
Abstract
Objectives:
To evaluate the efficacy of the “GiochiAMO” prevention program on modifying children's knowledge and belief regarding the use and abuse of alcohol and tobacco smoking.
Materials and Methods:
“GiochiAMO” is a multicomponent single-arm field trial based on card and board games to teach and enhance knowledge about risk factors related to smoking and alcohol consumption. A structured questionnaire was administered before and after the intervention to assess any change in knowledge.
Results:
A total of 167 students between 9 and 11 years of age took part in the intervention. Data concerning knowledge about cigarette smoking showed a statistically significant improvement (P = 0.008) with an increase of the mean scores from 5.93 (standard deviation [SD] = 2.05) to 7.90 (SD = 2.03). The scores related to the life skills of the intervention performed in the fourth grade classes demonstrated statistically significant improvements (P = 0.027). The scores related to the knowledge about alcohol consumption highlighted a statistically significant improvement (P < 0.001), with mean scores that rose from 7.44 (SD = 1.99) to 9.41 (SD = 1.94). The scores related to the life skills of the intervention performed in the fifth grade classes demonstrated improvements, although they were not statistically significant (P = 0.770).
Conclusions:
“GiochiAMO” demonstrated significantly improved knowledge about the risk and consequences of cigarette smoking and alcohol consumption on health. Longer follow-up studies, including a larger sample size, will be needed.
Introduction
The World Health Organization estimated that each year harmful use of alcohol causes 3 million deceases worldwide, reaching the percentage of 5.3% of total deaths. 1 The European region shows the highest rates of drinking in the world with over one-fifth of the population above 14 years of age reporting episodic alcohol drinking at least once a week. Heavy episodic drinking is widespread across all ages, although higher values concern young individuals and northern Europe countries. 2 Moreover, risk drinking habits among young people are associated with an increased likelihood of accidents and violent behaviors.3–10
In Italy, data from the National Institute of Statistics (ISTAT) showed an increase in the consumption of alcoholic beverages among subjects over 10 years of age from 65.4% in 2017 to 66.8% in 2018. However, the percentage of those who indicated to drink alcohol occasionally increased from 40.6% to 46.2%, in 2018. The rate of daily consumers declined in 10 years from 27.4% in 2008 to 20.6% in 2018. 11 The Health Behavior in School-aged Children (HBSC) survey performed in 2013–2014 revealed that 3% of the Italian girls and 7% of the Italian boys 11 years of age drink at least once a week, while the prevalence in 13 turns 8% in girls and 13% in boys. 12
Data concerning smoking habit are also alarming. It has been proved that smoking is associated with an increased risk for cardiovascular and tumoral diseases, and this hazard is increased for those smokers (90%) that started smoking tobacco before 18 years of age.13,14 Although tobacco use among adolescents has substantially declined in the last 40 years, in the United States of America alone, about 4.9 million middle and high school students declared to be current tobacco users in 2018. 15 These resulting numbers aligned with the Italian context, where the prevalence of adolescent smoking (20%) exceeds the European average (14%). 16
School is considered an important setting for smoking and alcohol prevention programs, but still, most of the interventions are delivered in a secondary school setting. 17 Interventions aimed at primary schools are less described in literature.18–20 It is common belief that the issue of alcohol and smoking should be prerogative of adolescents; however, a systematic review conducted in 2017, found out that children from a very young age are already aware and able to recognize alcohol, and prove some knowledge about its effects, so suggesting that it could be important to start prevention as early as possible. 21
During childhood and adolescence, games could be an effective educational tool to teach about the health risk and consequences of alcohol and cigarette smoking. Previous studies among children have shown that the use of game can be a useful teaching support.22,23 Furthermore, pedagogues, such as Piaget and Frobel, recognize the game during childhood as a useful tool that stimulates creativity, sociality, and intellectual development, and that could assume a pedagogical and educational value.24,25
“GiochiAMO” is a prevention project delivered in primary schools that combines educational lessons and gaming sessions concerning nutrition, physical activity, as well as smoking and drinking-related health risks and consequences. The intervention also includes a section based on a comprehensive social influence approach. 26 The intervention had been pilot tested in 2016–2017, and results suggest a significant increase in knowledge about the treated themes in the enrolled children.27–29 The aim of this study was to evaluate the efficacy of “GiochiAMO” in improving children's knowledge and attitudes, regarding the use and abuse of alcohol and tobacco.
Materials and Methods
Study design
To assess the efficacy of GiochiAMO, a single arm trial with one preintervention assessment and postintervention assessments was employed. Enrollment took place in November 2017 and baseline assessment took place in December 2017 and January 2018. The postintervention assessment took place between April 2018 and June 2018. All procedures used in the study were in accordance with the Declaration of Helsinki's principles. Anonymity was always guaranteed.
Setting and participants
The school, a primary school in Rome (Italy), was selected based on convenience. Eligible participants were primary school students between 9 and 11 years of age, attending the fourth (classes: A, B, C, D, E) and fifth grade (classes: A, B, C, D). Before the beginning of the trial, parents and teacher were informed about the purpose, structure, and ethical implications of the study. All participating children provided written informed assent and their legal guardians provided written informed consent. Children without a signed informed consent form on the day of the intervention were excluded.
Inclusion criteria
Children were enrolled in the program if they satisfied the following inclusion criteria: belong to the fourth or fifth grade of Fratelli Bandiera primary school; signed informed consent by the parents; and compliance of the responder to the questionnaire with ability to judge. Children were excluded from the study if they did not satisfy at least one of the above inclusion criteria.
Intervention
GiochiAMO (i.e., “Let's Play”) is a multicomponent school-based intervention that includes educational seminars as well as interactive games to promote healthy nutrition and physical activity and to prevent smoking and alcohol abuse among elementary school students. The present study reports the results of the smoking and alcohol component. GiochiAMO was developed by the Department of Public Health and Infectious Diseases at the Sapienza University of Rome (Italy). The project teaches risks and consequences to health related to alcohol consumption and cigarette smoking and aims to provide children with basic life skills competencies to effectively counteract social pressure.28,29 The ultimate goal is to motivate children to integrate healthy lifestyle choices into their everyday life. The interventions are structured in a knowledge-based education session and gaming sessions. Once a week, students were invited to take part in 30–45 minutes long game sessions, in class, over a period of 20 weeks.
Oral presentation
The oral presentation lasted 1 hour and was performed by medical doctors from the Department of Public Health and Infectious Diseases. It was designed with an endearing format for a children's audience and it focused on risks and consequences of these unhealthy habits: alcohol issue was treated focusing on health effects (e.g., irreversible brain impairment or liver damage), and on risky behaviors associated with its consumption (e.g., driving after drinking); the smoking issue was dealt with an overview on the topic of addiction, smoking-related pathologies, and on the environmental pollution. Children were stimulated to an active participation, by questions and comments.
Games
The game sessions were coordinated by teachers, lasted about 60 minutes each, and were delivered within the classrooms. Children were grouped in small units (six to eight persons each) to obtain full participation to the activities. A total of six games (board and card games) was proposed. The games stressed the issues related to alcohol consumption and cigarette smoking. In addition to the games, children were invited to participate in role plays, which focused on increasing their consciousness about social pressure and with the aim of strengthening their life skills, such problem solving. During these activities, teachers provided children with winning behavior models and incited them to create new ones to be shared. A typical game session requires two to four players and lasts about 30–45 minutes.
Board games
“The Game of the Drunk Goose” and “The Game of the Smoked Goose” are two board games designed by the research group inspired by the classic Goose game that can be played by up to eight people at a time. The game kit was composed of one play board, pieces, and gaming dices. A typical game session lasted about 30–45 minutes. Many boxes had special hazards or benefits for players passing by them. During the game, players had to answer questions about smoke and alcohol to move their pieces along the game board path. Wrong answers were connected to penances, physical exercises, or tongue twisters.
Card games
A deck of 40 cards was designed by the research group, identifying with different colors positive or negative meanings and health effects (Supplemementary Figure S1). Defining the rules, it was taken inspiration from traditional Italian card games, such as “Saltacavallo” and “Tappo.” The content was readapted and specifically structured to relate positive messages to winning strategies.
Group games
Role-playing games and group activities were ideated with the aim of stimulating social interaction among children while reinforcing life skill models and knowledge messages.
Questionnaires and outcomes
With the objective to evaluate differences of knowledge before and after the intervention, the children were asked to fill in the same questionnaire at the beginning and at the end of the study. Pre- and postintervention answers were paired by assigning an alphanumeric code to each child. Demographic data (sex and age) were collected from all the involved children. Moreover, students belonging to the fourth grade were administered with a questionnaire about cigarette smoke consisting of 18 multiresponse questions (11 questions concerning cigarette smoke and 7 questions concerning life skills) and one question investigating the smoking status of their parents (both parents were smokers; one parent was smoker; neither was smoker). On the other hand, fifth-grade students, filled in a questionnaire about alcohol consumption consisting of 17 multiple choice questions (11 concerning alcohol and 6 concerning life skills). Each question had a single correct answer that was rated with one point; wrong or unanswered questions were evaluated with zero points.
To perform the statistical analysis and compare results gained by the students, a structured scoring system was applied. Four scores were calculated:
Smoking Score (Sc_Smoke), as sum of the points gained answering correctly to smoking questions; Alcohol Score (Sc_Alcohol), as sum of the points gained answering correctly to alcohol questions; Life skills Score (Sc_Lifeskills), calculated both for the smoke and alcohol intervention, as sum of the points gained answering correctly to life skills questions.
Each score was itemized with T0, when referred to baseline results and to T1, if referred to postintervention results. Then, the difference between T1 scores and the related T0 scores was calculated and named as Delta score, so to detect changes in time:
Delta smoking score (Delta_Sc_Smoke), as difference between ScSmokeT1 and ScSmokeT0;
Delta alcohol score (Delta_Sc_Alcohol), as difference between ScAlcoholT1 and ScAlcoholT0;
Delta life skills score (Delta_Sc_Lifeskills), as difference between ScLifeskillsT1 and ScLifeskillsT0.
Statistical analysis
The statistical analysis was performed using IBM SPSS (Statistical Package for Social Sciences) version 25. A descriptive analysis of the demographic data was performed to describe the characteristics of the sample population (gender, age, parents' smoking status). Moreover, a univariate statistical analysis was carried out using the Wilcoxon test to evaluate the presence of statistically significant differences between the baseline and the postintervention scores. Finally, a linear regression was performed using a backward stepwise process of elimination of nonsignificant variables generating a minimal model. The following variables were included in the model: sex, age, class, and parents' smoking status (classified as smokers vs. nonsmokers). The level of significance of all the performed analysis was set at P < 0.05.
Results
During 2017–2018 school year, 167 children participated in the activities of “GiochiAMO” intervention. No dropouts were recorded. Two different interventions have been implemented: one concerning cigarette smoking (fourth grade primary school classes) and one regarding alcohol consumption (fifth grade primary school classes). Table 1 shows the sociodemographic characteristics of the population for each intervention group.
Descriptive Analysis of Sociodemographic Characteristics of the Population
Sample characteristics of the intervention against cigarette smoking
A total of 99 fourth grade primary school students, with a mean age of 9.01 years (SD = 0.39), participated in the intervention against smoking (Table 1). Genders were equally distributed. One student did not indicate sex (1%).
Sample characteristics of the intervention against alcohol consumption
A total of 68 fifth grade primary school students participated in the intervention against alcohol consumption. The sample included 40 males (59%) and 28 females (41%) with a mean age of 10.2 years (SD = 0.36).
A descriptive analysis of parents' smoking status before and after the intervention was performed (Table 2). The number of children declaring both parents as smokers decreased from 12 to 10. At the beginning of the intervention only three children indicated that only their mother smokes, while after the intervention, this number rose to five students who indicated that only their mother smokes. The number of children who reported that only the father smokes changed from 10 to 11. The number of children with none of the parents as smokers moved from 73 to 70. One missing was detected at T0 investigation; three missing were detected at T1 investigation. Table 2 shows results from the parents' smoking status descriptive analysis.
Descriptive Analysis of Parents' Smoking Status
Alcohol consumption related knowledge
Figure 1 and Figure 2 show variations in knowledge and life skill scores within the alcohol intervention group before and after the intervention.
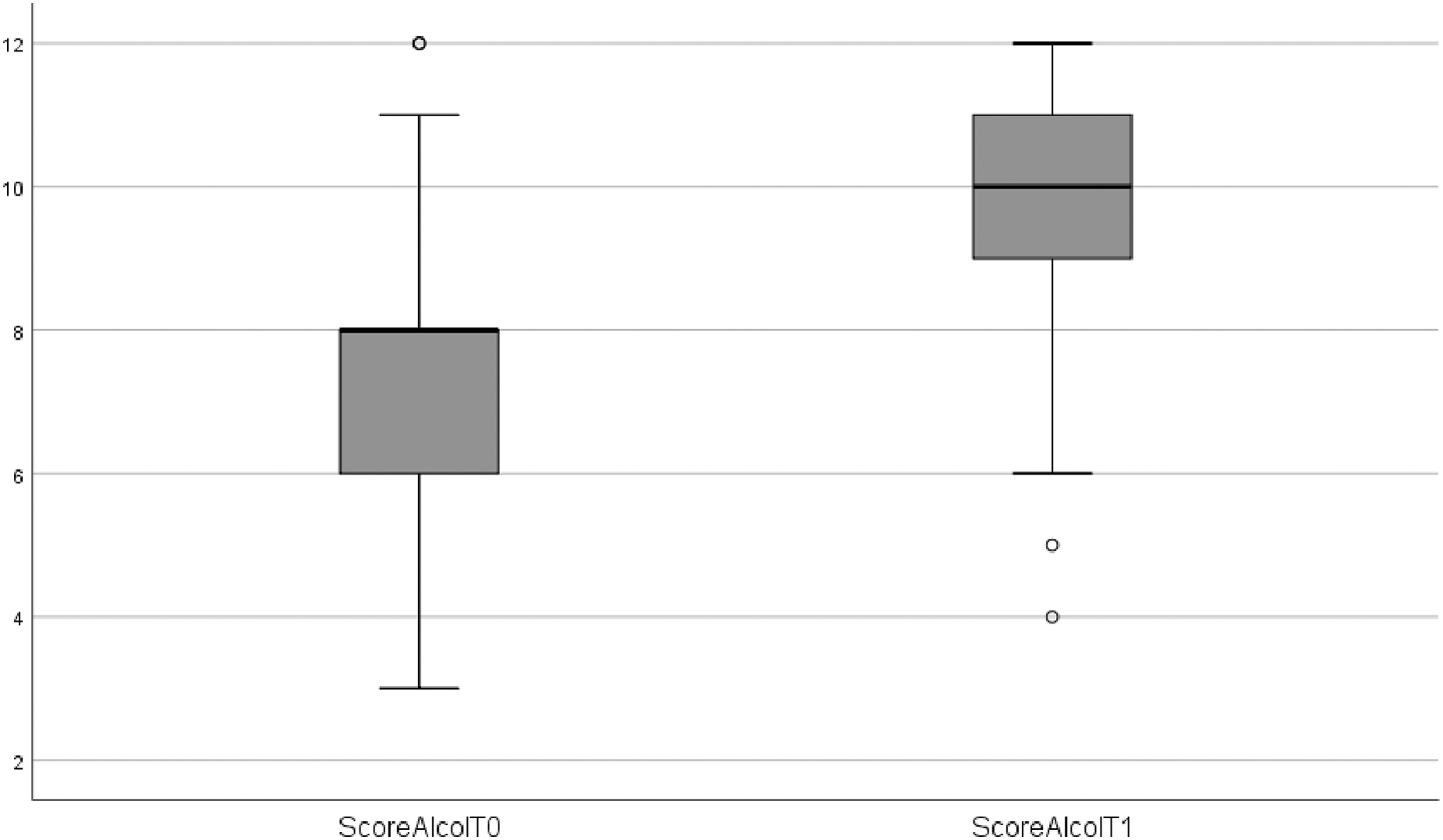
Box plot exploring variations in knowledge within the alcohol intervention group. ScoreAcolT0 = alcohol knowledge score at baseline assessment/preintervention assessment; ScoreAcolT1 = alcohol knowledge score at postintervention assessment.
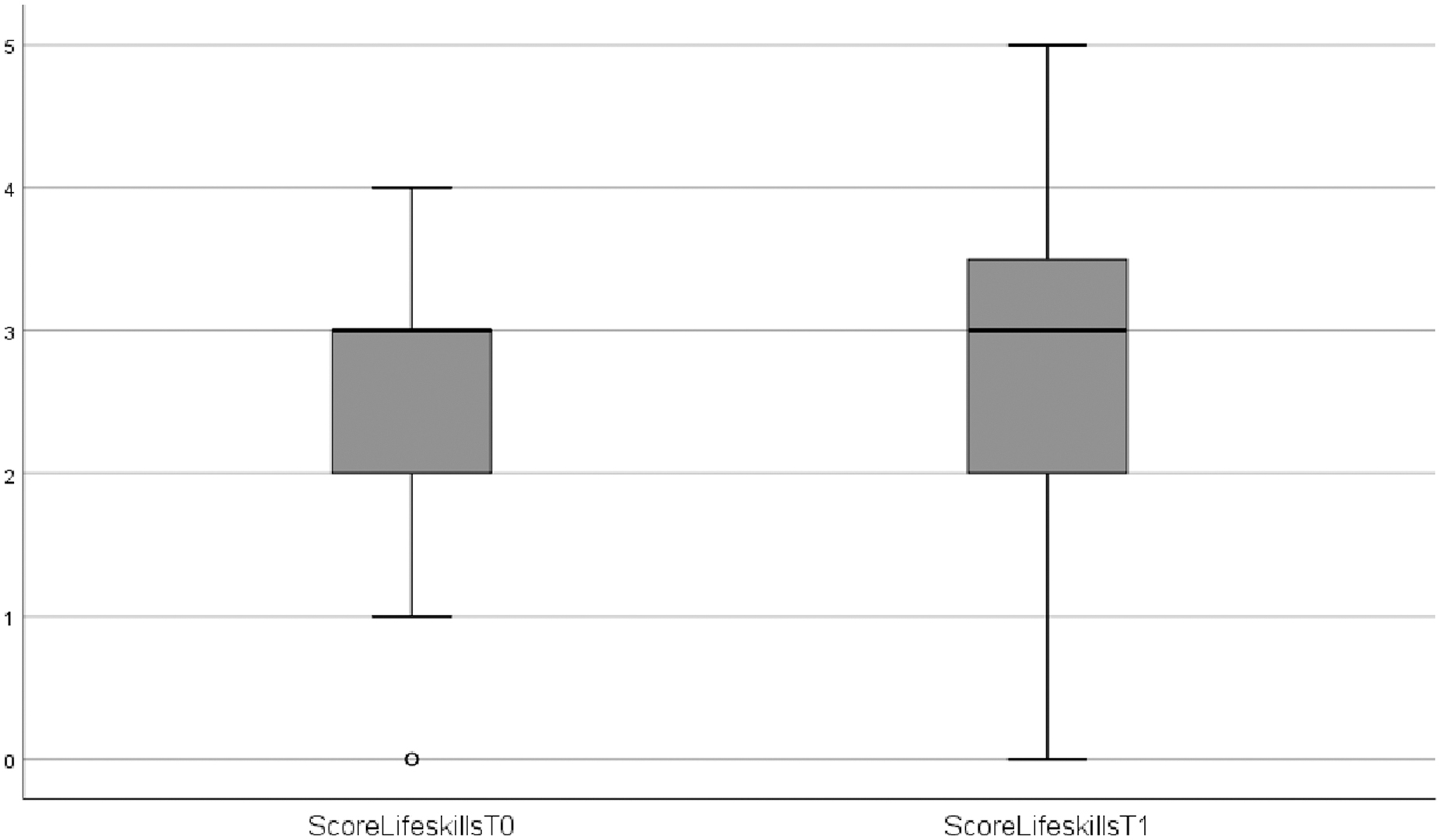
Box plot exploring variations in life skills within the alcohol intervention group. ScoreLifeskillsT0 = life skill score at baseline assessment/preintervention assessment in the alcohol intervention group; ScoreLifeskillsT1 = life skill score at postintervention assessment in the alcohol intervention group.
The results of the univariate analysis, concerning the alcohol interventions, show an improvement in all the records, except for the scores about life skills that have been registered in the fifth-grade classes. The scores related to the knowledge about alcohol consumption highlighted a statistically significant improvement (P < 0.001): the mean scores rose from 7.44 (SD = 1.99) to 9.41 (SD = 1.94); the median values passed from 7 (min = 4; max = 12) to 9 (min = 6; max = 12). The scores related to the life skills of the intervention performed in the fifth grade classes demonstrated reduction of the mean values that passed from 2.67 (SD = 1.07) to 2.63 (SD = 1.24); the median values remained unchanged at the value of 3 (min = 0 and max = 4 at T0; min = 0 and max = 5 at T1). However, it is important to highlight that these differences did not result statistically significant (P = 0.770).
Cigarette smoking-related knowledge
Table 3 shows the results for the intervention against cigarette smoking similar to the results of the intervention against alcohol consumption, smoking knowledge-related scores significantly improved (P = 0.008) after the intervention. Students had a mean score gain from 5.93 (SD = 2.05) to 7.90 (SD = 2.03); the median values passed from 6 (min = 0; max = 10) to 8 (min = 0; max = 11) (Fig. 3).
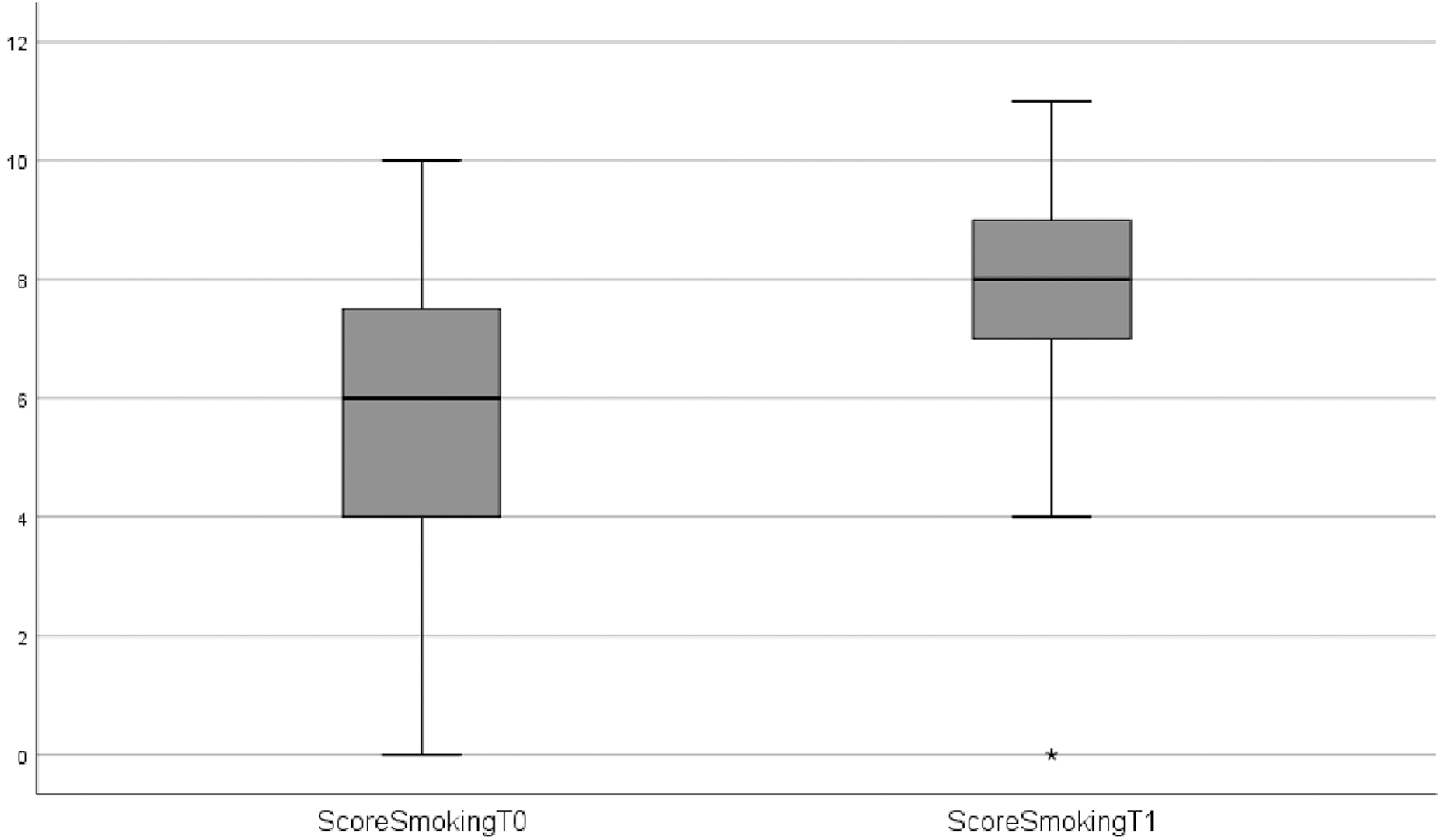
Box plot exploring variations in knowledge scores within the smoking intervention group. ScoreSmokingT0 = smoking knowledge score at baseline assessment/preintervention assessment; ScoreSmokingT1 = smoking knowledge score at postintervention assessment.
Univariate Analysis Using Wilcoxon Test
Wilcoxon test. Bold characters highlight statistically significant results.
SD, standard deviation.
The scores related to the life skills of the intervention performed in the fourth grade classes demonstrated statistically significant improvement (P = 0.027): the mean scores arose from 2.39 (SD = 1.30) to 2.81 (SD = 1.15); the median values passed from 2 (min = 0; max = 5) to 3 (min = 0; max = 5) (Fig. 4).
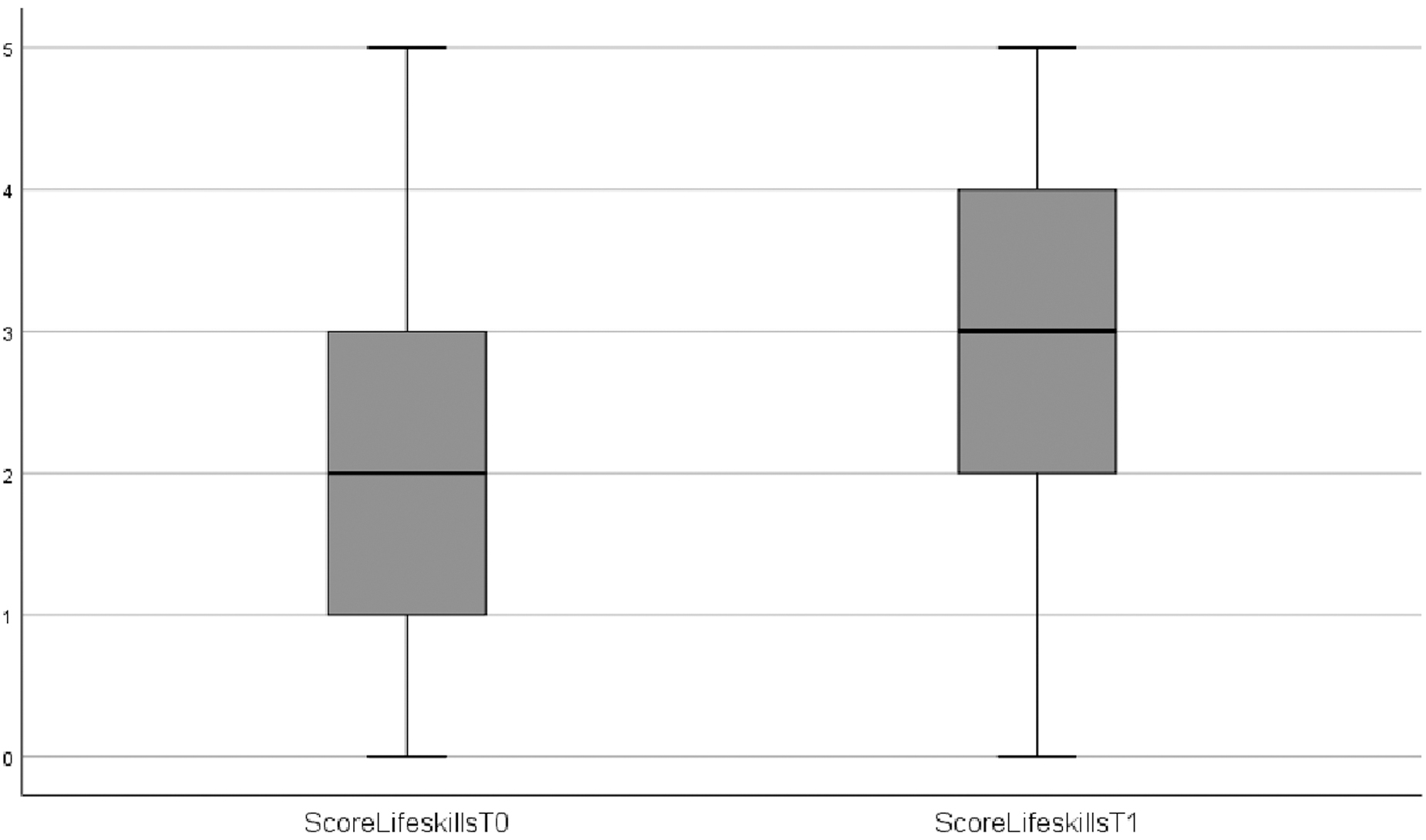
Box plot exploring variations in life skill scores within the smoking intervention group. ScoreLifeskillsT0 = life skill score at baseline assessment/preintervention assessment in the smoking intervention group; ScoreLifeskillsT1 = life skill score at postintervention assessment smoking intervention group.
The following variables were included in the linear regression model: sex, age, class, and parents' smoking status (classified in smokers vs. nonsmokers). The regression model evaluated whether these factors could interfere with the increase of knowledge within the sample population (Delta_Sc_Smoke). Results from the analysis show that children enrolled in class D and class E have significantly different scores if compared with others, whereas other variables do not influence the efficacy of the intervention.
A multivariate analysis with alcohol delta score (Delta_Sc_Alcohol) as dependent variable was conducted. Independent variables were: sex, age, and classes (B, C, D). Class A was taken as the reference group. The results show that only age was positively correlated with delta score (R 2 = 0.091; β = 0.302; P = 0.012).
Discussion
This study showed that “GiochiAMO” increased the knowledge about the risk and consequences of alcohol consumption and cigarette smoking among children 9–11 years of age. Furthermore, it proves the efficacy of combining the oral presentation with game sessions to deliver the contents.
These results are in line with previous scientific evidence that has shown a significant effect of interventions to prevent health risk behaviors targeted at an adolescent population. “Unplugged” for example, has been recognized in the European context as one of the most effective projects for alcohol and drug abuse prevention, but it was delivered to individuals between 12 and 14 years of age.17,30–32 Likewise, improvements in knowledge were observed in the “Wise Mind Study”: a school-based alcohol, tobacco, and drug prevention program delivered to adolescents. 33 However, it has been recognized the importance of an early delivery of the information, already during childhood, focusing on the risky consequences of these habits. Indeed, it has been observed that intervening at this stage, predicts a delay for the alcohol initiation, and results in later alcohol misuse and smoking addiction.21,34–40 In the light of the encouraging results previously obtained from two pilot studies performed in 2016 and 2017,28,29 this research demonstrated the efficacy of “GiochiAMO” intervention, to increase the level of knowledge concerning smoking and alcohol in a sample population of children.
Strengths and limitations
The study contains some limitation that must be acknowledged. First, the main limitation concerns the study design. We employed a single-arm trial, which does not allow to make comparisons to a control group. Second, the intervention has been tested only in one school, and the sample size is relatively small compared with similar interventions.9,10 The measurement was performed using a questionnaire that was not validated and took place twice within one school year. This might be early for detecting changes in behavior. Longitudinal research involving a larger sample size is needed to evaluate the effectiveness of GiochiAMO. Third, the data were self-reported; therefore, another limitation concerns the truthfulness of answers, and possible risks of biases, such as information and recall bias. Fourth, no other social or contextual factors such as family socioeconomic status (SES) that could have interfered with results, have been investigated. Researchers, for example, found that parental education, an indicator of family SES, was significantly and inversely associated with adolescent smoking status. Similar results were also detected for the association between household income and adolescent smoking. 41 Furthermore, external factors such as education about the risks of cigarette smoking from parents at home could have possibly biased our results.
Strengths of this study are represented by the innovative design of the intervention. Indeed, the education was delivered exploiting the power of games that was previously demonstrated by scientific literature. It has been proven that games can trigger students' learning motivation and enhance prosocial behaviors, increasing attention and helping in the emotion management.42,43 Some games focus on the ability to refuse health risk behaviors and face social pressure from peers. Overall, interventions using games represent a strong innovation and a useful tool to communicate with children about health-related information.22,28,29,44–47 The use of games as an education tool makes learning interactive and allows an active acquisition instead of the passive listening of a lesson.
Conclusions
“GiochiAMO” significantly improved knowledge about the risk and consequences on health of cigarette smoking and alcohol consumption. While longer follow-up studies, including a larger sample size, are needed, these data suggest substantial potentialities. “GiochiAMO” features an innovative project that may be used as an effective tool in childhood alcohol and prevention programs.
Footnotes
Acknowledgments
The authors would like to thank the director and teachers from Fratelli Bandiera primary school who helped in the implementation of the intervention and thank Tony Yordanov for his support.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.