
Abstract
Aim:
This study was carried out to evaluate the association of genetic polymorphism −670A>G in the promoter of Fas gene as well as serum biomarkers aspartate aminotransferase (AST) platelet ratio index (APRI) and AST/alanine aminotransferase (ALT) with significant fibrosis and cirrhosis in chronic hepatitis C patients. Seventy-nine patients with chronic hepatitis C in addition to 80 age- and sex-matched healthy controls were evaluated for genetic polymorphism −670A>G of Fas gene by polymerase chain reaction-restriction fragment length polymorphism and serum biomarkers APRI and AST/ALT in relation to significant fibrosis and cirrhosis diagnosed by liver biopsy.
Result:
Genetic polymorphism −670A>G in Fas gene was associated with significant liver fibrosis and cirrhosis. Heterozygous mutation was found in 11.4% of patients and 10% of controls, while homozygous mutation was found only in 7.6% of patients. Odds ratio (OR) was statistically not significant (OR=1.93, 95% confidence interval=0.76-4.92). Mean values of APRI and AST/ALT were significantly higher in patients with (F3-F4) compared with those with (F0-F2). (p-value <0.001 for APRI and p=0.007 for AST/ALT). In addition, APRI showed a better sensitivity than AST/ALT for prediction of significant fibrosis.
Conclusion:
Genetic polymorphism −670A>G of Fas gene was associated with significant fibrosis and cirrhosis in chronic hepatitis C patients. APRI and AST/ALT are independent predictors for significant fibrosis. APRI showed a better sensitivity than AST/ALT for prediction of significant fibrosis. Moreover, APRI can be used as an index to exclude liver cirrhosis without performing liver biopsy.
Introduction
H
The Fas ligand (Fas L) is a cellular surface molecule that belongs to the tumor necrosis factor family. It induces apoptosis by binding to its receptor Fas on Fas bearing cells. Various cells express Fas, while Fas L is expressed predominantly in activated T-cells (Shigeka et al., 1995). Fas is constitutively expressed in every cell in the liver rendering all liver cells sensitive to Fas-mediated apoptosis in vivo. During infection with HCV, infiltrating cytotoxic T lymphocytes recognize and kill viral antigens expressed on infected hepatocytes through the Fas-Fas L pathway. However, excessive or defective Fas mediated apoptosis leads to liver failure, fibrosis, and carcinogesis (Tobi et al., 2001; Jarmay et al., 2002). Recently, Fas expression was reported to be increased in the liver of patients with chronic hepatitis C and to be directly correlated with disease activity (Anguilar et al., 2005).
Liver biopsy is still considered the gold standard for staging fibrosis in chronic liver disease and selecting antiviral treatment candidates. However, liver biopsy is an invasive procedure, and complications occur in 0.6%-5% of patients (Hubscher, 1998; Gebo et al., 2002). Recent studies involving patients with chronic hepatitis C showed that the accuracy of histological assessment of necroinflammation and fibrosis depends on the size of specimens; the rate of diagnostic error varied from 10% to 30% in different studies. Another shortcoming of liver biopsy is its cost, as it always requires hospitalization for 6-18 h (Wong and Koff, 2000; Colloredo et al., 2003). For all these reasons, an increasing number of studies are being conducted in order to evaluate the effectiveness of noninvasive markers including two indices aspartate aminotransferase (AST) platelet ratio index (APRI) and AST/alanine aminotransferase (ALT) for the staging of liver fibrosis.
Based on these data, our study aimed at evaluating the association of genetic polymorphism-670A>G in the promoter region of the Fas gene and serum biomarkers APRI and AST/ALT with significant fibrosis and cirrhosis in patients with chronic hepatitis C.
Material and Methods
This study was performed at the Alexandria Main University hospital on 79 patients with chronic hepatitis C. All patients were seropositive for circulating HCV Abs with detectable serum HCV RNA by reverse transcriptase-polymerase chain reaction (PCR). Patients co-infected with HBV and those who received antiviral therapy within the previous 6 months were excluded from study. The control group included 80 HCV negative healthy subjects.
Informed consent was obtained from patients before the start of the study, and the study was approved by the Ethics Committee of the Faculty of Medicine, Alexandria University.
All subjects under study were subjected to the following procedures:
• Full history taking • Complete clinical examination with stress on jaundice, palmar erythema, clubbing, tremors, lower limb oedema, and splenomegally. • Laboratory investigations included A. Complete blood count using Sysmex XT-1800 (Siemens Health care Diagnostics, Inc.). B. Complete liver function tests, including ALT, AST, gamma glutamyl transferase (GGT), alkaline phosphatase, albumin, and bilirubin, were done by Dimension RXL chemistry auto analyzer; prothrombin time was done by Sysmex CA-1500; and alpha-fetoprotein was done by chemluminescence using Advia Centaur analyzer (Siemens Health care Diagnostics, Inc.). C. Evaluation of serum biomarkers, including 1. APRI calculated as follows:- AST/upper limit of normal for AST/platelet count (×109/L)×100. (Carey and Carey, 2010). 2. AST/ALT ratio D. Molecular detection of −670A>G polymorphism in the promoter region of Fas gene by PCR-restriction fragment length polymorphism: Genomic DNA was extracted from whole blood using E.Z.N.A. blood DNA kit (OMEGA Bio-tek). PCR was performed using the following set of primers. Fas-670F5′ CTA CCT AAG AGC TAT CTA CCG TTC3′. Fas-670R5′ GGC TGT CCA TGT TGT TGT GGC TGC3′ PCR was performed using 35 cycles as follows: Initial denaturation at 94°C for 1 min, annealing at 55°C for 1 min, extension at 72°C for 1 min, and final extension at 72°C for 10 min. PCR products were digested with 0.5 μL of ScrF1 at 37°C for 2 h and run on 2% agarose gel stained with ethidium bromide. Wild-type allele (A) produced a DNA fragment of 331 bp. Mutant G allele produced two fragments, 233 and 98 bp (Farre et al., 2008). E. Liver biopsy: was done only for the patients under study as a gold standard for staging of liver fibrosis and cirrhosis. Using Metavir's scoring system, liver fibrosis was staged on a scale of F0-F4: F0, no fibrosis; F1, portal fibrosis without septa; F2, few septa; F3, numerous septa without cirrhosis; F4, cirrhosis. Significant fibrosis was considered as fibrosis staging of at least F3 and cirrhosis staging as F4 (Carey and Carey, 2010).
Statistical analysis
Data were analyzed using SPSS V (15) computer program.
Quantitative data were presented as mean, standard deviation, and paired student t-test.
The nonparametric Mann-Whitney test was done to evaluate the mean values of APRI, AST/ALT in patients with (F0-F2) compared with those with (F3-F4).
Receiver-operating characteristic (ROC) curve analysis was constructed by the Medcalc computer program to find the risk of disease among the proportion of patients having certain determinant or allele.
The Monte-Carlo test was done to find the association of −670A>G polymorphism in the Fas gene with significant fibrosis and cirrhosis.
The level of significance adopted was ≤0.05 for all statistical tests (Wallach, 2000).
Results
The age of patients under study ranged from 30 to 66 years with a mean of 54.9±7.9, and the age of the control group ranged from 33 to 65 years with a mean of 52.9±7.1 years.
Table 1 represents a comparison between patients with chronic hepatitis C and controls regarding complete blood picture and liver function tests. Significant liver fibrosis by Metavir's scoring system (F3+F4) was observed in 33 (41.8%) patients. while liver cirrhosis (F4) was observed in 10 (12.66%) patients.
p is significant if <0.05.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma glutamyl transferase.
Mean values of APRI and AST/ALT were significantly higher in patients with (F3-F4) compared with those with (F0-F2). (p-value <0.001 for APRI and p=0.007 for AST/ALT). The cut-off value of APRI was calculated from ROC curve and proved to be 1.3 for predicting significant fibrosis and 3.43 for predicting actual cirrhosis. Sensitivity and specificity of APRI were 93.4% and 89.7% for predicting significant fibrosis and 88.9% and 99.3% for predicting liver cirrhosis, respectively. The area under the receiver operating characteristic curve (AUROC) was 0.973 for predicting significant fibrosis and 0.97 for predicting liver cirrhosis as shown in Figures 1 and 2.
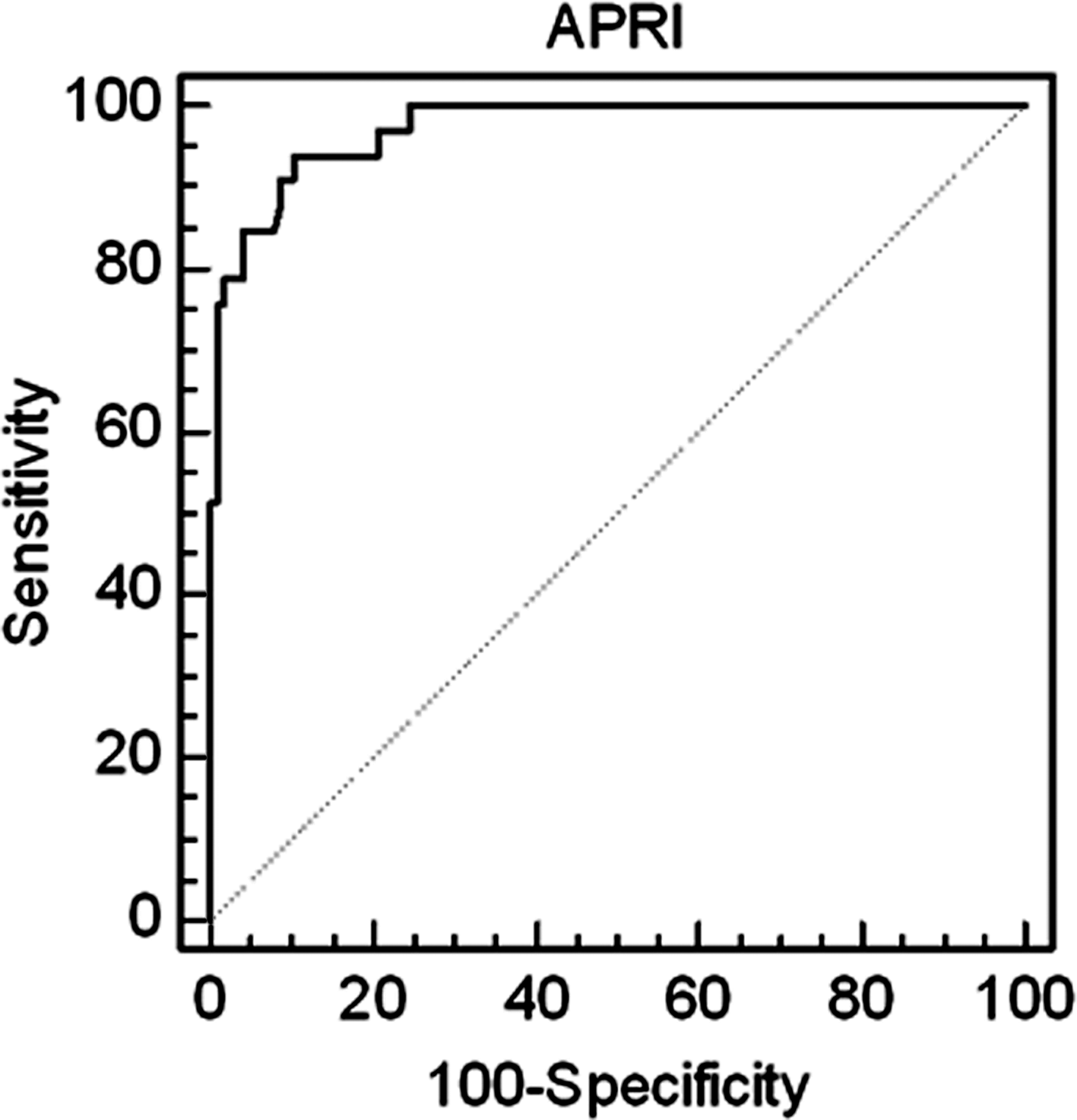
Receiver-operating characteristic (ROC) curve of AST platelet ratio index (APRI) for prediction of significant fibrosis in chronic hepatitis C patients.
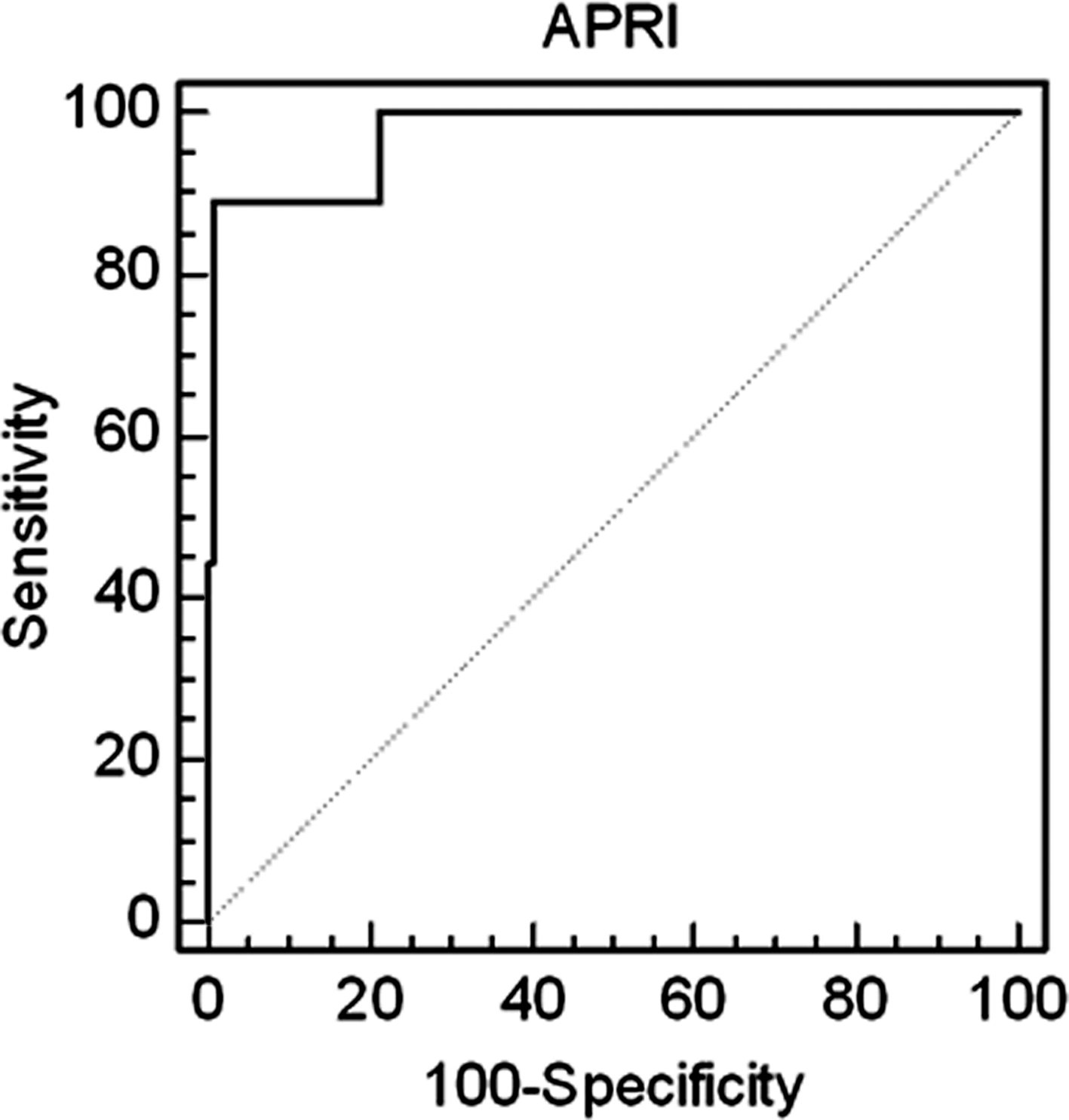
ROC curve of APRI for prediction of liver cirrhosis in chronic hepatitis C patients.
The cut-off value of AST/ALT was 1.17 for predicting significant fibrosis with sensitivity and specificity of 72.7% and 75.45%.; AUROC was 0.806. AST/ALT ratio was less sensitive than APRI in differentiating fibrosis stages as shown in Figure 3.
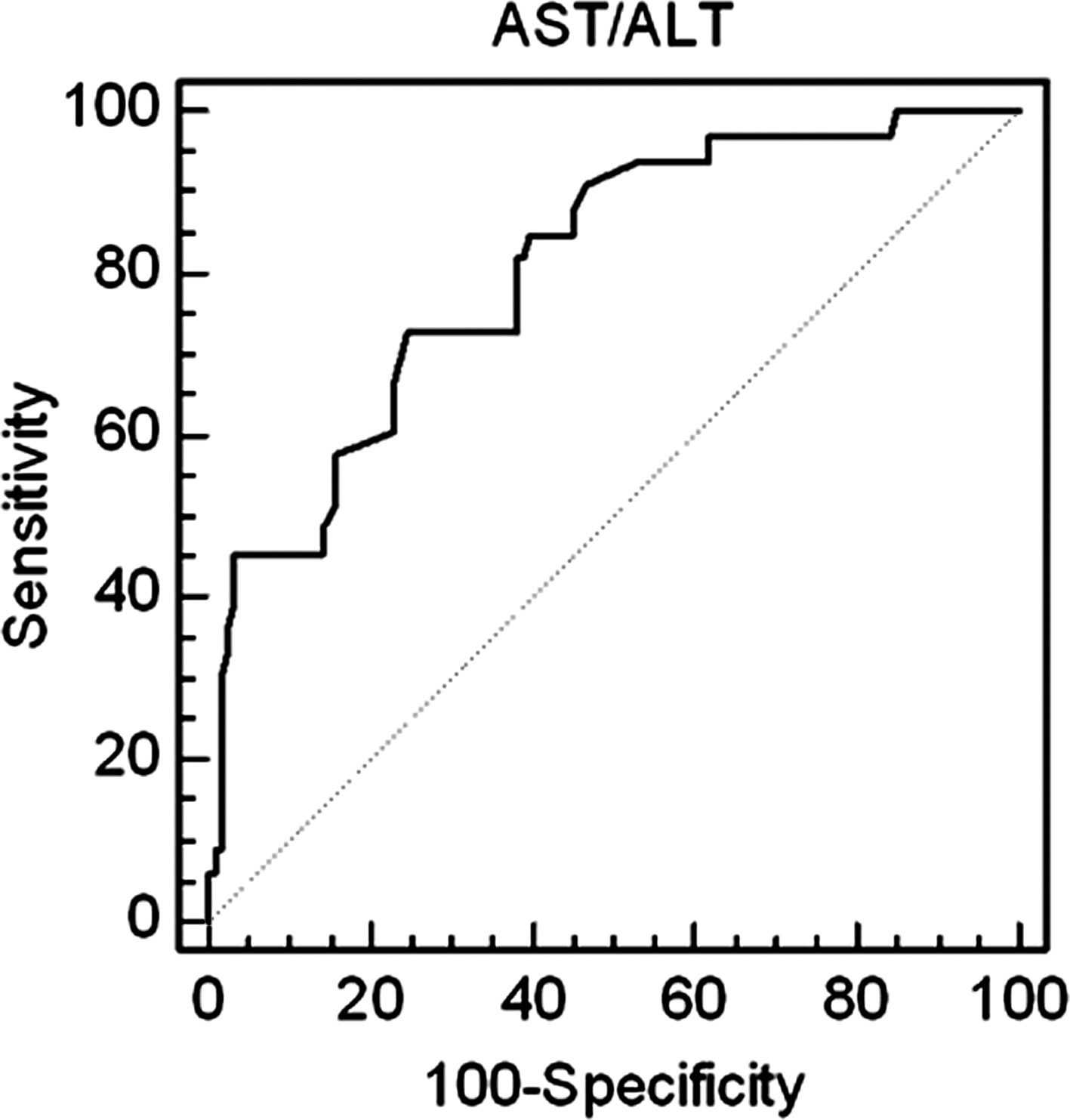
ROC curve of AST/ALT for prediction of significant fibrosis in chronic hepatitis C patients.
Genetic polymorphism −670A>G in the Fas gene was associated with significant fibrosis and cirrhosis (p-value <0.001). Heterozygous mutation was found in 11.4% of patients and 10% of controls, while homozygous mutation was found only in 7.6% of patients. Odds ratio (OR) was not statistically significant (OR=1.93, 95% confidence interval=0.76-4.92) as shown in Table 2 and Figure 4.
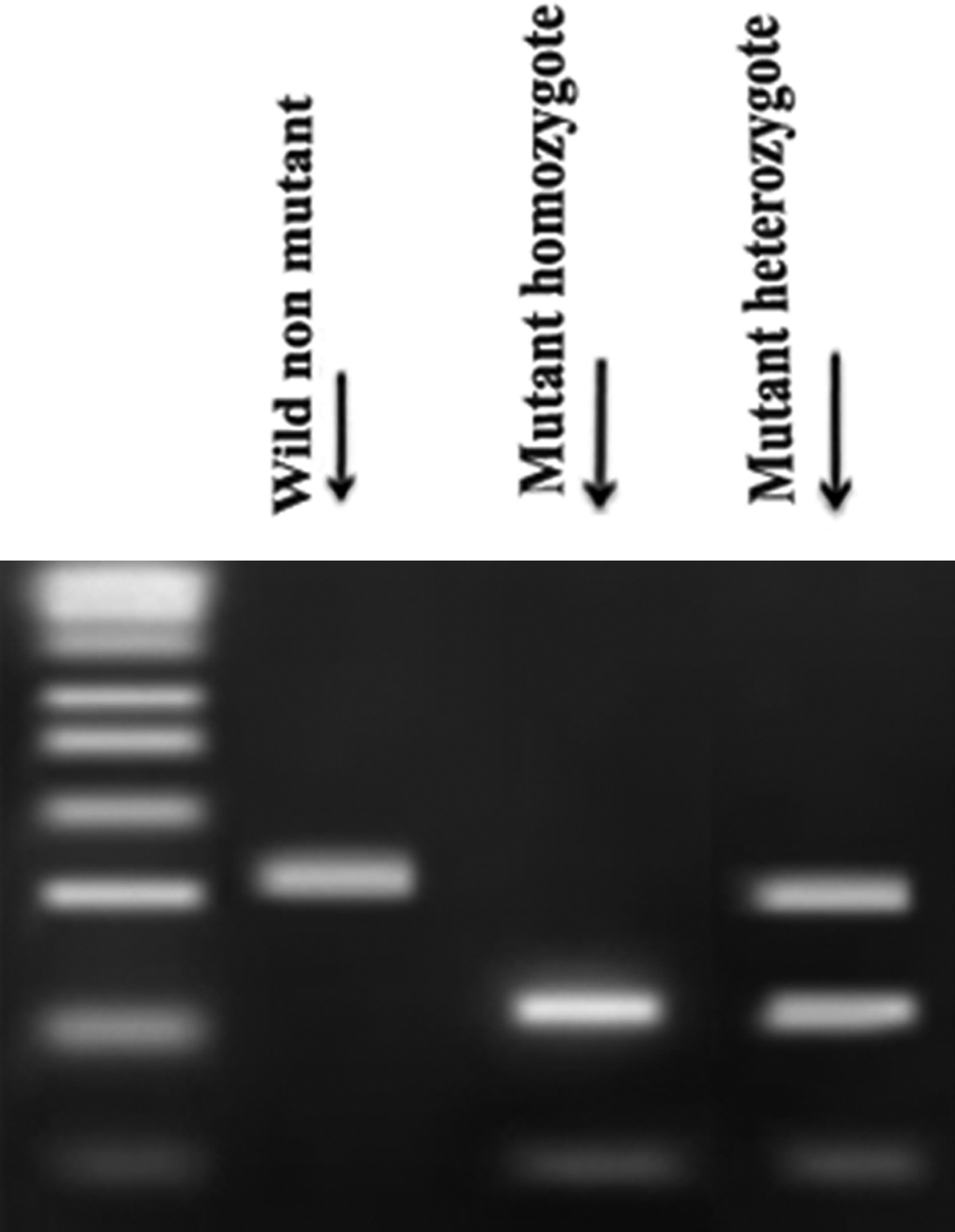
Polymerase chain reaction products amplified from genomic DNA and digested by restriction enzyme ScrF1. Wild nonmutant with A showed a band at 331 bp. Homozygous mutation with A to G substitution showed two bands at 233 and 98 bp. Heterozygous mutation with A to G substitution showed three bands at 331, 233, and 98 bp.
Discussion
Chronic hepatitis C is the most common cause of chronic liver disease and liver cirrhosis, and the most common indication for liver transplantation. Approximately 170 million people are affected with HCV worldwide, comprising 3% of the global population (Wasely and Iter, 2000). HCV infection is associated with an increased risk of hepatocellular carcinoma. The infection has a high propensity to become chronic, and the majority of HCV carriers have histological evidence of liver inflammation and chronic damage. Although there is a very wide spectrum of severity and progression rate, the mechanisms leading to liver cell injury, inflammation, and fibrosis in chronic hepatitis C are not fully understood. However, there is evidence to suggest that apoptosis of liver cells may play a significant role in the pathogenesis of HCV infection (Anguilar et al., 2005).
Altered levels of Fas expression have been implicated in the pathogenesis of several liver diseases. In HCV infection, Fas expression has been found to be upregulated in hepatocytes in accordance with severity of liver inflammation. These Fas-expressing hepatocytes become susceptible to the apoptotic death signal. When T cells migrate between hepatocytes and recognize viral antigens, they become activated and express Fas L, which can transduce the apoptotic death signal in Fas bearing hepatocytes. Thus, the Fas/FasL system seems to play an important role in liver cell injury caused by HCV infection (Hiramatsu et al., 1997; Tobi et al., 2001).
However, apoptosis as the result of viral infection can be induced not only by the host immune response through the function of activated T cells and natural killer cells, but also by viral proteins themselves (Ruggier et al., 1997). Recent studies indicate that the HCV core protein may have a regulatory function in modulating apoptosis in hepatocytes by either enhancing or suppressing it, depending on the transfection methods or cell types used, whereas both the NS3 and NS5A proteins were shown to have antiapoptotic effects. The antiapoptotic effect might be advantageous for HCV by allowing the host hepatocyte to survive apoptosis, resulting in sustained infection (Farci et al., 1992).
Since Fas expression levels may be influenced by the polymorphism in the promoter region of Fas gene, particularly when they affect transcription factor binding sites, we have investigated this genetic variant at −670A>G because of its special genetic localization and its involvement in several autoimmune and neurodegenerative diseases, as well as development of cancer (Kanemitsu et al., 2002; Van Veen et al., 2002; Sibley et al., 2003).
Concerning our study, the genetic polymorphism in the promoter region of the Fas gene was associated with the progression of fibrosis, indicating a possible role of Fas polymorphism −670A>G in the pathogenesis of chronic hepatitis C. However, there was no association between this polymorphism and the risk of chronic hepatitis C. Anguilar et al. (2005) and Mcllroy et al. (2005) observed that genetic polymorphism −670A>G in the Fas gene was associated with severity of liver inflammation but they did not find an association between the polymorphism and progression of fibrosis. The difference between our data and those of Anguilar may be attributed to the younger age of the patient group, as their mean age at biopsy was 33.8 years or it may be due to incomplete availability of data regarding the duration of infection, as the data were available for only 55.9% of patients, thereby reducing the statistical power considerably.
The evaluation of the degree of liver fibrosis is of fundamental importance to the prognosis, follow-up, and therapeutic decision making for patients with chronic liver disease. Liver biopsy is an invasive method with some limitations, including sampling artefact, inter-individual as well as intra-individual variability in scoring. Furthermore, serial liver biopsies are not a practical means of assessing fibrosis progression due to potential complications and costs. In our study, we tried to overcome that by examining each specimen by at least two pathologists (Eduardo et al., 2007).
In the last decade, many studies have been dedicated to the search of noninvasive markers able to provide accurate information about liver fibrosis and necrosis in patients with chronic potentially progressive disease. Actually, the efficacy of these markers encounters difficulty regarding the standardization and definition of cut-off values for each degree of fibrosis. APRI and AST/ALT are well-known predictors of advanced liver disease. The mean values of both markers in our study were significantly higher in patients with (F3-F4) compared with those with (F0-F2).
However, APRI showed a better sensitivity than AST/ALT for the prediction of significant fibrosis. These findings are in agreement with Eduardo et al. (2007). Moreover, better sensitivity of APRI led us to evaluate its accuracy as predictor of actual cirrhosis, showing high sensitivity and specificity to exclude liver cirrhosis without performing liver biopsy. In our population, the cut-off values of APRI were set at 1.3 for predicting significant fibrosis and 3.43 for predicting liver cirrhosis with higher sensitivity and specificity than those reported by Chen-Sheng et al. (2008). However, fluctuating patterns of AST and ALT activity in patients with chronic viral hepatitis may be an important limitation for these markers (Parise et al., 2006; Chen-Sheng et al., 2008).
In conclusion, genetic polymorphism −670A>G of the Fas gene was associated with significant fibrosis in patients with chronic hepatitis C. APRI and AST/ALT are independent predictors for significant fibrosis. Moreover, APRI can be used as an index to exclude liver cirrhosis without performing liver biopsy. Further studies are recommended on larger populations to evaluate the association between the Fas promoter genotype and the risk of chronic hepatitis C infection and to improve the clinical utility of these markers in response to antifibrotic drugs and interferon therapy, which may pave the way for apoptosis-based therapeutics.
Footnotes
Disclosure Statement
No competing financial interests exist.