
Abstract
Laboratories are increasingly required to perform molecular tests for the detection of mutations in the KRAS gene in metastatic colorectal cancers to allow better clinical management and more effective treatment for these patients. KRAS mutation status predicts a patient's likely response to the monoclonal antibody cetuximab. To provide a high standard of service, these laboratories require external quality assessment (EQA) to monitor the level of laboratory output and measure the performance of the laboratory against other service providers. National External Quality Assurance Services for Molecular Genetics provided a pilot EQA scheme for KRAS molecular analysis in metastatic colorectal cancers during 2009. Very few genotyping errors were reported by participating laboratories; however, the reporting nomenclature of the genotyping results varied considerably between laboratories. The pilot EQA scheme highlighted the need for continuing EQA in this field which will assess the laboratories' ability not only to obtain accurate, reliable results but also to interpret them safely and correctly ensuring that the referring clinician has the correct information to make the best clinical therapeutic decision for their patient.
Introduction
T
The increased clinical request for molecular testing for mutations in the KRAS gene in patients with colorectal tumors highlights the need for standardization of testing, the need for published guidelines for the process, and the need to provide laboratories with an external measure of the quality of their service. To address this final issue, a pilot external quality assurance (EQA) scheme was offered during 2009 by the United Kingdom National EQA Services (UK NEQAS) for Molecular Genetics. This EQA provider has been offering laboratories molecular genetic testing EQA schemes since 1991 (Ramsden et al., 2006) and has full EQA scheme accreditation status (Clinical Pathology Accreditation UK Ltd.). The provider is a part of the UK NEQAS umbrella organization operating under the UK NEQAS Code of Practice (www.ukneqas.org.uk). All laboratories participated under the UK Joint Working Group for Quality Assurance Conditions of Participation (www.rcpath.org).
Participants
UK laboratories providing molecular testing of the KRAS gene for mutations in metastatic CRC and all laboratories registered with the UK NEQAS for Molecular Genetics website were invited to participate in the pilot EQA scheme. Enquiries from other interested laboratories were received. Participant numbers were limited to 19 laboratories, because there was no previous experience of the workload involved in providing this pilot scheme and it was preferable to provide a high standard of EQA scheme with sufficient suitable validated EQA material than have large participant numbers.
The pilot scheme was administrated using the UK NEQAS for Molecular Genetics website (www.ukneqas-molgen.org.uk).
Materials and Methods
Each participating laboratory was supplied with EQA material for three clinical cases. The majority of diagnostic samples routinely tested for KRAS mutations are paraffin-fixed biopsy colorectal samples (95%) (Source BioScience laboratory data). Therefore, to ensure the samples distributed to participants reflected the clinical samples received for testing as closely as possible, biopsy samples were sourced.
Testing laboratories routinely receive samples in different formats, so participants were given the choice as to which type of sample they would prefer, and as far as possible, this request was met. The samples distributed for each case were either (i) four sections of 4 μm paraffin-embedded tumor tissue, (ii) four sections of 4 μm paraffin-embedded tumor tissue plus a slide-mounted paraffin section of tumor tissue, or (iii) three slides of mounted 4 μm paraffin section of tumor tissue.
Table 2 summarises the type of samples distributed. To reflect the processing of samples and reporting of samples within the laboratory, the EQA samples were assigned hypothetical patient names and dates of birth. This information was randomly created, did not resemble any known individual, and did not correspond to the source of the tissue samples.
The tumor tissue available for this pilot scheme was limited; therefore, two different tissue samples were used for each clinical case. The samples selected were of the same genotype so that the same KRAS genotype was distributed to participating laboratories for each case. The samples were also selected for a similar ratio of tumor cells to normal cells across the tumor block so that differences in tumor cell levels would not account for any discrepant results reported by participants. Table 2 details the sample type distributed.
Material was stored from all EQA cases for internal quality control purposes.
Sample validation
The genotype of the samples for EQA use was confirmed by two independent diagnostic laboratories before distribution. To prevent any errors, the samples destined for the pilot EQA were received centrally, coded, and dispatched for validation. The coding of samples and the validation of more than the required number of EQA samples ensured that the validating laboratories were not aware which samples would be used for the EQA scheme and, therefore, did not have an advantage during the scheme from acting as a validating center.
All samples were screened for changes in KRAS codons 12, 13, and 61 by pyrosequencing (Ogino et al., 2005; Cross, 2008; Dufort et al., 2009). The sensitivity of pyrosequencing for KRAS mutations determined in the validating laboratories is ∼5% for detection of tumor-specific mutations in a background of normal DNA. This is in agreement with cell line dilution studies (Ogino et al., 2005; Dufort et al., 2009).
Validating laboratory 1 testing methods
Pyrosequencing of codons 12 and 13 and codon 61. 10 ng tumor DNA amplified using F and R primers in MegaMix GOLD (Microzone Ltd.) for 38 cycles annealing at 60°C.
Primers: 12/13F 5′-GGCCTGCTGAAAATGACTGA-3′, 12/13R 5′-AGAATGGTCCTGCACCAGTAATA-3′, 12/13 pyrosequence primer 5′-CTTGTGGTAGTTGGAG-3′; 61F 5′-TGTTTCTCCCTTCTCAGGATTC-3′, 61R 5′-AAGAAAGCCCTCCCCAGTC-3′, 61 pyrosequence primer 5′-GGATATTCTCGACACAGC-3′. Pyrosequence analysis on a Pyromark Q24 (Qiagen). Figure 1 shows the results obtained for Case 1.
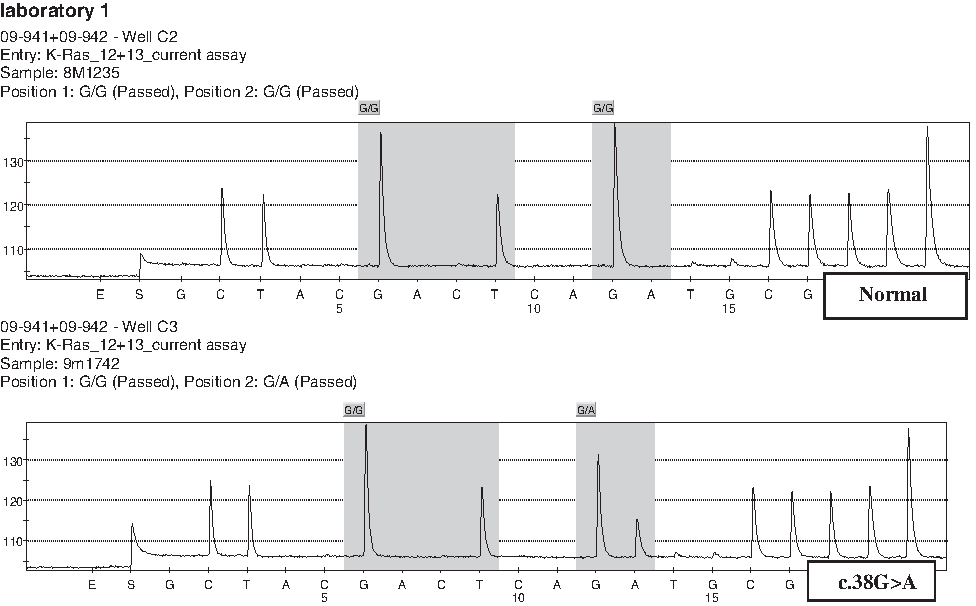
Results for Case 1 by pyrosequencing performed by validating laboratory 1.
Validating laboratory 2 testing methods
Pyrosequencing of codons 12 and 13 and codon 61 was carried out using the Qiagen Pyromark Q96 KRAS v 2.0 primers (Qiagen). PCR was performed using Hotstar taq (Qiagen) in a 25 μL reaction volume (Polymerase chain reaction [PCR] Buffer 1×, MgCl2 1.5 mM, deoxyribonucleotide triphosphates (dNTPs) 0.2 mM, PCR primer, 0.5 μL of each primer, and HotStar Taq DNA Polymerase 0.8 U) with 1 μL of each DNA sample per PCR (DNA extracted using QIAamp DNA FFPE Tissue Kit and eluted in a 30 μL volume). Each PCR underwent 38 cycles with an annealing temperature of 53°C. Pyrosequencing was subsequently performed on the PSQ96 (Qiagen) as per manufacturer's instructions. Figure 2 shows the results obtained for Case 3.
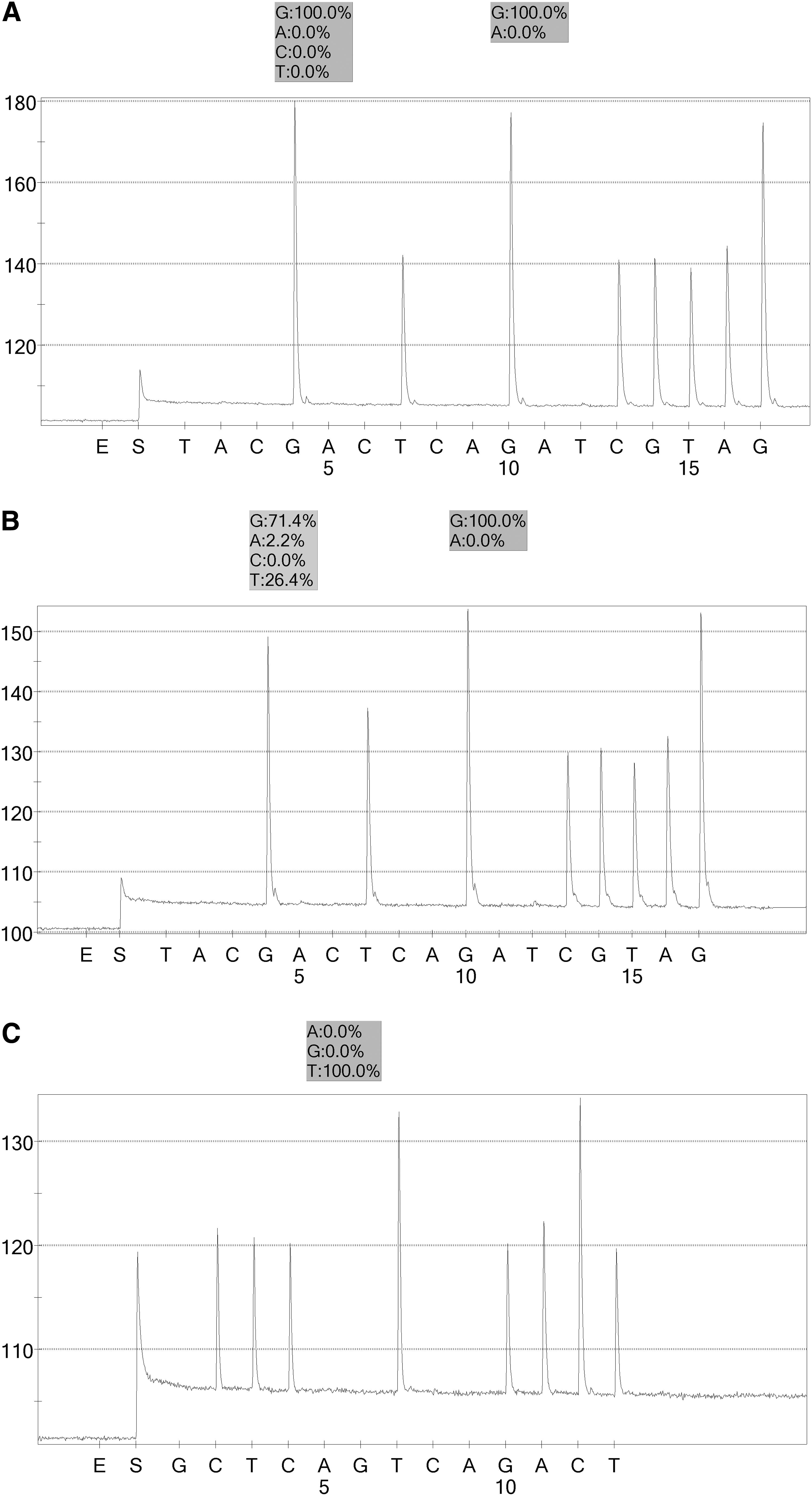
Results for Case 3 by method performed by validating laboratory 2.
The estimated tumor burden was assessed by one validating laboratory. A haematoxylin- and eosin-stained slide was prepared for each sample and assessed by a consultant histopathologist to estimate and indicate the region of tumor cells and to estimate the percentage of tumor nuclei within that region. This assessment acted only as a guide.
Table 3 summarises the validation results of the samples used for this pilot scheme. All genotyping results were concordant. Only the scheme organizer was privy to the expected results for the scheme.
Scheme testing format
Participants were required to test the samples supplied for changes in the KRAS gene according to normal laboratory procedures and to report the results in their usual report format or as genotyping results. They were given a testing period of 8 weeks. All results were submitted electronically.
EQA result assessment
All participant submissions were marked by two independent molecular genetic assessors against marking criteria ratified by peers. Submissions were identifiable only by the unique laboratory code. Each case was allocated 2.0 genotyping marks. An incorrect genotype resulted in a deduction of 2.0 marks for that case. The mean genotyping score for the three clinical cases was calculated for each participating laboratory.
Results
Eighteen out of the 19 participants were able to submit results within the allotted testing period. The laboratory that failed to submit results was in the process of developing their method and registered for the EQA to receive samples to aid their development work. They declined the offer of an independent assessment of their results.
Seventeen out of 18 participants submitting results reported the correct genotype for all three cases. Table 4 lists the participant scores.
One laboratory failed to detect the c.[35G>T] mutation in the sample supplied for Case 3. This false negative result arose from inexperience of the pyrosequencing software user; and as a result, the internal checking procedures within this laboratory have been assessed and amended to prevent a similar event occurring in the future.
Participant feedback
On completion of the marking process, all participants were provided with an individual laboratory score report detailing the genotyping scores assigned for each case, the mean genotyping score for the pilot scheme, and any comments made by the two assessors on their EQA returns. In addition, a full detailed scheme report was published and made available to all scheme participants.
Discussion
The original format of this pilot EQA was to assess the interpretation of the results and the genotyping accuracy. However, the content and standard of the reports submitted varied greatly with some laboratories submitting full clinical reports and others supplying tabulated genotyping results. Hence, the Scheme Assessors felt that the large variation in reporting formats made assessing interpretation difficult in this first pilot distribution. The wide range of interpretative content in the EQA reports indicated the need for clear guidelines for best practice for testing and reporting for KRAS analysis in CRC.
The genotyping results were assessed, and the KRAS mutations were reported using many formats. The HGVS (Human Genome Variation Society) format for the reporting of mutations is internationally recognized and should be used for the reporting of all mutations (see www.hgvs.org/mutnomen/). Table 5 gives a summary of the nomenclature used and the correct HGVS nomenclature. Only eight out of 18 laboratories used the correct HGVS nomenclature. Had the scheme been marked for interpretation, many of the participating laboratories would have lost marks for not using the correct mutation nomenclature.
Mutations in codons 12 and 13 are in exon 1.
HGVS, Human Genome Variation Society.
When mutation nomenclature is stated, then a reference sequence should be provided so that the correct site of the mutation can be identified. Only four out of 18 laboratories providing returns stated a reference sequence for the KRAS gene. The reference sequences that were quoted all corresponded to an appropriate KRAS sequence.
The most commonly used method of analysis was pyrosequencing (Ogino et al., 2005; Cross, 2008) of codons 12, 13, and 61 of the KRAS gene (see Table 6). The remaining laboratories performed a range of methods including commercially available kits, for example, DxS KRAS Therascreen kit (Qiagen), Amplification Refractory Mutation System-PCR (Amplification Refractory Mutation System analysis using primers specific for mutant or wild-type DNA sequences) (Newton et al., 1989), and high resolution melt or restriction fragment length polymorphism analysis followed by DNA sequencing. This pilot EQA was not prescriptive as to which method should be employed, as it is important for the scheme to assess the output of the laboratory and not their ability to meet the criteria of EQA scheme participation. Three participants did not state their methodology in the submitted reports.
PCR, polymerase chain reaction.
The scheme also did not specify which codons of the KRAS gene should be tested for mutations. Rather, the participants were requested to perform their routine testing protocol to assess the routine practices of the laboratory. The majority of participants tested the region encoding codons 12 and 13 of the KRAS gene. Other areas such as codons 59 and 61 were also analyzed (see Table 6). Mutations are reported to be present at 77% in codon 12, 17% in codon 13, and 5% in codon 61 in colorectal tumors (All Wales Molecular Genetics diagnostic laboratory data on over 1000 metastatic colorectal samples analyzed). There are currently no best practice guidelines that determine which codons or mutations should routinely be assayed.
UK NEQAS for Molecular Genetics provided a successful external quality assessment pilot scheme for the molecular analysis of KRAS gene in metastatic CRC during 2009. There was a considerable demand from both molecular genetic regional diagnostic laboratories and histopathology laboratories to provide such an assessment and since the completion of the scheme, more interested laboratories have applied for participation in future schemes. Therefore, there is a demand for more EQA in this field.
Future schemes will be improved by identifying a source of tissue in order to provide more EQA material to meet the increasing number of participants. This increase in the number of potential participants was highlighted by the proposal for a European wide EQA program to meet the need to standard the KRAS molecular testing across Europe (van Krieken et al., 2008).
It is important for EQA schemes to assess the whole testing process, which, in this case, involves not only the reporting of the genotyping result but also the interpretation of that result. Future schemes will require participating laboratories to submit their routine reports and both the genotyping and the interpretation of the result will be scored. This will provide the participants with a method by which to monitor their own performance and an external measure of the standard of service they provide against other service providers in this field. Further, the publication of international best practice guidelines would be beneficial to all laboratories providing a KRAS molecular testing service and would enable EQA schemes to assess against an agreed standard of service.
Notes
All mutation nomenclature stated in this article is according to GenBank accession number NM_004985.3 with numbering starting at the A of the ATG initiation codon.
Footnotes
Acknowledgments
The authors would like to thank all patients and clinicians who supplied the clinical material, also Tom Burr, Jane Bell, and Kevin Chittock for their contribution and helpful discussions. They express their gratitude to the All Wales Molecular Genetics diagnostic laboratory, Cardiff for their help in sourcing the EQA material, and Northern Genetic Service, Newcastle upon Tyne, for hosting the UK NEQAS scheme. The authors would like to thank UK NEQAS for Molecular Genetics Steering Committee for their advice and support of this pilot EQA.
Disclosure Statement
No competing financial interests exist.