
Abstract
Objective:
Muscle strength and balance impairment change the control strategy and increase the probability of falling. This study aimed to investigate the effect of 6-week strength-balance training through virtual reality exergaming (VRE) on muscle strategy during the limits of stability (LOS) test, fear of falling, and quality of life (QOL) in osteoporotic women.
Materials and Methods
: Twenty volunteer postmenopausal women with osteoporosis were randomly allocated to the VRE (n = 10) and traditional training (TRT as control, n = 10) groups. The VRE and TRT strength-balance training was performed for 6 weeks and three sessions per week. Before and after exercise, the muscle activity (onset time, peak root means square [PRMS]) and hip/ankle activity ratio were assessed by the wireless electromyography system. The muscle activities of the dominant leg were recorded during LOS functional test. The fall efficacy scale and QOL were assessed. Paired t-test was used to compare results within groups, and an independent t-test was used to compare the percentage changes in parameters between the two groups.
Results:
The VRE improved the onset time and PRMS. The VRE significantly reduced the hip/ankle activity ratio in the LOS test's forward, backward, and right directions (P < 0.05). No significant change was seen in all directions of the LOS functional test in the TRT group (P > 0.05). VRE reduced the fall efficacy scale (P = 0.042). Both VRT and TRT improved the total QOL score (P = 0.010).
Conclusion:
VRE was more effective in decreasing the onset time and hip/ankle ratio of muscle activation. The VRE is recommended to induce a better ability to reduce the fear of falling and control balance during functional activity in osteoporotic women.
Clinical Trial Registration number: IRCT20101017004952N9.
Introduction
Osteoporosis (OP) is a complex disease characterized by impaired bone microarchitecture and reduced bone mineral density, resulting in bone fragility and increased risk of fracture. 1 This most common bone metabolic disease 2 is one of the major health problems in any country because of its association with fractures. 3 Women with OP are at high risk of fall-related fractures. 4
Since most fractures in people with OP occur during a fall, 5 the primary goal of treating patients with OP in rehabilitation is to reduce the risk of falls and fractures. 6 So exercise has been recommended to treat women with postmenopausal OP. 7 Traditional strength and balance training has reduced falling risk by improving postural control 8 and increasing muscle strength. 9 Although evidence is overwhelming that conventional strength and balance training positively reduce falling risk, the compliance of older people in traditional exercise programs is still poor, 10 and people with OP are often reluctant to engage in these exercise classes for fear of falling and trauma. 11 Also, other factors such as pain, environmental barriers (real or perceived), and lack of motivation may affect patient participation and exercise performance. 12 Therefore, it should be considered when developing interventions to encourage exercise motivation and increase exercise activity.
One of the promising intervention tools that are sought to facilitate this goal is virtual reality exergaming (VRE) technology. 13 VRE technology provides visual and sensory feedback on the exercise compared with traditional training (TRT). It makes individual perceptions more effective, increases patient motivation, 14 and activates brain tissues. 15 Kim et al found that virtual reality or exergame-based exercise programs improve balance control and hip muscle strength in older adults. 16 Sato et al concluded that 24 sessions of an Xbox exercise improve lower body muscle strength and balance among older adults.17,18
Sadeghi and Shojaedin demonstrated that 3 weeks of virtual training could improve the fall risk index and functional mobility in healthy older women. 19 Also, in a randomized clinical trial, Singh et al evaluated the effects of virtual reality and traditional balance exercise on the risk and fear of falls in women older than 56 years. They concluded that virtual reality exercise could increase balance confidence and decrease the risk of falls among community-dwelling women. 20
In postmenopausal women with OP, due to physiological changes caused by aging and OP, we face a decrease in muscle strength and changes in the pattern of muscle activity. 21 These people are using a more hip strategy instead of an ankle strategy, which leads to the probability of instability and falling. 22 As the most crucial variable in maintaining postural control and muscular activity during functional balance, the hip and ankle strategy has received no attention, especially in women with postmenopausal OP. Considering the advantages of VRE, this study aimed to compare the VRE and traditional exercises on the pattern of lower extremity muscle activity during the challenging functional balance activity in osteoporotic women.
The limits of stability (LOS) were considered because it is associated with weight shift in the medial-lateral and anterior-posterior, used frequently in daily activities. We hypothesized after 6-week VRE, the lower limb's muscle activity, including the onset time, peak root means square (PRMS), and the hip/ankle ratio of muscle activity, would improve compared to the traditional strength-balance exercises. In addition, we hypothesized that VR training would be more successful than conventional strength-balance training in improving the quality of life (QOL) (Qualeffo-41) and the fear of falling in postmenopausal women with OP.
Methods
This study is a randomized control trial with the (IRCT20101017004952N9) registration code conducted in the movement disorder laboratory of the Physical Therapy Department at Tarbiat Modares University. The Medical Ethics Committee of Tarbiat Modares University approved the study (IR.MODARES.REC.1398.151).
Subjects and experimental design
The subjects were recruited from individuals admitted to bone densitometry clinics. So far, no study has examined the effects of VRE on muscle activity in people with OP; therefore, the sample size was estimated according to Kim et al, which examined the impact of virtual reality-based exercise programs on improving hip flexor muscle strength in older adults. 16 The calculation was based on the mean ± standard deviation of hip flexor strength in virtual reality (29.48 ± 7.42) and control (18.44 ± 3.77) groups, the effect size of 1.87, and the alpha of 5%, power of 80%, and an allocation ratio of one.
Inclusion criteria were as follows: 48–65 years of age, body mass index of 22–30 kg/m2, menopause at least 12 months before the study, lumbar T-score less than or equal to −2.5, no record of regular exercise (at least 30 minutes, 2–3 days/week), and not undergoing hormone therapy for at least the last 6 months. The education level of participants was at least the complete high school. The global normal cognitive function was considered to have at least scoring of 24 based on the Mini-Mental State Examination. The physical activity scoring was 5–7, according to the Baecke questionnaire. The volunteers did not smoke or drink alcohol. Their coffee consumption was a maximum of 1–2 glasses per day. Subjects were taking Ca-D supplements prescribed by the rheumatology consultant; they were asked to maintain their usual weekly diet during the study, as recommended by the rheumatologist.
Any subject with secondary OP, history of osteoporotic fracture, diabetes, inability to stand independently, history of cardiovascular diseases, or balance impairment due to other conditions, such as orthopedic, neurological, vestibular, or visual disorders, was excluded. Also, participants were excluded if they were unwilling to participate and reported pain and discomfort after exercise therapy.
Among 54 people assessed for study eligibility, 20 were recruited and randomly allocated to VRE (n = 10) and TRT (as a control, n = 10) groups (Fig. 1). Randomization was performed by an external observer using closed envelopes in blocks of four; in each block, two persons were randomly assigned to one of the groups. The assessor was blinded to the allocation of participants. Women in each group were asked not to alter their routine physical activity or dietary patterns during the study. All participants consented to participate after the study protocol was explained.
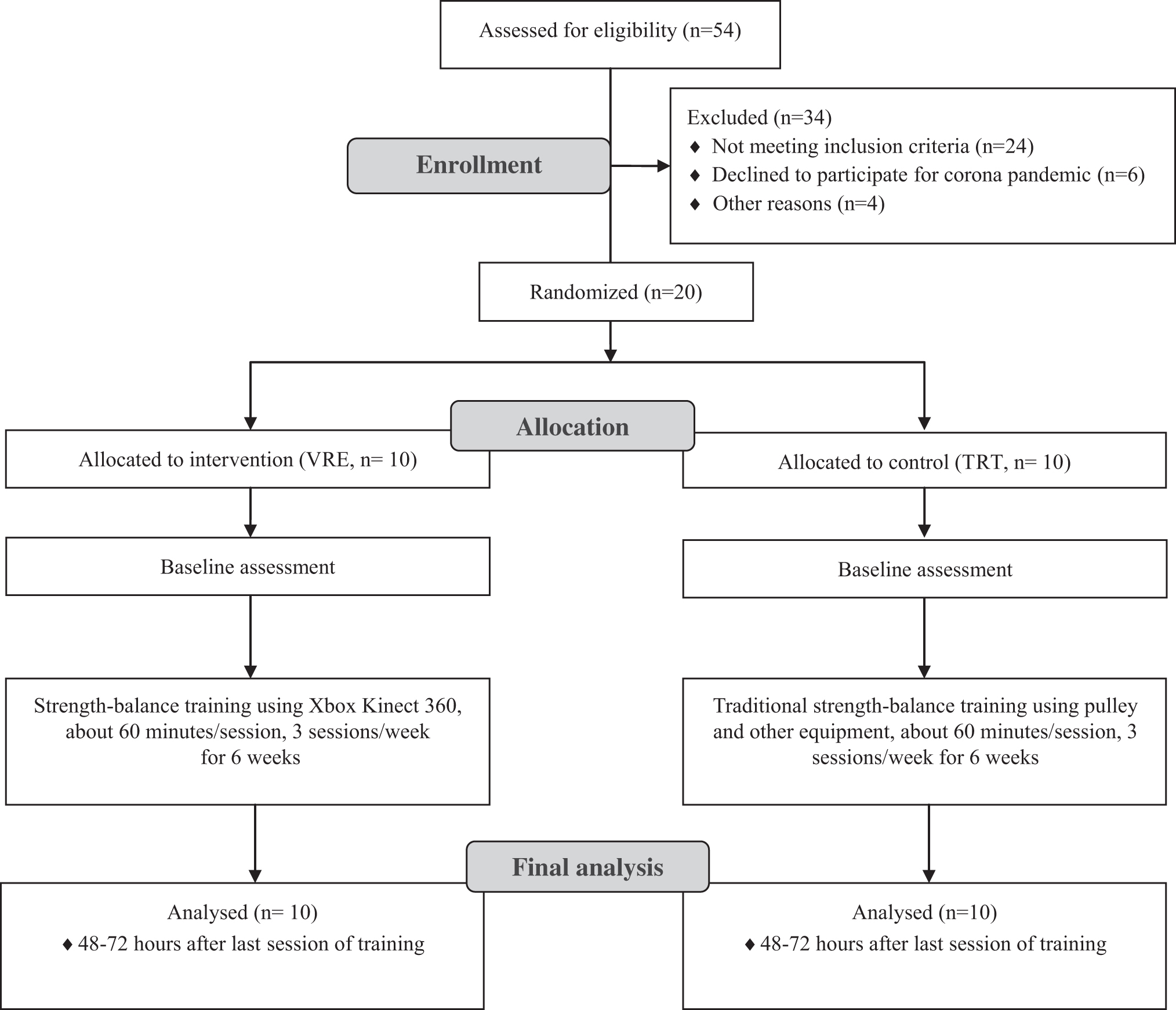
Randomized controlled trial flowchart for the study. TRT, traditional training; VRE, virtual reality exergaming.
All activities were performed thrice a week, about 60 minutes per session, for 6 weeks. Before and after training (48–72 hours after the last training session), a wireless electromyography system recorded muscle activities of the predominant lower extremity during the LOS functional balance task. Furthermore, both groups considered the scores of FES and Qualeffo-41 before and after exercise.
Limits of stability
The LOS as a functional balance test were performed using the force plate (9286B; Kistler Co., Winterthur, Switzerland) and Kistler-Mars software. 23 Before the data acquisition, each participant was familiarized with the test procedure. The preferred position of the subject's feet in the first session (before training) was controlled by recording the position of feet on a special sheet attached to the force plate. The exact situation was used for the LOS test after training. The examiner stayed close to the participants to protect them from probable falling.
At the LOS test, the participant was asked to shift her weight in four directions without taking any steps. According to the Mars software, the order of the shift of the center of gravity was forward, backward, right, and left, respectively. After each direction, they had to return to the starting position and then switch to the direction of the other highlighted target. The participant was asked to stand barefoot on the force plate in a two-legged position, while keeping their arms next to the body. An LCD screen (56 inches, 2 meters from the participant, and 1.5 meters above the ground) showed visual feedback of center of pressure (COP) displacements and displayed the COP's real-time position and movement. Subjects were instructed to move the COP cursor quickly and accurately toward the highlighted target without losing their balance.
Electromyography assessment
A 16-channel wireless electromyography system (Aktos; Mayon, Inc., Switzerland) and Nexus software (Vicon Nexus 2.8.1; Oxford, UK) were used to record the electrical activity of muscles during LOS functional balance test. Electrodes were placed on the belly of each muscle in line with fiber direction, according to the SENIAM method. 24 The skin was shaved and appropriately cleaned with medical alcohol to reduce the impedance to less than 10 mΩ. The disposable surface electrodes (Shanghai INTCO electrode Manufacturing Co., Ltd., China) with 2-cm intervals were tightly fixed to the skin to minimize movement artifacts.
We recorded the activity of the gluteus maximus (GMax), gluteus medius (GMed), rectus femoris (RF), biceps femoris (BF), medial hamstring (MH), tibialis anterior (TA), soleus (SOL), and lateral head of the gastrocnemius muscle (LG) of the dominant leg. The muscle activity recording was done with a 20–500 Hz bandpass and a sampling frequency of 1200 Hz.
These electromyography (EMG) sensors were true differential without reference electrodes with common mode rejection ratio (CMRR) 120 dB and SNR 50 dB. Maximum voluntary isometric contraction (MVIC) was used to normalize the electromyography signals recorded during LOS. The measurement of MVIC was done by a digital hand-held dynamometer (Hand-held Dynamometer; Lafayette Instrument Co., Lafayette, IN) according to the Make method because of its repeatability reported of 0.909. 25 Before MVIC, participants performed two to three warm-ups near maximal efforts for familiarization. The MVIC holding was five seconds, and each muscular group was tested three times with 30 seconds of rest between them.
A blinded expert physiotherapist did MVIC on the dominant side for ankle dorsi/plantar flexion and knee extension at sitting position, knee flexion and hip extension at prone lying, and hip abduction at side lying. The average value (kg) was used for subsequent analyses. The procedure, which included stabilized regions, and dynamometer placements, was based on Bohannon. 26 In addition, during the MVIC test, the EMG signal of target muscles was recorded to normalize the muscle activities during the LOS task. Participants were given verbal encouragement during all MVIC tests. All measured were done at 9–11am. The environmental conditions were same for light and temperature (20–23°C). The laboratory environment was quiet and noise free to avoid the subject's stress and the recording of disturbing information.
Fall efficacy scale
The fall efficacy scale questionnaire assessed the fear of falling in postmenopausal women with OP. This questionnaire is an individual test based on 10 daily activities a person faces during the day, including bathing and shopping. Each question is scored from 1 to 10 based on the person's level of trust (1 = complete trust and 10 = lack of confidence).
Therefore, the person who gets a total of 10 scores (1 score for each question) is a person who either did not fall or is not afraid of falling (normal). In comparison, if a person gets a total of more than 10 scores, she is a person who has experienced a fall, while performing one or more daily activities or feels that a fall may occur (abnormal). 27 The Persian version of the fall efficacy scale questionnaire was used as self-report. Persian translated version of the «Fall Efficacy Scale-International» has acceptable validity and reliability for the Iranian older adult population. 28
Qualeffo-41
The Qualeffo-41 questionnaire is a complete questionnaire that covers all aspects of QOL. The Persian version of the Qualeffo-41 questionnaire was used as self-report. The validity and reliability of this tool have been confirmed in Iranian women with OP. 29 This questionnaire consists of 41 questions that examine the QOL of women with OP in 5 areas of pain, physical function (daily activities, housework, and mobility), leisure and social activities, general health perception, and mental function. The subscores and total scores are expressed as a numerical value from 0 to 100; zero is the best score and 100 is the worst QOL. 30
Virtual reality exergaming
The Xbox Kinect 360 system (Microsoft Corp., Redmond, WA), which consists of a Kinect sensor and console, was used for VRE. The game device includes an infrared camera (Kinect sensor) that recognizes the user's real-time movement without needing a particular controller. To play active video games, the participant stood approximately 1.5–2 m from the 49-inch TV with the Kinect sensor placed below the TV at about 1.5 m above the floor surface. All exercise sessions began with 5 minutes of light dynamic warming-up activities, including sidestepping, forward-backward walking, and stretching. The training ended with a 5-minute cool-down program, including slowly walking and performing global stretching exercises. After receiving a gameplay demonstration from a trainer, the participants engaged in the games. The duration of VRE was 51 minutes of an active video game, three times per week (on nonconsecutive days) for 6 weeks.
The exergames had three levels: easy, intermediate, and difficult. Participants started the exergames with an easy level in the first 2 weeks. In the second 2 weeks, the intermediate level, and in the third 2 weeks, the participants performed the difficult level of exergames. As the game level progresses, the computer opponent acts faster (higher speed), and the player must perform with higher accuracy and more challenge.
We selected games that cause the most involvement in the lower and upper limbs and trunk muscles in a weight-bearing state (Table 1). The 1-minute break between each new game and 30 seconds of rest to repeat the next set of the same game were considered for everyone.
Description of Each Game in the Kinect Motion Sports, Your Shape, and Kinect-Adventure Pack
Traditional training
In this group, the participant performed a series of specific strength-balance training 3 days per week for 6 weeks. Training included biceps curl and scapular retraction of upper limbs, hip abduction, adduction, flexion, extension, knee flexion and extension (bilaterally by pulley), ankle dorsiflexion, and plantar flexion (using tilt board) as 2 sets and 10 repetitions in each collection. The duration of each session was about 45–50 minutes; the warm-up and cool-down were considered the same as the VRE group. MVIC was used for the training to be progressive in the TRT group. In the first 2 weeks, activities were performed with 50% of the MVIC; for the second and third 2 weeks, 55% and 60%, respectively. 31
In both groups, we also measured the 10-point Borg rating of the perceived exertion scale (Borg), which individuals subjectively rate their level of exertion during exercise. In the first 2 weeks of training, we determined the scale of 2–3 for light intensity; in the second 2 weeks, 4–5 for moderate intensity; and in the third 2 weeks, 6–7 for hard intensity. Borg's score was evaluated at the middle and end of each training session. Because the exercises started from an easy level and increased progressively and that proper rest was also considered between the exercises, Borg's scores were also at the determined levels, and there was no problem continuing the exercises in different sessions.
Data processing
All EMG data were processed using custom code written in Matlab (R2015b; Mathworks, Inc., Natick, MA). The raw electromyography signal was filtered with a second order Butterworth filter, rectified, and normalized to the muscle's MVIC. We calculated the root means square (RMS) value in 50-millisecond windows. The onset time of muscle activation and PRMS were extracted during the LOS test, and these parameters were calculated for four directions separately. Furthermore, we calculated the ratio of hip/ankle muscle activity following the formula,
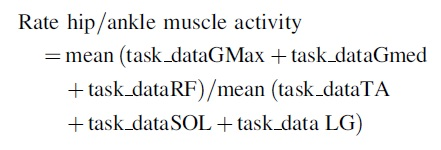
In this formula, task _data means the filtered and normalized EMG of each muscle related to the desired directions of the LOS task.
Statistical analysis
The normal distribution of data was tested through the Shapiro-Wilk test (P > 0.05). A paired-samples t-test was performed to evaluate the results within the group, and an independent t-test was performed to compare the results between the two groups. If the data were not normally distributed, the Wilcoxon and Mann-Whitney nonparametric equivalence tests were used. The mean percentage change
Results
The demographic parameters of the two groups are presented in Table 2. As shown in this table, the independent t-test indicated no significant difference between the two groups (P > 0.05).
Anthropometric Characteristics of Participants (Mean ± Standard Deviation)
BMI, body mass index; TRT, traditional training group; VRE, virtual reality exergaming group.
Muscle activity during LOS
Forward direction
The values of EMG parameters in the four directions of the LOS test are reported in Tables 3 and 4. After training in the VRE group, the onset time of the BF was reduced significantly (P = 0.047, effect size = 0.91). In the TRT group, onset time did not decrease significantly, and there was no significant difference between groups (P > 0.05).
Onset Time of Muscles in the Four Directions of the Los Test (Mean ± Standard Deviation)
Statistically significant (P ≤ 0.05).
FLOS; BLOS; RLOS; LLOS, forward; backward; right and left directions of LOS test.
BF, biceps femoris; GMax, gluteus maximus; GMed, gluteus medius; LG, lateral gastrocnemius; LOS, limits of stability; MH, medial hamstring; ND, no difference; RF, rectus femoris; SOL, soleus; TA, tibialis anterior.
Peak Root Means Square of Muscles in the Four Directions of the Los Test (Mean ± Standard Deviation)
Statistically significant (P ≤ 0.05).
FLOS; BLOS; RLOS; LLOS, forward; backward; right and left directions of LOS test.
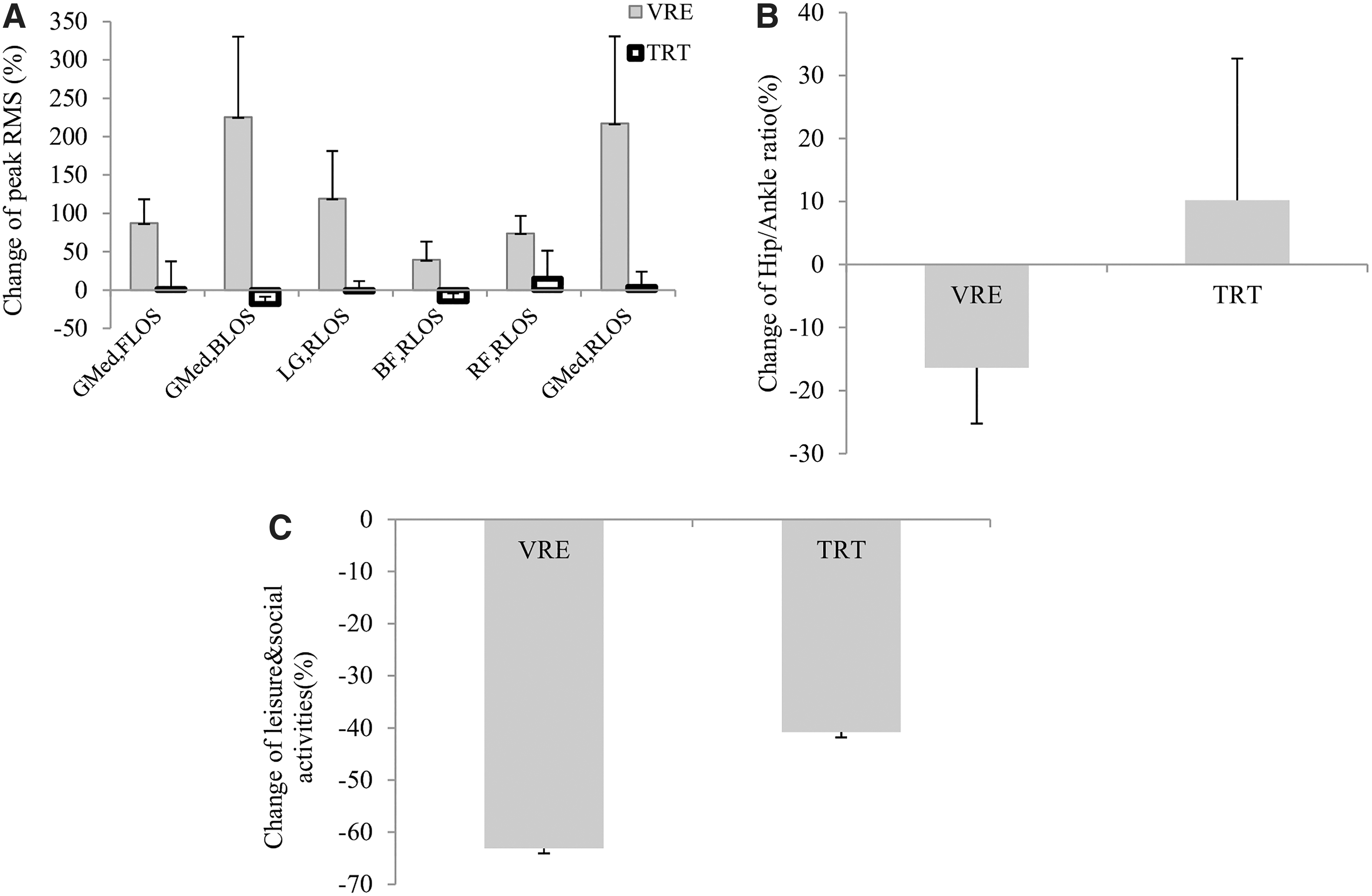
In the VRE group, PRMS of LG (P = 0.049, effect size = 0.85), BF (P = 0.050, effect size = 0.70), RF (P = 0.030, effect size = 0.72), GMax (P = 0.016, effect size = 1.01), and GMed (P = 0.008, effect size = 1.17) showed a significant increase after the training period. After TRT, the PRMS of SOL (P = 0.044, effect size = 1.10) and MH (P = 0.039, effect size = 0.76) was significantly increased. The PRMS of the GMed showed a significant increase in the VRE group than the TRT group (increase by 87.29% and 1.31%, respectively; P = 0.012, effect size = 0.87; Fig. 2A).
Between-group comparison.
Backward direction
After training, the onset time of BF decreased significantly in the VRE group (P = 0.030, effect size = 1.00). There was no significant change between the two groups (P > 0.05). Also, the PRMS of TA, RF, and GMax increased significantly (P = 0.031 effect size = 0.81, P = 0.002 effect size = 1.73, and P = 0.032 effect size = 0.79, respectively). In the TRT group, the PRMS of GMax increased significantly (P = 0.044, effect size = 0.68). The change in the PRMS of GMed was significant between the two groups (P = 0.031, effect size = 1.03). It increased by 225.50% in the VRE group and decreased by 18.08% in the TRT group (Fig. 2A).
Right direction
After training, there was no significant decrease in the onset time of muscle activity in the VRE and TRT groups (P > 0.05). After VRE, the PRMS of LG, RF, and GMed increased significantly (P = 0.014 effect size = 0.82, P = 0.040 effect size = 0.83, and P = 0.031 effect size = 0.63, respectively). TRT failed to significantly change the muscle's PRMS (P > 0.05).
The changes of the PRMS in LG (which increased 119.35% in the VRE group and decreased 1.73% in the TRT group), BF (which increased 39.45% in the VRE group and dropped 14.64% in the TRT group), RF (which increased 74.00% in the VRE group and 14.73% in the TRT group), and GMed (which increased 217.01% in the VRE group and 4.38% in the TRT group) were significant between groups (P = 0.001 effect size = 0.85, P = 0.042 effect size = 0.93, P = 0.022 effect size = 0.82, and P = 0.020 effect size = 0.82, respectively; Fig. 2A).
Left direction
After training, there was no significant decrease in the onset time of muscle activity in the VRE and TRT groups (P > 0.05). After training in the VRE group, the PRMS of MH and RF muscles increased significantly (P = 0.042 effect size = 0.75 and P = 0.013 effect size = 1.66, respectively), but the TRT group showed no significant change. In this regard, there was no significant change between the two groups (P > 0.05).
The ratio of the hip/ankle muscle activity
After VRE, the hip/ankle ratio decreased significantly in the forward direction of the LOS functional test (P = 0.034, effect size = 1.14; Fig. 3A). In the backward and right directions, this ratio was significantly reduced by 0.33 and 0.43, respectively (P = 0.035 effect size = 1.13 and P = 0.048 effect size = 1.06, respectively; Fig. 3B, C). In the left direction, this ratio showed no significant change (P > 0.05, Fig. 3D). After TRT training, there was no significant change (P > 0.05, Fig. 3A–D). In the right direction of the LOS functional test, this ratio showed a significant decrease in the VRE (−16.38%) compared to the TRT group (+10.20%) (P = 0.043, effect size = 0.88, Fig. 2B).
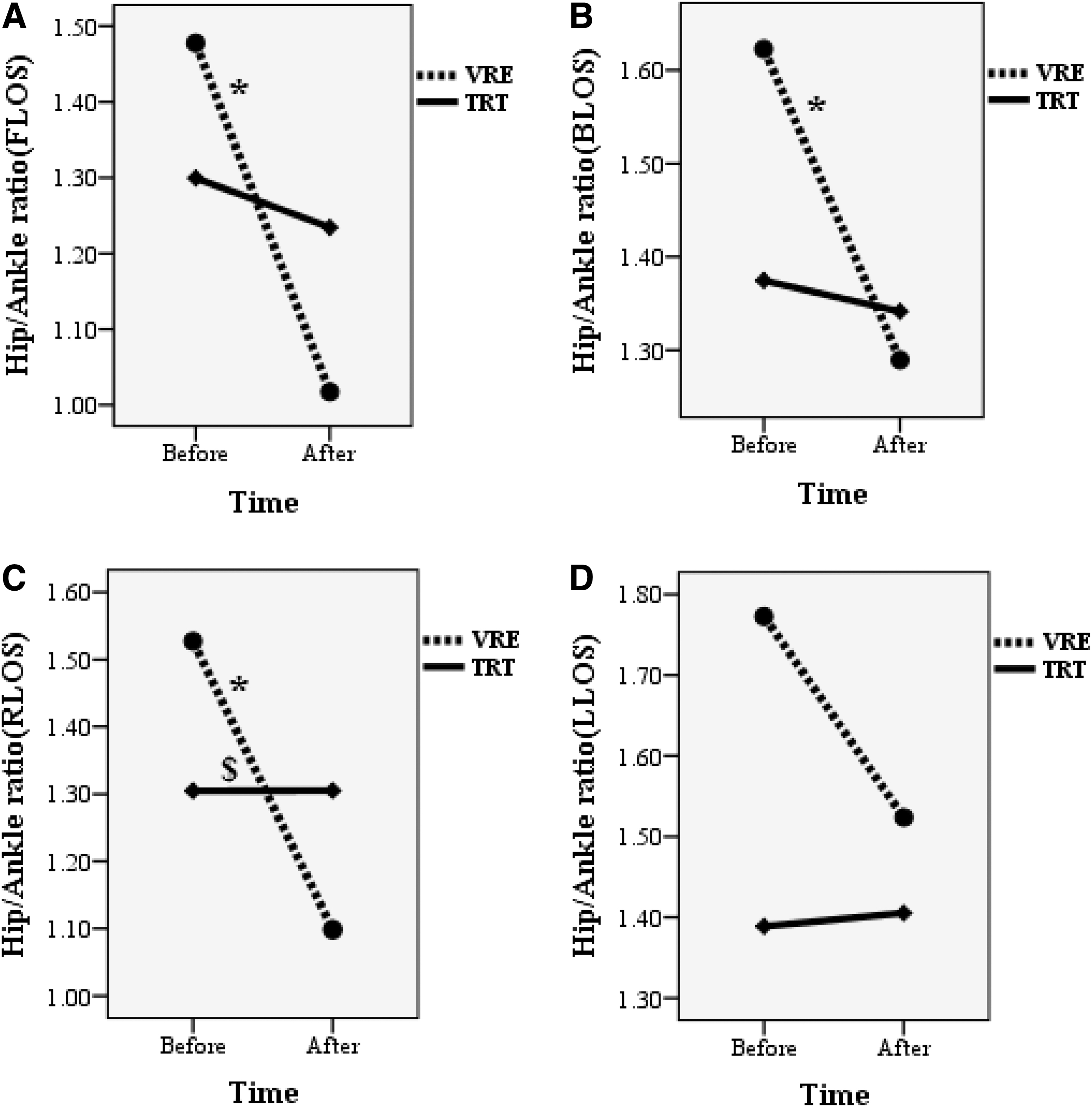
The ratio of the hip/ankle muscle activity of the VRE and TRT groups.
Fall efficacy scale and Qualeffo-41
After 18 sessions of VRE, the fall efficacy scale score decreased significantly (P = 0.042, effect size = 0.97), but in the TRT group, this score was not significant (P = 0.066). Intergroup comparison was not significant (P = 0.579) Figure 4.
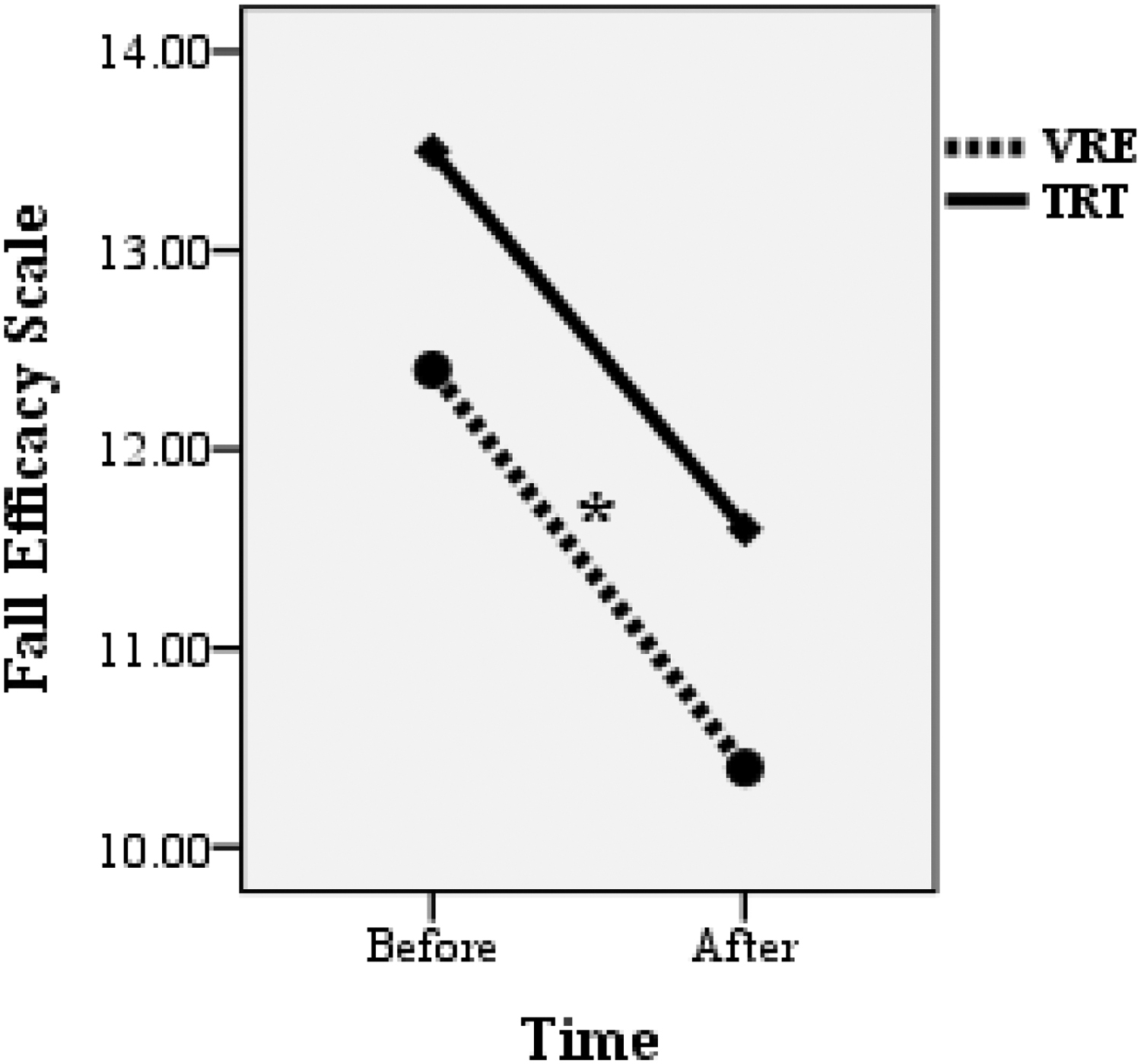
Fall efficacy scale of the VRE and TRT groups. Intergroup comparison was not significant. *Significant difference between the before and after training in the VRE group.
The values of the Qualeffo-41 questionnaire are reported in Table 5. After training, the total score and scores related to mobility, leisure and social activities, and general health perception decreased significantly in the VRE group (P < 0.001 effect size = 2.21, P = 0.009 effect size = 1.02, P < 0.001 effect size = 2.93, and P = 0.002 effect size = 1.41, respectively). The TRT group's total score and subscores related to pain, mobility, leisure and social activities, and general health perception decreased significantly (P < 0.001 effect size = 2.16, P = 0.009 effect size = 1.01, P = 0.002 effect size = 1.21, P < 0.001 effect size = 1.75, and P = 0.017 effect size = 0.91, respectively). The between-group comparison showed a significant decrease in the leisure and social activities in the VRE than in the TRT group (P = 0.010, effect size = 1.25; Fig. 2C).
Qualeffo-41 Questionnaire Scores in the Virtual Reality Exergaming and Traditional Training Groups (Mean ± Standard Deviation)
Statistically significant (P ≤ 0.05).
ADL, activities of daily living.
Discussion
The objective of this study was to evaluate the effect of 6 weeks of strength-balance VRE and TRT on the lower extremity muscle activity during the LOS functional balance test in postmenopausal women with OP. We hypothesized that 6-week VRE improves the lower limb muscle activity, hip/ankle muscle activity ratio, FES, and Qualeffo-41 score more effectively than the TRT in osteoporotic women.
After VRE, the onset time of muscles showed a decreased pattern, but it was significant only for BF in the forward and backward directions of the LOS test. TRT could not change the onset time of muscles in all directions of the LOS test. There is a connection between the timely initiation of proper postural control and falling, and a previous study has indicated the importance of shortening muscle onset time in postural control. 32 Laroche et al have stated that fallers women demonstrated 29% longer motor time than nonfallers women. 33 Therefore, muscle onset time or latency strongly discriminates fallers from nonfallers and is functionally significant in determining postural control ability. 34 Reducing reaction time after VRE in osteoporotic women is clinically valuable and may reduce the likelihood of falls because people activate their muscles in a shorter period to produce force. 35
Weakness of the lower limb muscles in postmenopausal women with OP is one of the most critical risk factors and makes them prone to falls. 35 Considering that there is a significant correlation between muscle strength and RMS in the elderly, 36 in our study, PRMS was investigated to observe the effects of VRE and TRT on muscle ability to control weight shifting in the challenging LOS functional task. The results indicated that VRE caused a significant increase in the PRMS of muscles in four directions of the LOS test.
Although in the TRT group, only the PRMS of SOL and MH in the forward direction and GMax in the backward direction increased significantly, in the VRE group, the increase of PRMS of the GMed in the forward and backward directions and LG, BF, RF, and GMed in the right direction were significant compared to the TRT group. These results indicate that the 6-week VRE is more effective in improving the muscle capability for controlling balance and stability during weight-shifting activity and decreasing the risk of falling during functional movement in daily living.
Park et al indicated that virtual reality exercise is an effective intervention for increasing the muscle activity of normal adults. 37 Better results in the VRE group than in the TRT group may be due to more dynamic movements of the lower extremity, broader center of pressure movements in anteroposterior and mediolateral directions, and more muscle competition during virtual training. 37 In VRE, people need to more and faster recruit motor units to maintain stability. 38 The unpredictability of exercises in VRE can be a factor in facilitating anticipatory control strategies. 39
In this regard, VRE is more beneficial because it appropriately modifies visual feedback to activate the brain tissues better. Providing appropriately modified visual feedback may facilitate activation of brain areas during VRE that causes better functional neuroplasticity. 15 The increase in brain activity in the temporal cortex 40 and prefrontal cortex areas 41 has been shown after performing exercises in the virtual reality environment. In this regard, Prochnow et al, using functional magnetic resonance imaging (fMRI), have shown the activation in brain areas related to motor control, including the supplementary motor area, the inferior frontal cortex, and the inferior parietal cortex. 42
Furthermore, the results showed VRE significantly decreased the hip/ankle ratio of muscle activity; however, TRT could not change it significantly. Intergroup comparison showed that in the right direction, the percentage change of ratio was significant, which decreased by 16.38% in the VRE group and increased by 10.20% in the TRT group. The ankle strategy has been identified as an essential balance strategy. It is the first muscle synergy activated with the loss of balance to restore the center of mass to the base of stability. 43 It has been stated that women with a history of falls have a decreased ability to recover balance with the ankle strategy. 34
In this study, VRE further increased muscle activity around the ankle joint, shifting the hip strategy to the ankle strategy in osteoporotic women. The center of pressure displacement is higher and multidirectional during VRE, probably generating ankle and hip postural control strategies. 44 Direction, range, and movement speed during VRE frequently change; therefore, this may require central processing speed strategies that induce greater demands and challenges on participants' neuromuscular systems than TRT. 20 Moreover, VRE probably demands the cognitive organization and execution of synchronized motions compared to TRT. 45 On the other hand, the realism of VRE may increase the sense of autonomy and independence in training 46 and reduce the age-related fear of falling. 47
Only VRE significantly reduced the fall efficacy scale and fear of falling into daily tasks in osteoporotic postmenopausal women. Repeated exposure to visual, auditory, and mechanical stimuli through the VRE can lead participants to learn the effects of motor control strategies and increase their involvement by responding to stimuli with active enjoyment. 48 After training, VRE and TRT improved the QOL in postmenopausal women with OP. The results showed that VRE significantly improved the QOL compared to the TRT group in leisure and social activities. It could be because participants were more motivated and enjoyed VRE. 49
The changes in mobility, leisure and social activities, and general health perception in VRE may be due to real-time games and feedback, which enhanced the experience related to brain plasticity by providing different game experiences. 50 Playing a variety of games and progressing to higher levels of training can create a sense of self-confidence among the VRE group and enhance their motivation, driving them to perform newer movements and increasingly complex activities; these can indirectly bring forth many positive effects on mobility, leisure and social activities, and general health perception. 51 Also, we observed a significant improvement in pain, mobility, leisure and social activities, and general health perception in the TRT group. The regularity of traditional balance-strength training can significantly improve the QOL in the TRT group. Although the QOL generally increased in both groups, VRE offers many opportunities to provide patient rehabilitation.
The development of modern technology makes it possible to use VRE as a telerehabilitation in patients' homes. Telerehabilitation increases the motivation to do home exercises and continue the rehabilitation program 52 during some status, such as the coronavirus pandemic. On the other hand, older people now need remote intervention to maintain their mobility safely. 53 Satisfaction and enjoyment of such interventions have been positively evaluated, and it has been stated that exergames create a motivating aspect for daily activities and training in the elderly. 54
This study has some limitations. First, a relatively small sample size; therefore, further research with a larger sample size is warranted to confirm the results of this study. The second is the lack of a no-intervention group, and the third is the lack of long-term follow-up to consider the QOL and falls. Furthermore, it was not possible to fully control the nutrition and unify the diet in the study groups, and this can be a limitation for the study. Future research should investigate the effect of VRE on muscle strategies and balance control in the faller community of osteoporotic women. It is also recommended that VR and traditional exercises should be designed in terms similar to open and closed chain conditions, which may clarify the effectiveness of the VR environment for the elderly community.
Conclusion
After 6 weeks of training in osteoporotic women, the VRE was more effective than TRT for improving muscle activity and shifting hip strategy to the ankle during functional balance tasks (LOS). Although both types of exercise improved the QOL, only VRE could reduce the fear of falling. The unwillingness of the elderly and people with OP to participate in training and daily activities due to fear of falling reduces the QOL. VRE's advantages over TRT may improve muscle strategy to decrease the fear of falling and increase the motivation to participate in functional activities.
Footnotes
Acknowledgments
We gratefully acknowledge all participants who participated in this study.
Authors' Contributions
Study conception and design: G.T. and M.G. Acquisition of data: G.T., M.G., N.B., and F.B. Analysis and interpretation of data: G.T., M.G., and F.B. Drafting of the article: G.T., M.G., F.B., and N.B. Critical revision: G.T. and M.G.
Authors' Confirmation Statement
Mr. M.G. and Prof. G.T. are from Tarbiat Modares University (Tehran, Iran); Prof. F.B. is from the University of Tehran (Tehran, Iran), and Prof. N.B. is from the Baqiyatallah University of Medical Sciences (Tehran, Iran), all where education and research are the primary function.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project has been supported by a grant from the Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran.