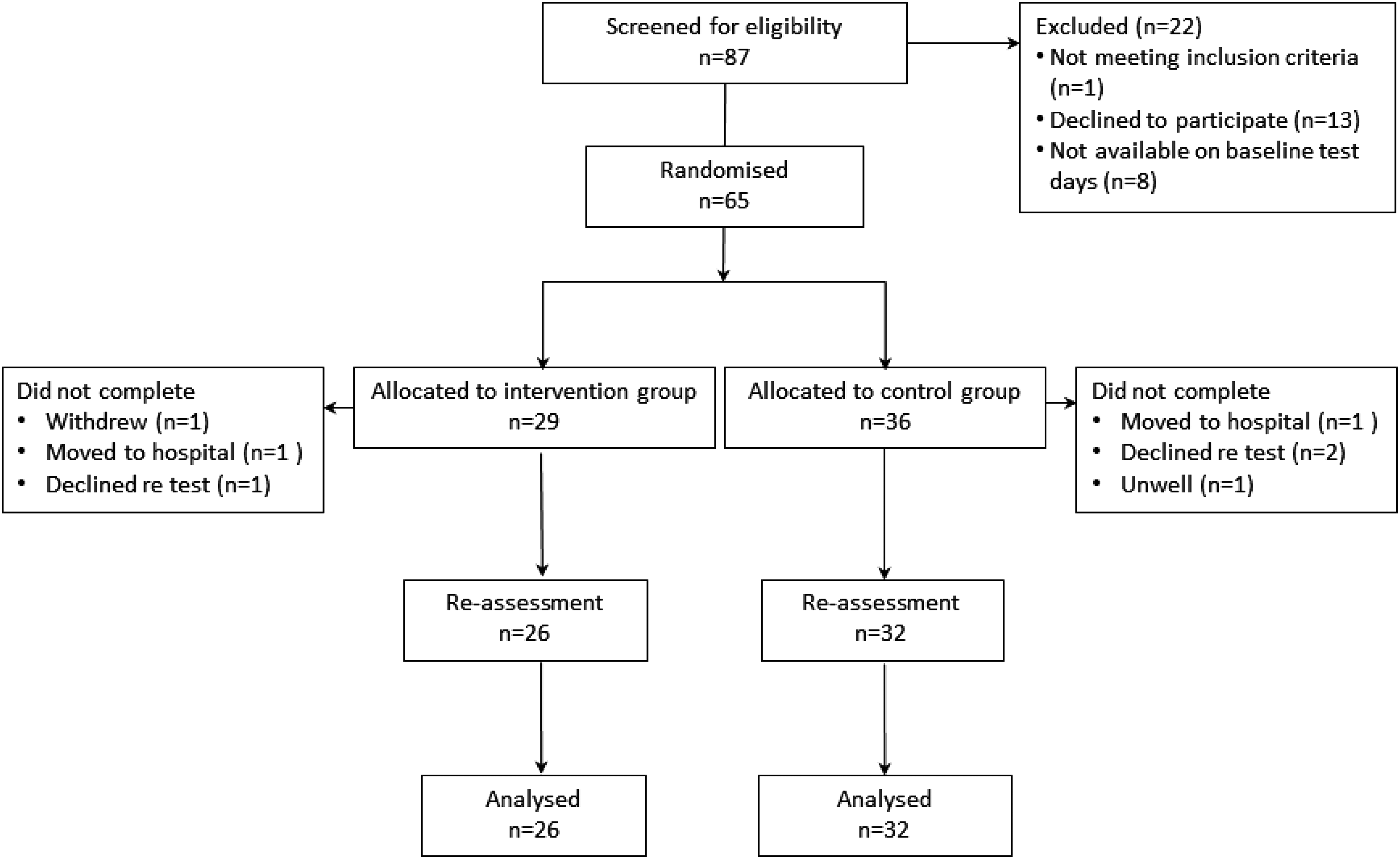
Flow of trial participants.
Values are displayed as group medians with interquartile ranges (q1; q3).
The AMTS was not completed in one intervention group participant who had English as a second language.
The TUG was not completed at baseline in one intervention group participant who was unwell at baseline testing.
Physical activity (time spent in ambulation or standing) is presented for participants who wore a sensor at baseline and at 8 weeks.
AMTS, abbreviated mental test score; DEMMI, de Morton Mobility Index; DF, degrees of freedom; s, seconds; TUG, timed up-and-go.
Table 3 shows the effect of the exergame intervention, age, gender, and cognition on DEMMI scores. There was a trend toward improvement in DEMMI scores in the intervention group (P = 0.06). Cognition was not a significant predictor of DEMMI scores in either intervention or control groups (P = 0.86).
LTC, long-term care; SE, standard error.
Figure 2 shows the predicted relationship between age and DEMMI scores, for intervention and control groups. There was a significant effect of age on DEMMI scores (P = 0.04), such that older age was associated with lower DEMMI scores in both groups.
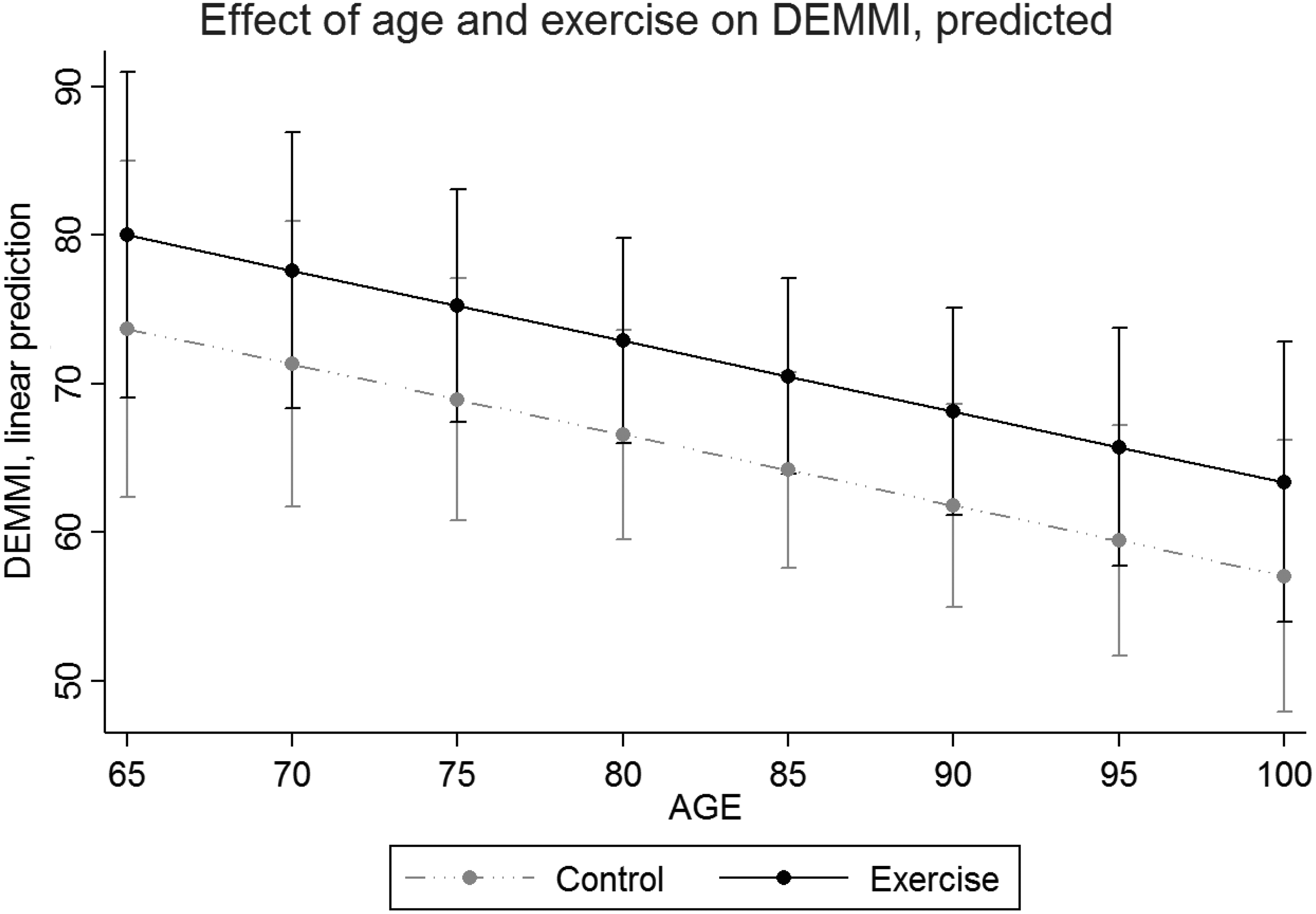
Predicted relationship between age and DEMMI scores with 95% CI. CI, confidence interval; DEMMI, de Morton Mobility Index.
No variable (exergame intervention, age, gender, and cognition) was a significant predictor of TUG scores.
There was no significant difference between intervention and control groups in physical activity levels at baseline (Table 2) or at 8 weeks (P = 0.42). Sensor data were missing for 16 of the intervention and 10 of the control group. Reasons for missing data were because participants declined to wear the monitor (n = 14); were unable to understand its purpose sufficiently to give informed consent (n = 9); had English as a second language (n = 1); were unavailable on the days when sensors were being fitted (n = 1); or because of technical malfunction (n = 1).
Attendance and adverse events
Participants in the intervention group attended 55% of scheduled sessions (8.8 ± 5.2 out of 16 scheduled sessions). Seven (27%) participants attended 14 or more sessions, although level of attendance did not have a significant effect on DEMMI scores (P = 0.49).
Documented reasons for nonattendance were illness, including hospitalization; musculoskeletal pain; conflicting schedules, for example, visitors, hairdresser's, or doctor's appointments; feeling too tired, being asleep, simply not wanting to attend, or the resident was unable to be located by the class instructor. One participant would not engage in the sessions, citing the visuals on the screen as inappropriate. Three participants stopped attending after the first two or three sessions, citing tiredness or lack of interest.
Participants who attended the exergames reported enjoying them. The most common reason participants gave for attending was to improve their balance, or because they considered that exercise was good for them. Some participants also liked the scheduled exercise times, meaning they felt obligated to attend, versus relying solely on their own motivation to do exercise, and the benefit of not having to go outside of the facility for exercise. Those with specific neurological impairments appreciated exercising with an instructor who understood their specific needs. No adverse events were observed or reported.
Discussion
The overall aim of this study was to determine whether a group-based exergame program could improve mobility in LTC residents with and without cognitive impairment. This is the first study to examine a group-based exergame program using off-the-shelf exergames in LTC facilities, which has included residents with cognitive impairment. It therefore provides results of real world exergames training in an LTC environment.
Mobility scores improved in the exergames group, although this did not reach significance. Of note, resident's cognitive impairment did not influence the mobility outcomes. Attendance at exergames sessions was good for a proportion of participants, which may be reason enough to consider them as part of an activity program for LTC residents.
Potential reasons for the lack of measurable improvement in exergames group may have been that the frequency or intensity of sessions was insufficient to effect change. We chose to offer the exergames twice weekly because it was considered feasible within the LTC facilities' schedules and sustainable for residents. Previous research indicates that once a week is insufficient, but three times weekly is too difficult for LTC residents. 7 In terms of intensity, exergames have been quantified as equivalent to light intensity energy expenditure in community-dwelling older people. 10 In LTC residents, who are older and frailer, it is likely that the energy cost of performing equivalent tasks would in fact be higher. 26 Certainly, participant feedback indicated that the exergames sessions were more strenuous than other classes they had attended. On this basis, we believe the frequency and intensity of exergames was appropriate.
Attendance rates at exergames sessions were comparable to trials of other exercise programs in LTC facilities. These studies reported adherence rates of 42%–56%.4,6 Low adherence to physical activity programs in LTC facilities is not surprising given the heterogeneity of residents' health status, along with their diversity of interests. Adherence to physical activity in LTC facilities is improved by providing a range of different activities to accommodate residents' preferences, 8 and by ensuring that motivation and pleasure are key features of the programs. 3 Since one-quarter of participants in our study attended all, or nearly all of the sessions offered, we believe these group exergames were engaging for at least some residents.
However, we identified a number of design issues that limited the applicability of exergames in LTC in their current form. First, the Xbox Kinect was designed to accommodate a single player in front of the sensor, although we ran the exergames as a group intervention. This meant individual residents were not directly interacting with the game. Group activities are more appropriate for LTC environments to enable social interaction, and because residents require supervision when exercising. For these reasons, development of exergames platforms that can interact with a group of players would be beneficial.
Second, there were very few exercises that were suitable for residents. The speed of play and the complexity of the movements narrowed the range of exercises that we could use. The complexity of the onscreen visual and auditory feedback also appeared to confuse some participants. Games need to be simplified and slowed down; for example, designing lower limb exercises without accompanying arm movements or vice versa. Using this approach, activities such as Tai Chi or dance could also be modified to suit LTC residents.
Ideally, physical therapists would prescribe and supervise exercise programs to suit the individual needs of LTC residents. However, this is not the case. LTC facility staff with little training or support usually manage the exercise programs. The potential benefit of exergames technology is that staff or family could supervise engaging appropriately designed, research-based activity programs for the residents.
There are limitations to this trial. First, we were unable to recruit the required number of LTC facilities to power the study for the primary outcome measure (the DEMMI) within the locality, and funded timeframe available for the study. The failure to recruit sufficient participants would have reduced the likelihood of detecting significant differences for exergames group. Second, we are unable to quantify the amount of activity residents might have engaged in outside of the exergame sessions, or activities the control group might have undertaken. While we documented the activities scheduled in each LTC facility, we did not record whether participants actually attended the activities. Finally, we did not control for the social interaction that instructor-led exergames would have provided. Future research might include a third arm using an instructor-led social activity program to provide a contact control.
Conclusions
Exergames did not significantly improve the mobility of LTC residents. However, attendance rates indicate that the exergames were engaging for a proportion of residents. On this basis, development of exergames designed specifically for older people living in LTC warrants further investigation and development.
Footnotes
Author Disclosure Statement
No competing financial interests exist.