
Abstract
Background:
Innovative methods for smoking prevention interventions need to be investigated to increase attractiveness, access hard-to-reach populations, and increase effectiveness. We studied the feasibility and immediate effects of an intervention to reinforce norms and behaviors of young people related to antismoking, integrated into a popular online community game.
Methods:
A pilot randomized controlled trial was conducted through the HABBO online community. The intervention group was exposed to repeated discussion sessions with small groups of peer players and two facilitators once a week for 1 month (four sessions), inside the game. The control group had access to antismoking information websites. Process indicators (attractiveness, participation) and immediate outcomes (norms and intentions with regard to smoking) were assessed by questionnaire.
Results:
One hundred sixteen players were invited to participate in the intervention; 10 did not meet eligibility criteria, 30 were allocated to the intervention group, and 76 to the control group. Median age was 23. Twenty-four percent were not in education, employment, or training. A median of eight players attended each session and the median number of exchange chats by session was 399; 70% of chat time was occupied by the players. Twenty players attended all four sessions. Immediate norms, representations, and intentions were evaluated in 39 players and showed small differences between groups.
Conclusion:
Delivering and evaluating a smoking prevention intervention in an online game is feasible. In the targeted online community game, the intervention was attractive and allowed the delivery of innovative interventions to audiences with diverse social profiles. Long-term effects, sustainability, and evaluation methodology are discussed.
Introduction
Adolescent smoking is predictive of tobacco consumption—the world's leading cause of avoidable premature mortality 1 —in adult life.2,3 Thus, adolescence appears to be a key period for the prevention of this behavior and its consequences in terms of morbidities and mortality. In Europe, in 2014, 17.5% of 15–24-year-old males (24.3% in France) and 13.5% of 15–24-year-old women (20.1% in France) were daily smokers of cigarettes. 4 Although in France, the prevalence of daily smoking among 17-year-olds fell from 38% to 25% between 2003 and 2017, there are still prevention efforts to be made: on the one hand because the prevalence remains high, on the other hand because the smoking according to the advantaged/disadvantaged social gradient remains very clearly marked in youth (20.0% and 28%, respectively, of smoking in 2017). 5
Since few years, the tobacco industry uses marketing campaigns deployed in online social network and videogames to reach young people. 6 For it, the use of the Internet allows to adopt an innovative and youth-friendly approach, and the promotion of tobacco products is less constrained. In that respect, tobacco control strategies have to evolve on the same ground to better connect with young people for prevention. 7
In fact, adolescents and young adults are intensive Internet users. In 2019, 95% of 16–24 Europeans used the internet on a daily basis, 8 in France, in 2019, 100% of people aged 12–24 were internet users.6,9,10,11 To date, systematic reviews assessing interventions aiming to prevent adolescent smoking are heterogeneous in terms of methodology and mechanisms of action, and do not enable identification of the most effective methods. 12 Existing literature does offer some guidance for online smoking prevention. Regarding intervention modalities, peer coaching has been shown to be superior to messages delivered by a technological avatar (programs, robots, or “bots”), in particular to reduce smoking among young smokers. 13 Notably, few existing online programs allow discussion with individuals in target groups. 14 Finally, to access “ hard-to-reach ” populations, web-based interventions should be equipped to make them adolescent friendly. 15 This is why we chose to implement our prevention action through a favorite entertainment of the young people, a videogame. 16
Public health professionals have created their avatar in a popular videogame with social networking component, bringing together thousands of players, and offered weekly 100% virtual group discussions for a month. This implementation of action into an existing entertainment videogame is a novelty in the prevention research field.
The main objective was to study the feasibility of an innovative intervention for smoking prevention embedded in a virtual game world used by adolescents. The secondary objective was to describe the evolution under the intervention of smoking intention and smoking-related norms.
Methods
A pilot randomized controlled trial was conducted using an online community game (ClinicalTrials.gov Identifier: NCT04888208).
Site of intervention
From existing game environments, we chose HABBO, 17 a virtual world for teenagers ages 13 and older—developed by Sulake. The reasons for the choice were: (1) free user access; (2) a large French-speaking HABBO community (several thousand users); (3) HABBO inclusion of health issues (in French-speaking HABBO, a team of health psychologists Fil Santé Jeunes animates weekly focus groups); and (4) an existing security and moderation system. To play, it is necessary to create an account with an email.
HABBO is a world made up of various “rooms”. Public rooms are open to all players, and represent real public spaces, such as restaurants, cinemas, or nightclubs. Players embody avatars, virtual characters that they can customize. These can interact with other users, mainly through instant chat.
Collaboration for the study between Sulake (a company specializing in online entertainment, virtual worlds, and social networks) and the research team was initiated. As part of this research project, Sulake developed a new room in HABBO, consisting of a garden in which a bus is parked, where the intervention took place (Fig. 1). Sulake collaborates in charitable partnerships around the world to educate teenage players about a range of topics. It was not involved in the design and objectives of the study nor in the analysis of the data.
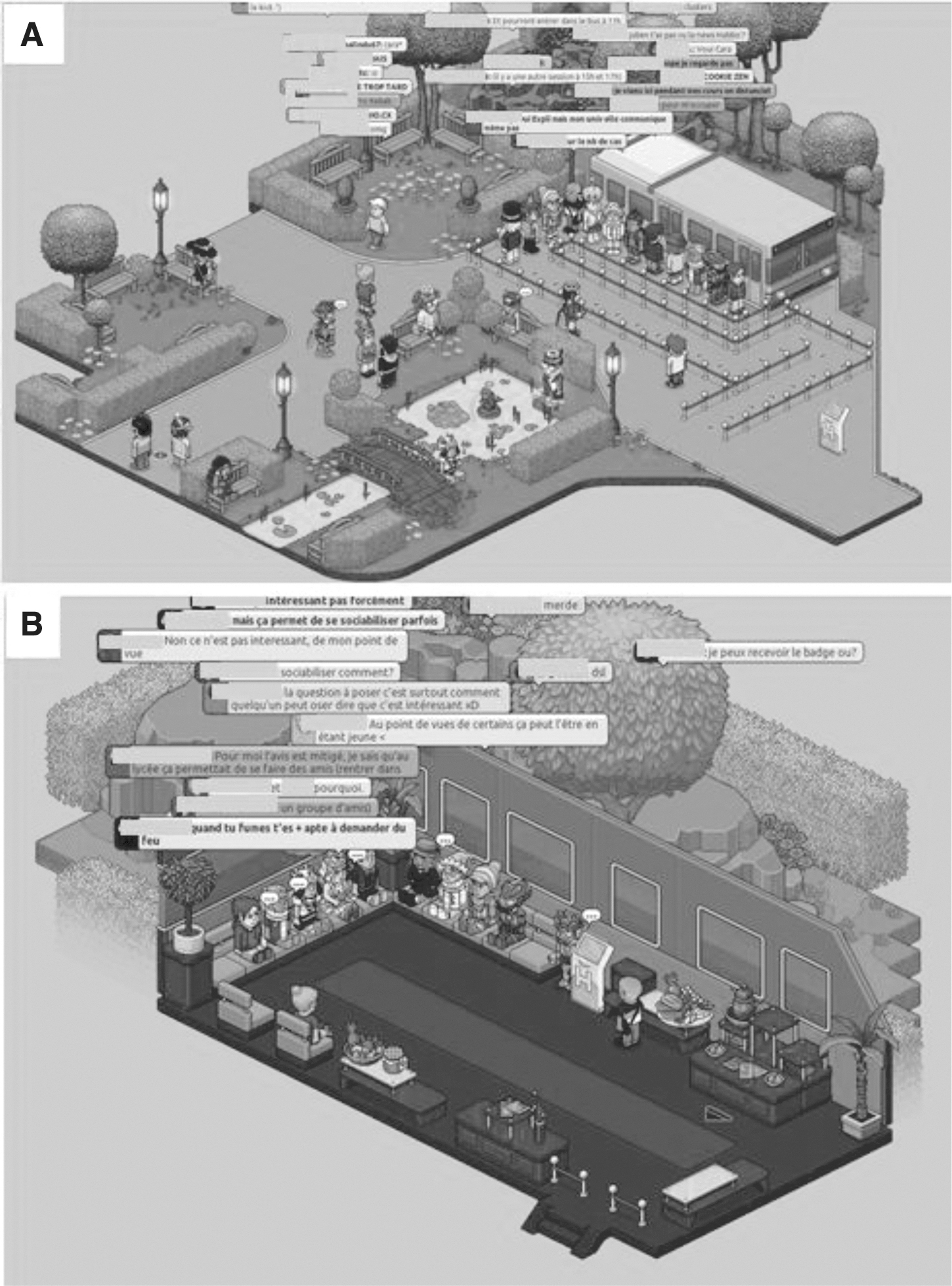
New room in HABBO dedicated to the research consisting of a garden with a kiosk information accessible to all players
Theoretical background of the intervention
To build the intervention, we analyzed the HABBO game to fully comprehend its logic and main components. Two emerged as central for our intervention: socialization as players come into the world, to make friends and converse with them; and badge collection, where badges give the players status, and some show their membership of a specific “tribe/group”. This was one of our elements of attractiveness.
The intervention was based on the theory of planned behavior, 18 whereby attitudes, subjective norms, and perceived behavioral control are seen as determinants of smoking intention. The theoretical framework also applied notions of social support, group motivation, and social learning 19 to small online groups. 20
Intervention characteristics
The intervention group had access to four 30-minute sessions at 1-week intervals (Thursdays at 11:00, 15:00, or 17:00) in groups of 10 players maximum. It included four sessions addressing: (1) reasons why youth smoke; (2) benefits of not smoking and experiences of antismoking behavior; (3) watching visual antismoking content (pictures and videos from popular international antitobacco campaigns) and discussion of impact; and (4) ways of prevention actions in the game.
A short moment of dance was organized at the end of each session, to strengthen group cohesion; and a new badge was given to players who completed the session, to enhance attractiveness. Sessions were led by two professional facilitators, doctors in public health, trained in the game. Their role was to propose topics of discussion (and possible sources of support), moderate exchanges, and relaunch the debate when it ran out of steam, to support the prevention discourse of players (antitobacco norms and attitudes) and foster social support.
Participants and recruitment
Participants were members of the French-speaking HABBO community who agreed to participate and to complete the baseline questionnaire. For minors, parents had to be not opposed to participation (Ethics section). No opposition was expressed.
An insert on the HABBO community home page was released a week before the start to promote the study.
Design of the study
The design was an online-only pilot-controlled trial with individual randomization. Recruitment took place over 1 day. Once participants were allocated to an intervention or control group, they were followed for 4 weeks (from October 1, 2020).
On the day of recruitment, the virtual garden dedicated to research opened for the first time. When a player arrived in the virtual garden, the research ethics information note was automatically submitted in a pop-up window. After having read it and consented, players could leave the room or stay to complete a baseline questionnaire (embed in the game without use of an external website). Only players who completed the baseline questionnaire were eligible for randomization. Allocation between the two groups was done by the community manager of Habbo whose avatar was present in the garden. Her role was to allocate recruits to groups at her discretion, she randomly picked lines in the players' response database, without a pre-established randomization list (no preplanned allocation ratio, no predefined rule) (Fig. 2). The community manager manages a community of several thousand players, in her work she does not befriend the players, and therefore had no prior reason to bias the allocation of players in the groups.
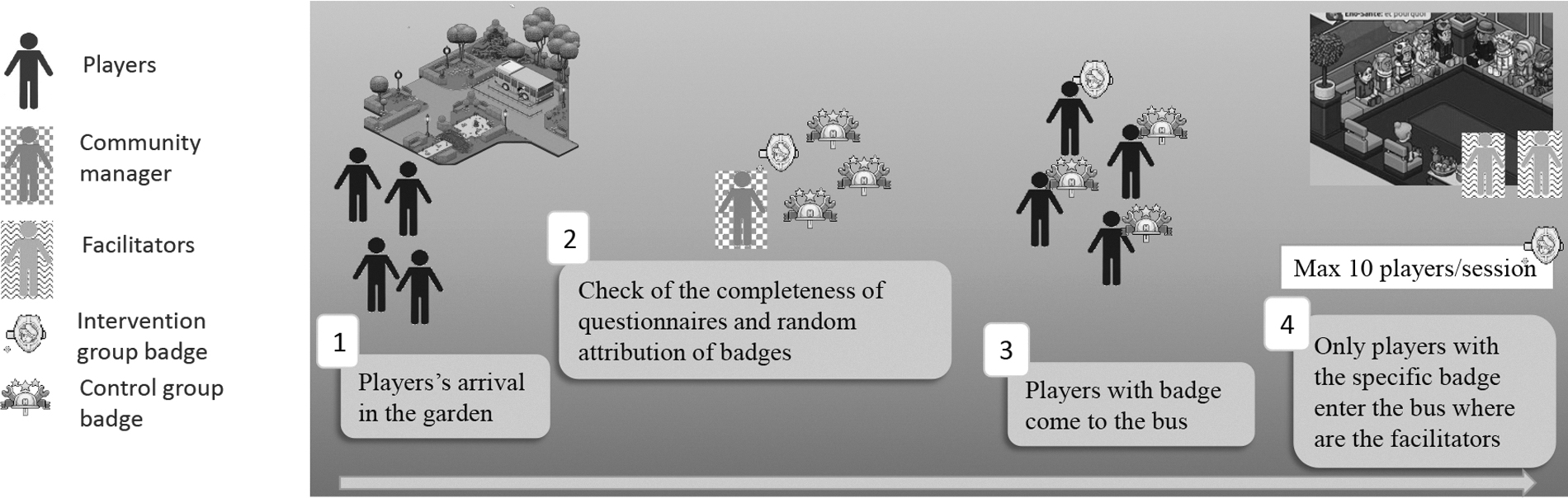
Randomization process and intervention group players' participation in the study.
The time between the collection of the questionnaires and the randomization was very fast (a few minutes) and did not allow the community manager to read the individual responses. She distributed virtual “badges” to players (for the intervention group or for the control group), independently of the answers given to the questionnaire by players, and without consulting the intervention team.
To ensure feasibility, the garden was open to a maximum of 30 players at once, 10 minutes before each time of recruitment (11:00 15:00, and 17:00). Badges were given to randomized participants. The number of patients finally included was not known in advance; we only limit the maximum of 30 specific badges giving access to the intervention (10 per recruitment times), to ensure feasibility of delivery of the intervention. The other badges allowed the players to participate as control participants in the study.
Intervention group
The game allowed for restricting access to certain areas to specific players. The place of the intervention (a virtual bus parked in the virtual garden) was made accessible only to players wearing the “intervention” badge and to facilitators.
Control group
The control group had access to the garden where there was an information kiosk providing noninteractive health and antitobacco information resources (governmental and validated nonprofit organization websites).
Data collection
Data were qualitative (verbatims from instant chat, participant observation) and quantitative (process indicators and questionnaires submitted to players). Data from questionnaire were collected by Sulake, the provider of the Internet virtual world hosting the HABBO players community. Sulake transmitted data in an anonymized form without any possibility of reidentification (the ID correspond to a series of numbers automatically generated by HABBO when creating player profiles, which does not correspond to any personal information). Completion of the same questionnaire (30 items) twice (once at baseline and again at the end of the study, at 4 weeks) was carried out directly in the game. A great virtual party at the end of the 4 weeks of the study with the players of the control and intervention groups enabled completion of final questionnaires.
Outcomes
Feasibility and process outcomes were reach (profile of participants), attraction (numbers of players present at the trial launch), and retention (numbers of participants staying in the intervention over time), participation in the program sessions (number of players, numbers of chats), player interaction with facilitators and satisfaction with the intervention, numbers of players who completed the evaluation, and number of players who used the information kiosk.
Evolution under the intervention of smoking intention and smoking-related norms were assessed through a self-questionnaire based on the Theory of Planned Behavior developed with French adolescents in real life 21 (the validation study showed a satisfactory face and content validity) and internal consistency of the “intention” dimension was excellent (n = 1573, α = 0.93) and that of the “behavioral beliefs” dimension was good (n = 1573, α = 0.74). 22
A smoking intention score was collected through three items based on a visual numeric scale and interpreted for each item with 1 the smallest and 7 the greatest intention to smoke (e.g., “I have the intention to smoke in the next month” not agree at all [rated 1]—absolutely agree [rated 7]). Attitude score was measured using two items with 1 the least and 7 the most positive attitude to tobacco (e.g., Smoking is: unpleasant [rated 1]—very pleasant [rated 7]). The behavioral belief score was measured by 14 items matched by 2 and can be interpreted as the smallest tabagism risk when the score is negative up to −21; and greatest risk when the score is positive up to +21, 0 indicating neutral behavior (e.g., “if I smoke in the next month I will be popular”: probably [rated 7] to probably not [rated 1], match with the item “being popular will be”: very positive [rated +3] to very negative [rated −3]). Questions on young people's opinions related to tobacco from a nationwide repeated cross-sectional study were added. 23
Qualitative analysis
Players' behaviors, speeches, and interactions were observed throughout the sessions. Qualitative data were transcribed at the end of each session and enriched by the feedback of facilitators. Data were anonymized, then synthesized, and analyzed by themes by the two facilitators. The use of mixed methods in the study was for complementarity, and here qualitative data were used to illustrate the results of quantitative methods. 24
Quantitative analysis
Quantitative variables are described by their median (1st quartile [Q1]–3rd quartile [Q3]) and qualitative variables by counts and percentages. Data were analyzed in participants who answered the final questionnaire (no data imputation). All statistics were calculated using SAS software © 2002-2012 by SAS Institute, Inc., Cary, NC, version 9.4 for Windows.
Sample size
No sample size was calculated for this pilot study whose primary objective was to describe feasibility. Based on game's experts, the animation and moderation of more than 10 players simultaneously is not recommended, given the rate of chat. To test different time slots and increase heterogeneity among participant profiles, while maintaining an adequate level of facilitators' concentration, we planned the animation of three groups per intervention day. Thus, the sample size expected was at least 30 players in the intervention group.
Ethics
Players could withdraw from the study and request the erasure of their data at any time on simple request (the contacts were provided in the information note). The information note remained present on virtual terminals in the game throughout the duration of the search. Regarding parents, as part of our research, underage players were asked to ensure their parents' agreement to participate (as they did for their registration on Habbo). A page dedicated to information for parents and allowing them to express their opposition to their minor adolescent participating in the research was accessible from the site connection page 15 days before the start of the study and stayed there until 15 days after the end.
Under French regulations, this type of research does not require written consent but an information and a right of opposition. The proposed circuit has been validated from an ethical and legal point of view by the competent local authorities: The Inserm Institutional Review Board (IRB00003888) gave a favorable opinion of our study and approved its procedure (July 7, 2020).
After each receipt of anonymized databases by the research team, the HABBO team deleted the research-related data from its servers. They agreed not to use it when establishing the framework for collaboration.
Results
Participant flow
On the day of recruitment (October 1, 2020), 116 players entered the virtual garden and were invited to participate in the intervention. Of these, 10 did not complete the baseline study questionnaire and were not included in the study (Fig. 3). Of the 106 badges distributed, 30 gave access to the intervention. The other badges (n = 76) allowed the participants to participate as controls in the study. The virtual garden was full at each time of recruitment (30 players present simultaneously). Participants were mainly girls, young adults (min age: 16–max age: 31), living in France (Table 1). Almost a quarter (26/106, 24%) were unemployed (not in education or training); a third were occasional or daily smokers.
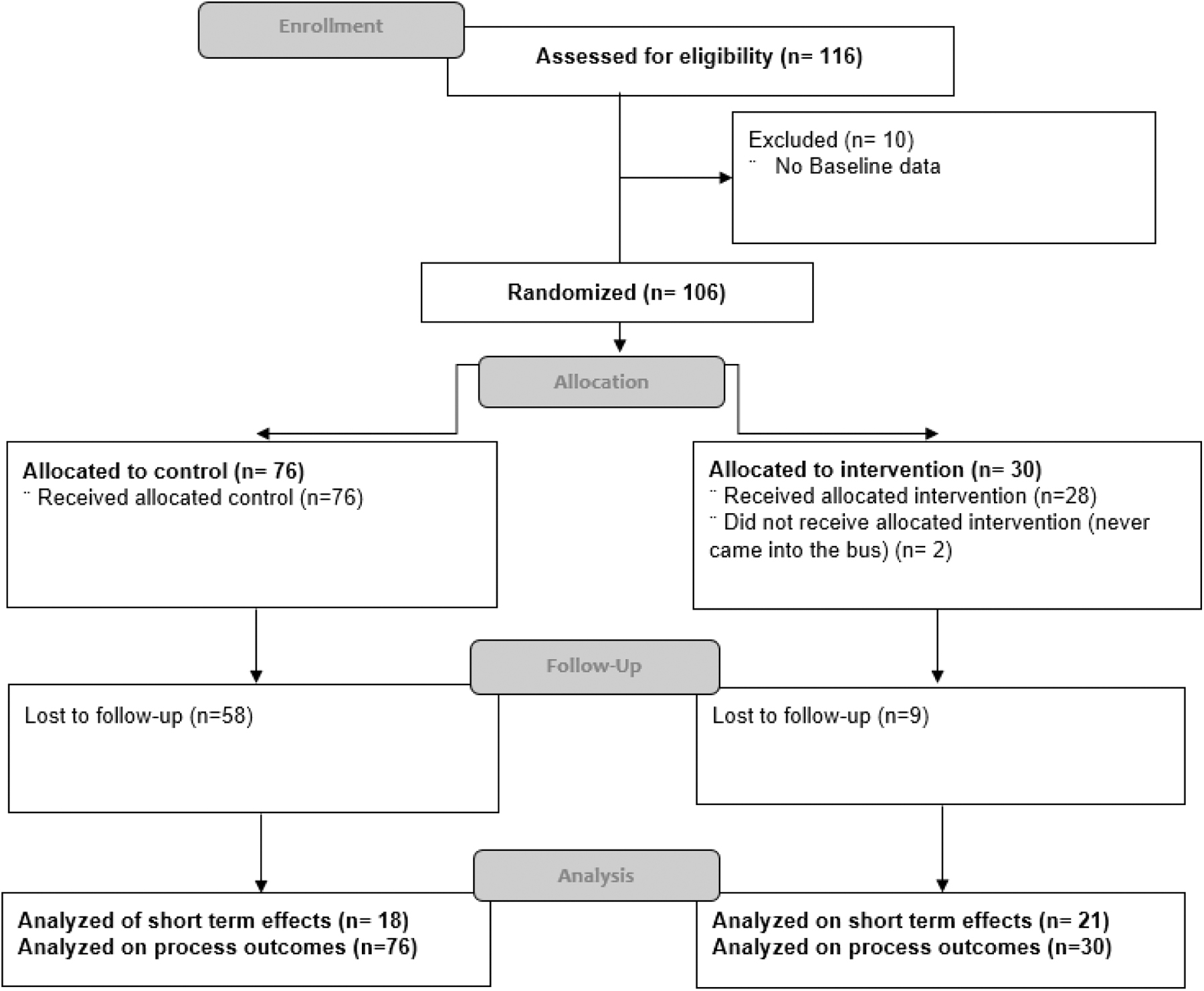
Flow chart.
Characteristics of Participants at Baseline
MD, missing data; Med, median; Q1: 1st quartile; Q3, 3rd quartile.
Attractiveness and player participation
All the participants (in the control and intervention group) were recruited on a single day and those in the intervention group reported clues of satisfaction (Table 2).
Verbatims Associated with the Analyzed Themes
Participation in the intervention sessions
Of the 30 randomized players, 2 never entered the bus; 5 attended only the first session and never returned; the others attended 3 (3/30) or 4 (all) (20/30) sessions. All the planned sessions were completed. All players collected their reward badges at the end of the sessions.
On two occasions, participants left a session and justified this (technical problem, appointment in real life).
A median of eight players were present at each session [Q1:7–Q3:9]; 399 [Q1:383–Q3:407] chats were posted by session by players (70% of chat time per session) and 179 [139–205] by animators. The distribution of discussion time was very variable between the players (between 2 chats and 126 chats per session). No troll player (players who try to intentionally ruin the gaming experience for other players) was observed.
Participation in the quantitative study and lost to follow-up
The final questionnaire was completed by 39/106 players (37%). Those who were lost to follow-up (no final assessment) was 30% of the intervention group and 76% in the control group. In the intervention group, the 21 final respondents were mainly players who participated in every session (19/21, 90%).
Study adhesion
Among respondents to the final questionnaire, 6/18 participants of the control group and 16/21 of the intervention group reported they went on governmental information websites through the information kiosk present in the game (no information on their motivation to visit these websites).
In the intervention group, 12/21 players reported speaking about the intervention with family or friends in real life, and 18/21 with other Habbo players. We do not have the information whether these Habbo were in the study or not. Seventeen out of twenty-one reported that during sessions, they were strictly participating only in the session (no work, lessons, or other things on internet or real life). At the time of final evaluation, 20/21 appreciated the intervention “a lot” or more.
Evolution under the intervention of intentions and attitudes toward tobacco
Results showed no change in terms of high intention to use tobacco (Supplementary Data S1). Two players who reported smoking at baseline declared themselves to be no longer smokers at week 4; both were in the intervention group.
Norms and representations
Final questionnaires showed little changes in evaluation of norms and representations (Table 3). Results showed that players in the intervention group reinforced their opinion that smoking allows them to manage stress. In the intervention group, a reinforced opinion of the usefulness of smoking for talking with a stranger was reported, but no change on having more friends was noticed, which is consistent with chats during the sessions (Table 2).
Norms and Representations Related to Smoking Behaviors
One missing data.
The behavioral belief score was measured by 14 items matched by 2 and can be interpreted as the smallest tabagism risk when the score is negative up to −21; and greatest risk when the score is positive up to +21, 0 indicating neutral behavior (e.g., “if I smoke in the next month I will be popular”: probably [rated 7] to probably not [rated 1], match with the item “being popular will be”: very positive [rated +3] to very negative [rated −3]). A positive score indicates a risk of tabagism related to this item. A negative score indicates a protection of tabagism related to this item.
Two missing data.
Discussion
This study showed the feasibility of integrating a smoking prevention intervention into online community games, attracting, reaching, and retaining target audiences through sustainable interventions. However, Evolution under the intervention of norms and attitudes was limited.
Reach
The chosen game led us to expect to reach more adolescents than young adults. The observed population (mean age 23) may be a result of the gaming community aging with the game, and randomization using a baseline questionnaire probably selected the most motivated players, possibly the most mature or those looking for a revival of interest, accounting for the “older” profile of players. Initial recruitment and intervention sessions took place on a weekday during daytime, which probably led to a particular study population present in the game at these times. Reported smoking prevalence was equivalent to that of the general French population 18–24 years of age (35.3% daily smokers in males and 28.8% in females 25 ). Our study group contained a higher proportion of unemployed than the general French population of the same age, 26 and unemployed young people are more at risk of smoking. 25 The place and scheduling of intervention may therefore enable reaching a population not exposed to prevention interventions in the school or work context.
Selection dependent on willingness to complete a baseline questionnaire may induce a recruitment bias but allowed us to deliver our interventions in quite controlled conditions. The “barrier” of the questionnaire limited “troll” players.
Intervention place
Our experience shows that certain elements are important to ensure the feasibility of research in online community games: use of the elements of the game (functionalities, formats.), based on interactions and support between peers, diversifying and repeating the intervention, and adopting a language and a posture consistent with the context of the game. The needs for participant selection, randomization, and completion of questionnaires inherent in experimental studies could be implemented with the available tools of the game: creation of dedicated places, restriction of access to these places, distribution of incentives (adapted to each game), and pop-up windows.
Attractiveness and retention
The attractiveness was demonstrated particularly in the intervention group, where participation was high and the response rate to final questionnaires satisfactory. Another positive indicator is the high number of chats exchanged per session, and the proportion of speaking time between facilitators/players in favor of players. By contrast, the response rate in the control group to the final questionnaire was low. Further reflection is needed on the control to be offered to players who expect novelty in the game.
The nonresponse rate to questionnaires also questions the acceptability of the length 27 and mandatory aspect of our questionnaires in a game context.
Tobacco-related outcomes
This pilot study was not an efficacy trial; the objective of studying evolution under the intervention of tabagism-related measures was only exploratory and should be interpreted with caution. Moreover, the evolution of measures was investigated in the very short term: at 4 weeks of intervention, the sustainability of any changes and their potential impact on behavior is questionable.
In comparison of our participants to the general French population, we note a better representation of smoking by young people in our study. In the French population 15–25 years of age, in 2010, 18% thought that smoking makes one feel more comfortable in a group—much less than in our study population where more than a third of players thought this. The proportion believing that smokers are less well accepted (26%) was also less than in our study population. 28
We observed in the intervention group an evolution over the 4 weeks of the beliefs that tobacco could help manage stress or talk with a stranger. This increase in belief is not enough to suggest that it will cause a change in smoking behavior according to the model on which this intervention is based, where beliefs are associated with intentions and attitudes to bring about a change in behavior. Nevertheless, this should be considered an unintended side effect of our intervention. Health promotion interventions could present side effects. 29 This counterproductive effect observation will allow to better anticipate the deployment of this type of intervention in the future. Indeed, our discussion group mixed smokers and nonsmokers, the sharing of experience of some players—although not advocating the use of cigarettes—may have reinforced certain beliefs in others. A separation of the groups according to the behaviors will be planned in our future studies.
Strengths and limitations
This is the first study integrated into an existing game through partnership with a videogame entertainment company and reaching a community of players whose presence in the game is not linked to a concern with health issues. It has shown that this approach may offer a way to meet public health challenges of prevention and inequalities with a hard-to-reach population. In the intervention group, feasibility and acceptability were demonstrated using the means and constraints of the game to ensure randomization, to administer questionnaire surveys and to carry out interventions appreciated by the players, even though these were based on a theory of smoking prevention intervention, whereas a notable proportion of our participants were already smokers. On the other hand, the study highlighted potential weaknesses: the difficult balance between technical constraints and the implementation of randomization as recommended, the difficulty of following and motivating players over time to measure short-, medium-, and long-term effects of an intervention, and of finding a relevant, attractive, and feasible control intervention.
This study was not primarily intended to investigate the effectiveness of the intervention, so the number of subjects needed was decided on the objective of feasibility; this resulted in the impossibility of carrying out tests with adequate statistical power to conclude on the intervention effects.
Conclusion
This pilot study showed that conducting public health research in an existing videogame is feasible. In the targeted gaming community, the intervention was acceptable and allowed the delivery of innovative interventions to audiences with diverse social profiles. The results increase our experience with videogames and identify specific parameters to enable research implementation and evaluation. It allowed us also to identify the potential counterproductive effects of such interventions. The study will enable us to upgrade and assess an intervention based on these results through a large-scale trial.
Footnotes
Acknowledgments
The authors thank Anita Burgun (INSERM, Centre de Recherche des Cordeliers, UMR 1138 Equipe 22) for her contribution to the development of the project; Coralie Cantin (Habbo) for his great help as community manager of the Habbo game; Habbo ambassador players who made it possible to optimize the delivery of the intervention; Habbo players who participated in the intervention and provide helpful feedback; Vanessa Rousset and Véronique Regnier (Centre Hygée, HESPER EA 7425) for their participation in the reflection on the study; and Olivier Lareyre and P2P teams directed by Florence Coussin-Gelie for the questionnaire used.
Authors' Contributions
E.L.R.: conceptualization; methodology; project administration; supervision; investigation; formal analysis (qualitative and quantitative); validation; interpretation of data; writing—original draft; writing—review and editing; and funding acquisition. P.M.: conceptualization; investigation; formal analysis (qualitative); interpretation of data; writing—original draft; and writing—review and editing. C.A.: conceptualization; methodology; resources; interpretation of data; validation; writing—review and editing; and funding acquisition. L.M.: conceptualization; interpretation of data; and writing—review and editing. J.K.: conceptualization; interpretation of data; and writing—review and editing. B.C.: conceptualization; interpretation of data; and writing—review and editing. B.G.: conceptualization; interpretation of data; analysis supervision; and writing—review and editing. F.C.: conceptualization; interpretation of data; and writing—review and editing. C.D.: conceptualization; facilitators' training; interpretation of data; and writing—review and editing. P.A.: conceptualization; interpretation of data; ethics and regulatory supervision; and writing—review and editing. A.D.: conceptualization; methodology; interpretation of data; validation; and writing—review and editing. A.B.: conceptualization; methodology; resources; interpretation of data; validation; writing—review and editing; and funding acquisition.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
We thank the Institute for Public Health Research for funding this study (call for proposals—TABAC 2018 n° grant: TABAC18-026_AM)—no involvement from funders in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.