
Abstract
Introduction:
We investigated the effects of an exergames-based exercise program for older adults, and its benefits on their physical literacy (PL) domains, such as physical (mobility skills), affective (motivation and confidence), cognitive (knowledge about physical activity [PA]), and behavioral (daily exertion) when compared with a conventional exercise program and no training (NT) (control).
Material and Methods:
Forty older adults (mean age 72 years) volunteered and were randomized within three groups—exergame training (ET; n = 15), conventional training (CT; n = 14), and NT (n = 11). ET group performed training sessions based on a commercially available exergame console, while the CT group enrolled in a convention exercise program (aerobic, strength, balance, and flexibility exercises). The training program was conducted three times a week for 6 weeks. The Timed Up and Go Test (TUG), Exercise Confidence Survey (ECS), Motives for Physical Activity Measure-Revised (MPAM-R), Knowledge and Understanding Questionnaire (K&UQ), and total PA tracking (using wearable technology) were used as the study's outcomes. Outcome variables were measured at preintervention (week 0), postintervention (week 6), and at the time of final follow-up (week 9).
Results:
We observed a reduction in the ET TUG time at postintervention and follow-up. Also, a significant main effect for group and moment of measurement was observed for the Fitness-Health subscore, derived from MPAM-R. The values demonstrated by ET and CT were statistically different (P = 0.01) and a within-group comparison revealed significant differences in the ET from preintervention to both postintervention and follow-up (both, P = 0.01). We did not observe any other significant difference.
Conclusion:
Our results suggest that a 6-week exergame-based training program may have the potential in improving the physical and affective domains of PL in community-dwelling older adults. The topics related to fitness and health seem to be of interest in this population and programs can make use of them to improve the PL domains.
Introduction
The senior population is the fastest-growing age group worldwide. A world population of ∼2.1 billion older adults (>65 years) is expected by 2050, which is nearly double the current value. 1 As people age, they become more vulnerable to biopsychosocial changes, such as social isolation, dependence, and reduced physical and cognitive functions.2,3 These age-related changes may be due to the adoption of unhealthy lifestyle choices (e.g., decreased physical activity [PA], poor nutrition, etc.).4,5
According to Michel et al., 6 the most important factors of successful, healthy aging are daily habits such as well-balanced nutrition, social interaction, and PA practices. In particular, regular engagement in PA by older adults is effective in promoting social interaction, preventing age-related risks of chronic diseases, and reducing general physical and cognitive impairments.7–9 Despite the well-known positive effects of PA engagement, only 10–30, of older adults report engaging in regular physical exercise as recommended by validated PA guidelines,5,10 and only 36% of older adults are aware of the PA recommendations. 11
Major barriers of regular PA include the lack of time and motivation, physical disorders, presence of chronic diseases, and fear of injuries.12,13 An active lifestyle is associated with the availability and accessibility to activities in the environment in which older adults live. 14 On the other hand, the perception of everyday surroundings as unfavorable for PA can lead to disengagement and insecurity to perform PA, 15 leading to a sedentary lifestyle and physical disabilities. 16
Regular PA practices are related to the development of physical literacy (PL) throughout one's lifespan. PA is defined as “any bodily movement produced by skeletal muscles that requires energy expenditure.” 17 A PA could be an integration of intended and unintended movement, being part of regular daily living activities or physical exercise programs. To further understand PA in terms of motor action outcomes, and broader social, cognitive, and affective processes, PL has been defined as the development of the motivation, confidence, physical competence, knowledge, and understanding to value and engage in a wide variety of physical activities and environments that benefit the person as a whole. 18 Over time, PL levels may fluctuate depending on factors such as age, health status, daily habits, PA engagement, participation in sports, workplace demands, and preferred interests. 19 Although PL may be developed at any age, it typically takes more time and practice for older adults to learn or recover physical and cognitive skills, especially when compared with earlier years.19,20
Exposure to multicomponent physical exercise programs, including aerobics, flexibility, muscle strengthening, and balance training combined with a variety of environments, is recommended for the early development of PL. 21 Early exposure to PA may be effective in establishing lifelong PA participation and preventing several functional declines in later life.22–25 Furthermore, long-term PA engagement is associated with greater odds of successful physical–psychosocial aging. 26 However, the practice of a conventional exercise program is often considered monotonous and boring among older adults, leading to loss of interest and discontinuation of regular engagement. 27 Therefore, effective approaches that emphasize task-oriented training and motivate self-regulated practice are needed to maintain long-term quality of life and functional capabilities.24,25
In this direction, innovative tools for practicing physical exercises and monitoring PA parameters have gained notable research focus as they may represent an alternative to the conventional approach to engaging in healthier lifestyles.28–30 Recent technological advances, such as fitness trackers and virtual reality (VR)-based exercises, have been designed to encourage people to engage in PA. 31 Fitness trackers encompass a broad range of research- and consumer-grade wearable devices worn anywhere on the body. Their potential is amplified by their portability and ability to monitor health and wellness for later life independence.32,33 Not surprisingly, VR has been employed in exercise programs, usually in the form of exergames (or active video games).30,34 Due to exergames' unprecedented capacity to produce auditory and visual sensations, the players feel immersed in VR and can practice PA simulating what they would do in the real world. 35
As an interactive tool, exergaming is perceived as an enjoyable experience that makes the activity more accessible and motivates older adults to engage and adhere to exercise programs.36–38 Evidence supports the use of exergames as rehabilitation tools to improve physical and cognitive functions, such as balance, mobility, muscle strengthening and flexibility, executive function, and processing speed.39–43 Following this, the goal of this study was to evaluate the use of exergames in an exercise program for older adults, and the benefits on their mobility skills, motivation, confidence, knowledge about PA, and daily exertion when compared with a conventional exercise program and no training (NT) (control). We hypothesized that participants allocated to the exergame training (ET) group would experience and retain benefits in each of four PL domains (physical, affective, cognitive, and behavioral), compared with those who performed the conventional training (CT).
Materials and Methods
Experimental protocol
We conducted a single-blind randomized-controlled trial (RCT) study between September and December 2018 at an independent-living center in Calgary, Alberta, Canada. The study addressed the application of Whitehead's PL concept 18 to investigate the effect of exercise training, both exergame and conventional programs, on older adults' physical competence, self-confidence, motivation, knowledge about PA, and daily step count. To measure outcomes, we used the Timed Up and Go Test (TUG), Exercise Confidence Survey (ECS), Motives for Physical Activity Measure-Revised (MPAM-R), Knowledge and Understanding Questionnaire (K&UQ), and total PA tracking (using wearable technology). We chose these measures to correlate with the PL domains: physical (mobility skills), affective (motivation and confidence), cognitive (knowledge and understanding of PA), and behavioral (daily exertion), respectively.
Outcome variables were measured at preintervention (week 0), postintervention (week 6), and at the time of final follow-up (week 9) (Fig. 1). To minimize experimenter bias, the study coordinator (not involved directly with training sessions) administered the surveys, scheduled the order of the assessments, and downloaded the daily exertion data.
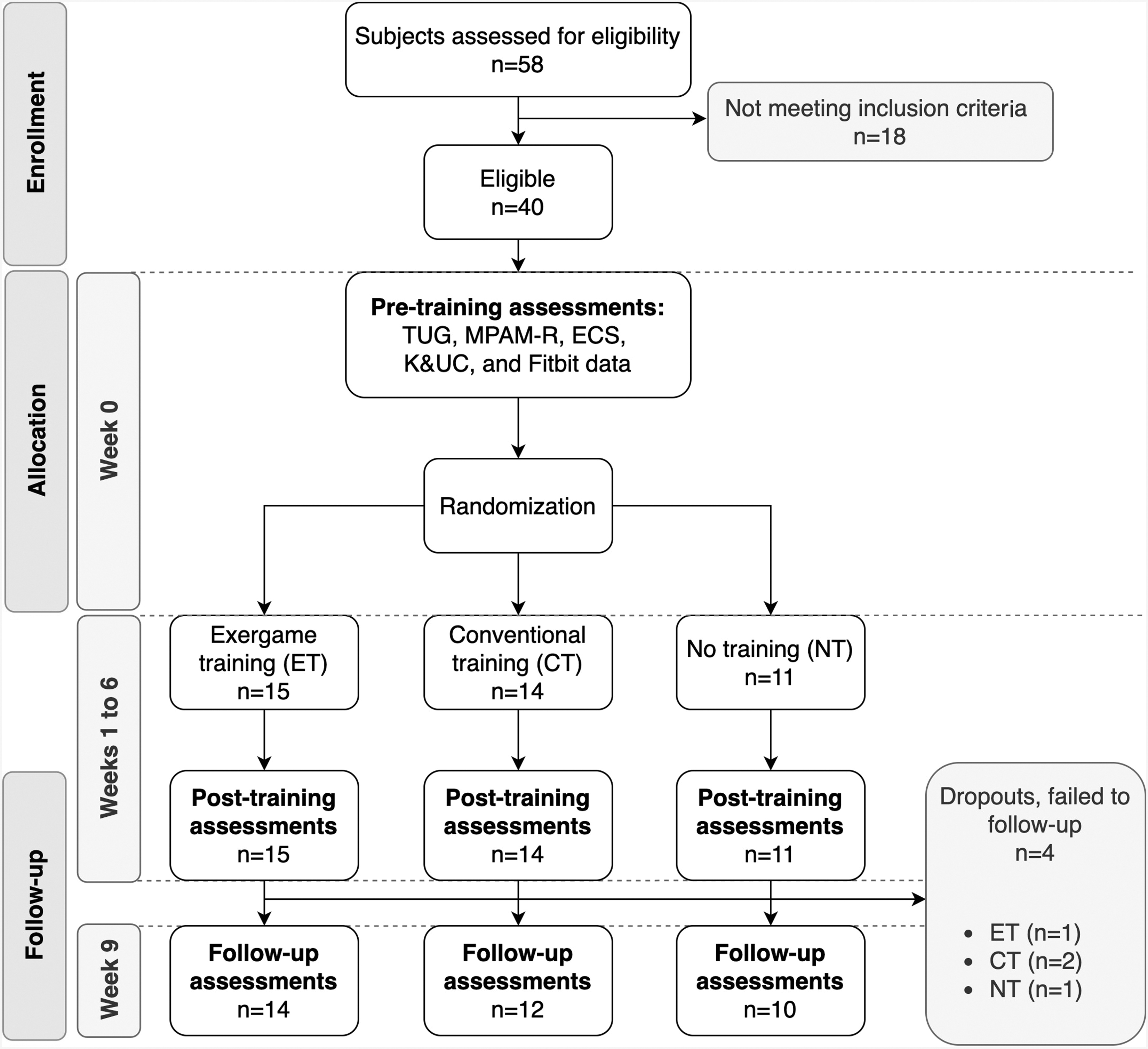
Study flow chart. TUG. MPAM-R. ECS. K&UQ. ET. CT. NT. POST and follow-up assessments were the same as PRE. CT, conventional training; ECS, Exercise Confidence Survey; ET, exergame training; K&UQ, Knowledge and Understanding Questionnaire; MPAM-R, Motives for Physical Activity Measure-Revised; NT, no training; POST, posttraining; PRE, pretraining; TUG, Timed Up and Go Test.
Sample
Older adults (defined as ≥65 years old) were recruited from 15 community centers and 3 retirement facilities. Fifty-eight subjects demonstrated interest in the study. One physical therapist prescreened all subjects using specific guidelines 44 and the Mini-Cog Test for cognitive function assessment. 45 Exclusion criteria were: incapacity to ambulate without an assistive device; balance or neurological disorder(s) (e.g., stroke, traumatic brain injury, spinal cord injury, nerve injury, multiple sclerosis, or parkinsonism); did not present vision and hearing skills compatible with interacting with a videogame; presented with acute/chronic disease (accessed by PARQ-Plus); failed to clear the Mini-Cog Test (score <3); and, took part in a PA program within the last 3 months. After screening, 40 participants (15 males and 25 females) were included in the study (Fig. 1). To maintain allocation concealment, randomized sequences were computer generated, and participants were assigned to one of three groups: ET (n = 15), CT (n = 14), and NT (n = 11). The study was approved by the Research Ethics Board (#REB16-1633) and participants read and signed the agreement consent form.
Demographics
We obtained demographic data at preintervention (week 0) to characterize the sample. This included age (years), sex (male or female), height (cm), weight (kg), and body mass index (BMI; kg/m2).
Physical competence—timed up and go test
TUG is a measure of functional mobility 46 in which the participants start seated on a chair and on the tester's command, they stood up, walked 3 meters, turned around, walked back, and sat down on the same chair. The time taken to complete the task was recorded (Casio HS70W, Tokyo, Japan) and they wore their usual footwear. The TUG is considered a reliable test for older adults, and the general cutoff for fall risk classification is performing below 13.5 seconds.46,47
Confidence—exercise confidence survey
The ECS measures participants' confidence to exercise in a variety of daily life conditions. 48 The 5-point Likert scale (1 = “I know I cannot” to 5 = “I know I can”) consists of 12 items asking participants to rate their exercise confidence. Higher scores indicate higher confidence or self-efficacy. This test is a reliable outcome (Cronbach's α = 0.92). 49
Knowledge and understanding—knowledge and understanding questionnaire
The K&UQ includes seven open-ended questions about knowledge on the appropriate intensity, duration, and frequency of PA for achieving health benefits. 50 Participants answered with numbers in the first 2 questions, and “true/false” or “yes/no” in the following 5 questions (true or yes = 1, false or no = 0). Especially, the first 2 questions were scored ranging from 0 to 2–0 and was given for answers below the expected answer, 1 was given for the expected number, and 2 was given for answers above the expected. The sum of correct responses formed a knowledge score of up to 9 for each participant. A previous study demonstrated high reliability (Cronbach's α = 0.81). 51
Motivation—motives for physical activity measure revised
The MPAM-R is a 30-item questionnaire to assess motivation for PA participation. Participants completed the questionnaire containing five motive subscales: Interest (e.g., “I enjoy this activity”), Competence (e.g., “I like physical challenges”), Appearance (e.g., “I want to improve my appearance”), Fitness–Health (e.g., “I want to maintain my physical strength”), and Social (e.g., “I want to meet new people”). Answers to each item were recorded on a 7-point scale ranging from 1 (“not at all true for me”) to 7 (“very true for me”). The MPAM-R has demonstrated satisfactory reliability for each subscale (Cronbach's α ranging from 0.78 to 0.92). 52
Daily exertion behavior—total physical activity tracking
We provided each participant with a wristband activity tracker (Fitbit Flex 2™; Fitbit, Inc., San Francisco). Participants wore the device on their nondominant wrist (contralateral to the writing hand). Participants were instructed to wear the device for 24 hours a day during the full study period (from week 0 to follow-up measure; see Fig. 1). We provided written and verbal instructions on how to recharge the device overnight twice a week. The device measured daily exertion behavior based on arm movement, and data recordings were transferred through a Bluetooth connection directly to a mobile application. We selected the Fitbit Flex 2 based on a combination of factors, including simplicity, waterproofing, and battery life, to increase total wear time and compliance. 53 Fitbit Flex series has shown to have moderate-to-strong concurrent validity in assessing sedentary behavior (r = 0.90) and moderate-to-vigorous PA (r = 0.65–0.76). 54
Participants in the ET and CT groups downloaded the Fitbit data once a week before the training session. The NT group commuted to a community facility once a week to meet with the research coordinator to download the data but did not have contact with the other groups. Participants did not have access to the data from the Fitbit until the end of the study.
Training programs
Both the ET and CT programs were designed to match the physical demands and were led by two instructors. Exercise training sessions occurred simultaneously in two separate rooms (for ET and CT groups) within the same independent-living center. Participants chose from 1 of the 3 different session times (2 mornings and 1 afternoon). Sessions were conducted three times a week for 6 weeks (a total of 18 sessions). Each session was conducted in small groups of four to five subjects and had a duration of 40–50 minutes. The instructors tried during each session to (1) create a supportive social environment; (2) maximize participants' opportunities to be physically active during the sessions; (3) satisfy participants' needs for autonomy by including elements of choice, when possible; (4) deliver experiences that were fair by allowing all participants to experience success regardless of their capabilities; and (5) ensure the safety of participants by continuous supervision during the exercise sessions. The participants were asked not to enroll in any other structured physical exercise program during the study, but they were allowed to maintain their usual daily activities.
Exergame training
We used a Nintendo Wii-U console to run Wii Fit-U™ games 39 (Nintendo, Kyoto, Japan). We selected and categorized games available into four types: aerobics, strength, balance, and flexibility. Each session comprised an aerobic exergame to warm-up (∼10 min), then participants performed a strength (∼10 min) exergame, balance (∼10 min), and flexibility (∼10 min) exergames (Fig. 2). Games were considered simple and had features that could be easily understood by the participants. 39 Participants used the Wii Balance Board™ and Wii Remote™ to control the game target element shown on the screen while moving on both the sagittal and frontal planes. The initial screen of each game allowed participants to understand the game, what type of body movements were required, and to select the game's difficulty level.
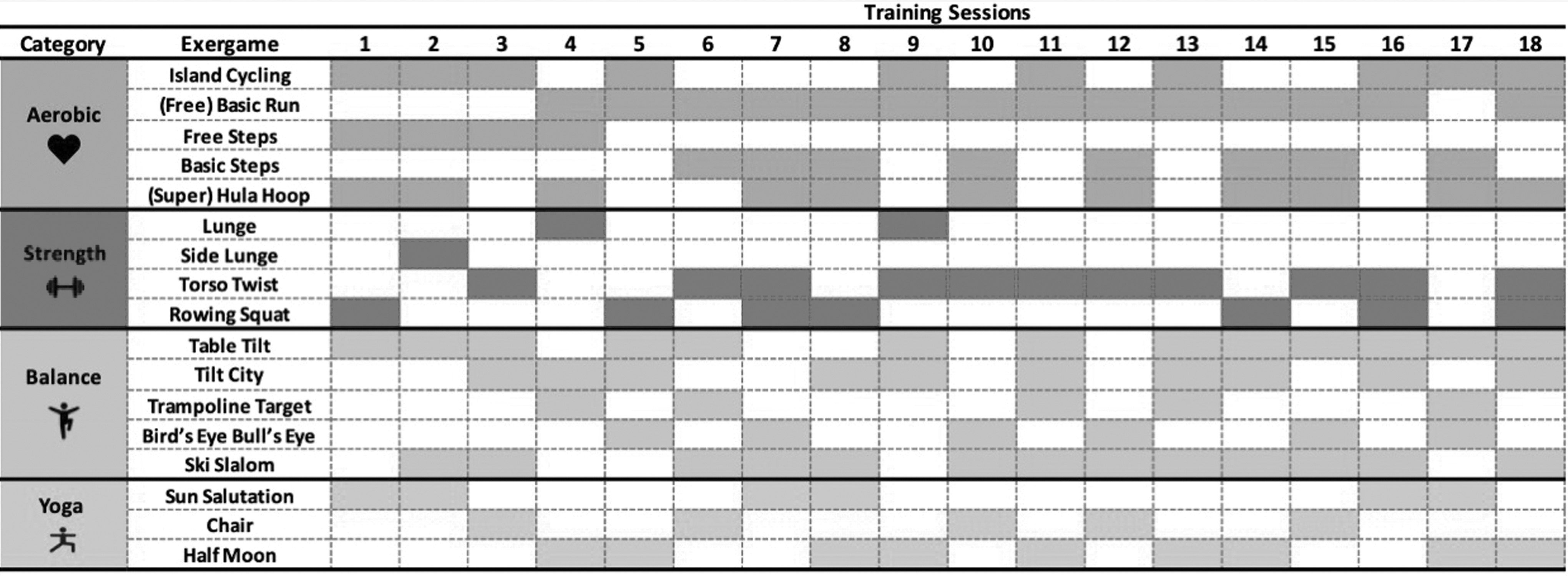
Exergames were used by the ET group during the study by category and each training session. The Wii Fit-U™ games were categorized into four types: aerobics, strength, balance, and flexibility. Each session comprised an aerobic exergame to warm-up (∼10 minutes), then participants performed a strength (∼10 minutes) exergame, balance (∼10 minutes), and flexibility (∼10 minutes) exergames. The shaded rectangles represent the sessions where the exergame was used.
Instructors demonstrated how each game should be played and assisted participants when selecting the game difficulty level to achieve their best performance. Instructors gradually increased game difficulty levels every 2 weeks to achieve a positive effect of the exercise program. However, the actual progression criteria after the first 2 weeks depended on individuals' perception of their physical abilities (e.g., coordination, agility) and performance in the games (e.g., games' score, time remaining to complete the tasks).
Conventional training
The conventional physical training protocol was adapted from guidelines provided by Kisner et al. 55 The CT program consisted of exercises done seated on a chair, standing behind the chair, and laying down on an exercise mat. The exercises followed the same macrostructure used for the ET group (Supplementary Table S1). Each participant established their exercise workload, for example, by using elastic bands and ankle weights to increase resistance and difficulty. However, the instructors tried to increase the difficulty of each exercise every 2 weeks for each subject to keep constant overload for moderate exercise intensity.
No training group
Participants allocated to the NT group were asked not to engage in any organized exercise training, but they were advised to maintain their usual daily routine.
Statistical analyses
The estimated sample of 30 participants (power = 0.80, effect size = 0.5, and type I error = 5%) was calculated assuming three independent groups with three longitudinal measures, using G*Power software V. 3.1.9.6 (Germany). One-way analysis of variance was used to investigate differences among the demographic data. Generalized Estimating Equation (GEE) models were employed to determine the longitudinal effects on each of the dependent variables: TUG, ECS, K&UQ, MPAM-R, and Daily step count. We also analyzed the MPAM-R subscores (Interest, Competence, Appearance, Fitness-Health, and Social) for a deeper understanding of PL's affective domain. GEE models accounted for group (ET, CT, and NT), moment (preintervention, postintervention, and follow-up), and interaction effects. When necessary, we used a posthoc Bonferroni pairwise comparison. The threshold for statistical significance was set to P < 0.05. All statistical analyses were completed using IBM® Statistical Package for the Social Sciences (SPSS) version 23.0.
Results
Demographics
Only the BMI was a significant difference among groups (P = 0.03, Table 1), in which ET (31 kg/m2) presented higher than the other groups (CT: 29 and NT: 26 kg/m2; P < 0.05). Therefore, BMI was treated as a covariate for all GEE models. 56
Demographic Variables
A significant difference in value was highlighted in bold letters.
Values displayed in mean ± SD. ET, CT, and NT groups. BMI.
ET significantly different from CT and NT (both, P < 0.05).
BMI, body mass index; CT, conventional training; ET, exergame training; NT, no training; SD, standard deviation.
Training enrolment
All subjects completed the 6-week program and the postintervention assessment. Mean and standard deviation participant attendance was 15 ± 3 and 15 ± 2 sessions for the ET and CT groups, respectively. Adverse events (e.g., motion sickness or injuries) were not reported during the intervention. In the follow-up assessment (week 9), there were four dropouts (ET: 1, CT: 2, and NT: 1) due to a lack of time commitment and unwillingness to travel to the exercise facility for follow-up. Therefore, the follow-up completion rate was 90% (36/40) (Fig. 1).
Training effects
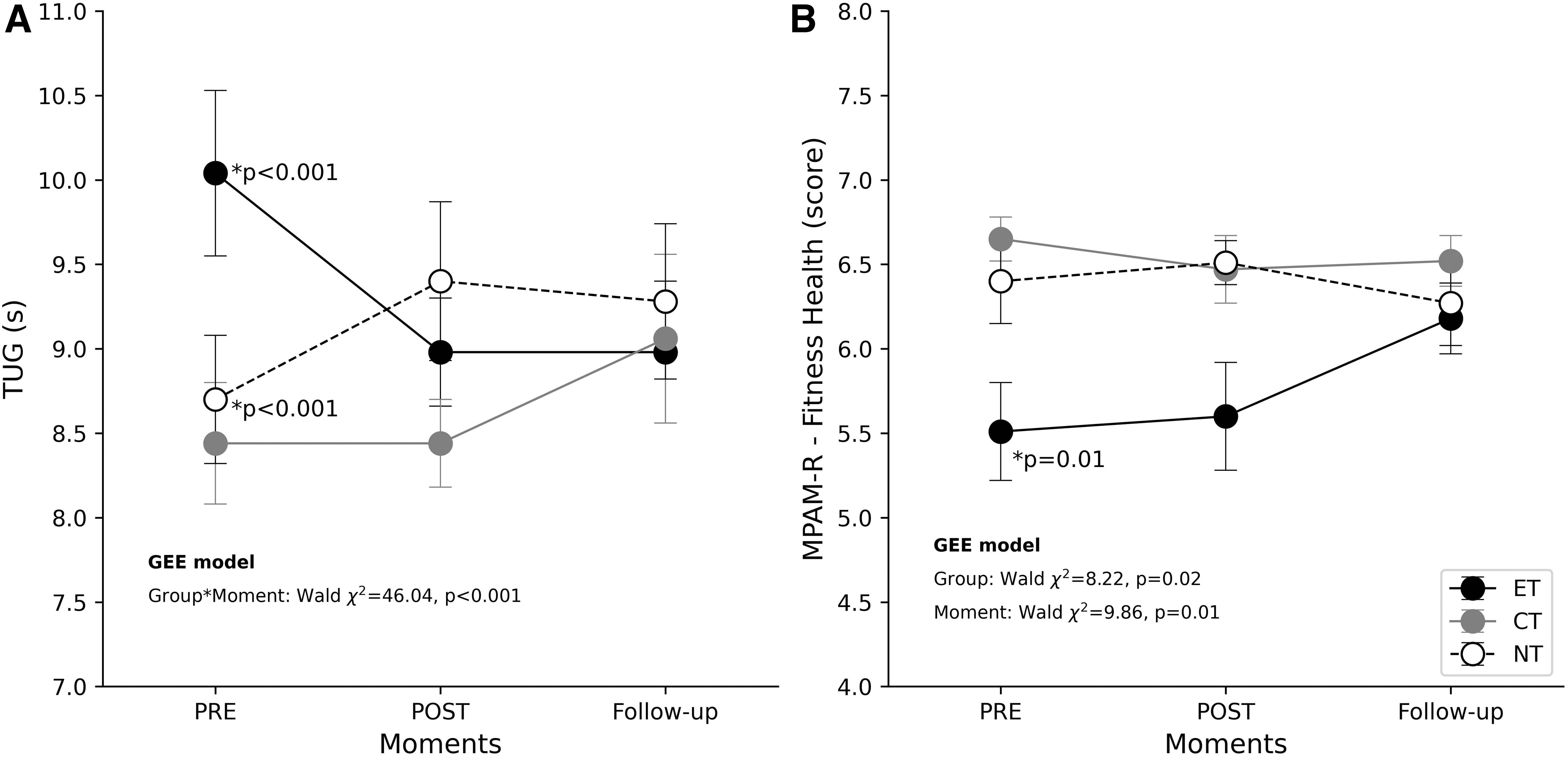
We observed a significant interaction for TUG (Wald χ 2 = 46.04, P < 0.001; Supplementary Table S2). A follow-up within-group comparison revealed significant changes across moments for ET (Wald χ2 = 27.35, P < 0.001; Table 2) and NT (Wald χ 2 = 16.81, P < 0.001; Table 2). Posthoc pairwise comparison demonstrated that the preintervention differed from both postintervention and follow-up assessments (all, P < 0.001; Fig. 3A). However, it should be noted that ET and NT demonstrated opposite behaviors, with ET performance improving (i.e., a lower time) and NT worsening (i.e., a higher time). A group main effect was observed in ECS (χ 2 = 7.81, P = 0.02; Supplementary Table S2). Further posthoc analysis indicated that NT was statistically different (P = 0.02).
TUG and Fitness-Health MPAM-R subscale values across moments. Values in mean ± SD.
TUG, ECS, K&UQ, MPAM-R, and Daily Step Count of Each Group, and Comparison Within Groups by Phases of the Study
Values displayed in mean ± SD. TUG. ECS. K&UQ. MPAM-R. ET, CT, and NT groups. Significant P-values are highlighted in bold. Each variable was adjusted for BMI (covariate).
ECS, Exercise Confidence Survey; K&UQ, Knowledge and Understanding Questionnaire; MPAM-R, Motives for Physical Activity Measure-Revised; TUG., Timed Up and Go Test.
Regarding the MPAM-R subscore values, only the Fitness-Health subscore demonstrated a significant main effect for group (Wald χ 2 = 8.22, P = 0.02; Supplementary Table S3) and moment (Wald χ 2 = 9.86, P = 0.01; Supplementary Table S3). Further posthoc analysis indicated that the ET and CT Fitness-Health subscores were statistically different (P = 0.01). The within-group comparison showed significant differences in the ET Fitness-Health subscore from preintervention to postintervention and follow-up (both, P = 0.01; Fig. 2B and Table 3). We did not observe any other significant difference.
MPAM-R Subscale Values and Comparison of Each Group, and Comparison Within Groups by Phases of the Study
Values displayed in mean ± SD. MPAM-R. ET, CT, and NT groups. Significant P-values are highlighted in bold. Each variable was adjusted for BMI (covariate).
Discussion
This was an RCT aiming to compare the effects of an exergame-based program to a conventional exercise program with a NT control on each of the four PL's domains in healthy community-dwelling older adults. Our results suggest that a 6-week exergame-based exercise program was able to improve the physical and affective PL domains measured through TUG and MPAM-R Fitness-Health subscore, respectively.
An improvement in TUG performance in older adults after an exergame-based exercise program is in line with the findings of a systematic review. 43 An improvement in TUG performance may be linked to increased self-confidence and reduced fear of falling.57,58 Also, self-confidence can improve by gaining an understanding of technological devices and through performance in novel activities, such as the Nintendo Wii games.59,60 In fact, increases in self-confidence in healthy community-dwelling older adults after a 12-week exergame intervention was previously reported. 61 However, we did not find differences in subjects' ECS or K&UQ scores, therefore, we cannot directly relate physical improvement with increased self-confidence in our study. Intervention length may be partially responsible for the contrasting results between the present and the Williams et al. 61 study, suggesting that a longer exergame-based exercise program intervention period may be necessary to improve self-confidence in older adults.
Derakhshanrad et al. 62 suggested that PA engagement by older adults is often due to extrinsic goals, such as wellness and socialization. As exergames are interactive, challenging, competitive, and more rewarding than conventional exercise programs, they can motivate older adults.63,64 Moreover, the fun and entertaining capacity that exergames' interactive environment provides, as well as the immediate performance feedback, may keep participants motivated to continue engaging in PA.65,66 Altogether, this can create a context to foster autonomy and perceived competence, which may enhance enjoyment and sustained motivation.67–70 Although we did not observe differences in the MPAM-R total score, the ET group significantly improved their MPAM-R Fitness-Health subscore suggesting that a 6-week exergame-based exercise program was able to increase the motivation toward engaging in PA due to fitness and health-related subjects. This is relevant information that can orientate future studies and/or PL programs for older adults. Topics related to fitness and health can be used as a starting point to interact and develop programs, not just to improve motivation toward PA, but in other PL's domains as well.
It is believed that increased extrinsic motivation to be fit and healthy, and the enjoyment of peer socialization while engaging in PA, may contribute to a higher adherence rate to exercise programs. 71 However, we did not observe increases in the MPAM-R Social subscale for any of the training groups. Considering exergame as a tool to engage in exercise, the social aspect cannot be left out. By concept, VR games insert humans (the player) into a virtual world, which can be experienced with or without interaction with other players, either in-person or virtually. Our exercise program was delivered in small group sessions (four to five subjects), creating an intrinsic environment for social interaction. The lack of significant change on the MPAM-R Social subscale may be partly attributed to the short training period (6 weeks). Researchers and PA providers should keep the length of intervention in mind when designing exergame-based programs and create strategies to facilitate social interaction. Examples include creating group activities to be in place or virtual rooms with peers of the same age to improve communication using online text/audio chats or similar technology.
Adherence, and its subsequent beneficial effects, is a challenge to implementing exercise programs for older adults.72–74 While the exercise training schedule in the present study requiring 3 days of weekly attendance for 6 weeks, attendance by the ET group (80.5%) was in line with previous studies.75,76 Participants in our study attended nearly all offered sessions and had no adverse events, indicating that the Nintendo Wii Fit subgames and their difficult progression were engaging and feasible in their routines.
Interestingly, even with the physical and affective PL domain enhancement observed by the subjects, we did not find changes in the daily step count (behavior domain) for any moment during the study. In other words, only providing a structured exercise program (exergame or conventional) did not produce changes in the volitional daily exertion. However, it should be noted that the subjects were instructed to not change their normal activity level during the whole study. This strict direction may have limited behavioral changes noticed in the follow-up.
PL is an inclusive and holistic concept 77 and should be considered as a framework to implement and control training programs beyond the physical aspects related to exercise. Although the concept has reached widespread attention in academia, its discussion has been limited to the philosophical sphere.78,79 We agree that a deep understanding of PL's philosophical foundations is important; however, a pragmatic perspective reflecting whether individuals are making progress along their PL journey enables researchers and practitioners to operationalize PL's domains and establish measurable differences in specific populations. 79 In this context, the present study demonstrates a replicable design encompassing all four described domains of PL in older adults.
Incorporating fitness and health topics into programs designed to improve older adults' PL can significantly impact their overall wellbeing. Exercise programs aimed at enhancing PL can include a variety of activities, such as strength training, aerobic exercises, and balance training using both conventional and exergame approaches. In addition, the inclusion of health topics, such as nutrition, stress management, and disease prevention, can help older adults maintain a healthy lifestyle. By providing education and practical strategies for incorporating PA and healthy habits into their daily lives, programs designed to improve PL can help older adults maintain their independence, reduce their risk of chronic disease, and enhance their overall quality of life. Furthermore, incorporating fitness and health topics into PL programs can promote socialization and community engagement, providing older adults with a sense of purpose and belonging. 80 Future studies could investigate the effectiveness of incorporating these aspects into exercise programs in improving PL and overall wellbeing in older adults.
This study has some limitations. Despite the randomization and allocation concealment processes, the ET group's BMI was higher. We addressed this problem by considering the BMI as a covariate in our statistical models. Additionally, ET group began the study with a higher TUG time, despite the randomized allocation of participants. While some may argue that this initial difference could potentially inflate the observed benefits in the physical domain for the ET group, it is important to highlight that the statistical model used in our study is robust enough to account for such differences. The training duration and the short period between postintervention and follow-up assessments might be a partial limitation. It is possible that the timeframe was not long enough to develop and produce observable changes in the self-reported instruments used. Although the subjects demonstrated good adherence to the training program, we observed a few dropouts in the follow-up testing. The follow-up testing was scheduled in early December when the average temperature was colder and snow precipitation was higher compared with the beginning of the study.
Participants may have faced difficulties due to different weather conditions to travel to the facility. Finally, the participants in the ET or CT group were free to choose a session that best suited their schedule. Although the group session structure facilitated direct contact between participants within their respective groups during the training session, we cannot guarantee that they interacted and shared feedback on their training routines outside of the sessions. Despite not having control over this, we did not observe any participants commenting on the group allocation or about differences in the training routine during the study. Additionally, the group that did not receive any training (i.e., NT group) did not have any interaction with the training groups during the training period.
Conclusion
Our study provides preliminary evidence that a 6-week exergame-based training program may have the potential to improve the physical and affective domains of PL in community-dwelling older adults. These findings suggest that exergames could be a promising tool for promoting PL in older adults. However, we suggest caution in generalizing these findings to the entire senior population due to the limitations of our study. Future research should aim to provide ecological validity and confirm the potential benefits of exergames for long-term PL development, promoting healthier exertion behaviors, and preventing health disorders in older adults. Nonetheless, our study highlights the relevance of incorporating fitness and health topics in programs designed to improve older adults' PL.
Footnotes
Authors' Contributions
A.M.C. helped devise the study, collected the data, analyzed the data, interpretated the outcome, and drafted the article. A.W. facilitated participant recruitment, managed participant activities and information, coordinated data collection, provided wearable data, and contributed to the literature review and discussion. D.S. provided valuable insights into the project plan, helped supervise the project, and edited the article. K.S. provide detailed feedback, new approaches to understanding the data, and helped edit the article. V.R.A.C. helped with the literature review, data analysis, and interpretation. L.K. devised the study, supervised the study, provided feedback on the process, helped conceptualize the data analysis, and edited the article. All authors have read and approved the final version of the article and agree with the order of presentation of the authors.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.