
Abstract
Objective: Whereas some studies have reported that the osteoprotegerin (OPG) gene is associated with osteoporosis risk in some studies, their results have proved inconclusive. We performed a meta-analysis of studies on the associations between OPG A163G and G1181C polymorphisms and the risk of osteoporosis. Methods: A literature search in PubMed, Embase, Web of Science, Cochrane Library, and China Biological Medicine (CBM) databases was conducted to identify all eligible case-control studies published before August 15th, 2013. Pooled odds ratios with their corresponding 95% confidence intervals were used to evaluate the strength of the association under either a fixed- or random-effect model according to the heterogeneity test. Results: Ten case-control studies were included with a total of 1673 osteoporosis cases and 1554 healthy controls in this meta-analysis. For the OPG A163G polymorphism, the combined results showed that the G allele of the A163G polymorphism may be associated with an increased risk of osteoporosis. Stratified analyses showed that the magnitude of the effect was similar among the Caucasian and postmenopausal women subgroups. Unlike the A163G polymorphism, the meta-analysis results revealed that the C allele of the G1181C polymorphism may be associated with a decreased risk of osteoporosis, especially in the Asian and postmenopausal women subgroups. No publication bias was detected for either polymorphism. Conclusion: Our findings showed that the G allele of the OPG A163G polymorphism may increase osteoporosis risk, whereas the C allele of the G1181C polymorphism may protect individuals from osteoporosis. Both of these effects were observed in postmenopausal women.
Introduction
O
Materials and Methods
Search strategy
Clinical studies in which OPG A163G and G1181C polymorphisms are related to osteoporosis were identified by an extensive literature search in PubMed, Embase, Web of Science, Cochrane Library, and Chinese Biomedical (CBM) literature databases up to August 15, 2013. We used the following keywords and MeSH terms without any language restriction: (“osteoporosis” or “bone loss” or “bone density”) and (“genetic polymorphism” or “single-nucleotide polymorphism” or “SNP” or “mutation” or “variation”) and (“osteoprotegerin” or “OPG” or “TNFRSF11B”). We also screened references of retrieved articles and review articles to identify potentially eligible studies that might have been missed in the electronic search.
Selection criteria
To be included in the analysis, candidate studies had to meet the following criteria: (1) case-control study focused on the relationship between OPG A163 and G1181C polymorphisms and susceptibility to osteoporosis; (2) all patients met the diagnostic criteria for osteoporosis; and (3) sufficient data on allele and genotype frequency. Studies were excluded if they did not meet all of the inclusion criteria. If there were multiple publications from the same study, either the one with the largest sample size or the most recent publication was selected. Any disagreements were resolved by discussions and subsequent consensus.
Data extraction
Two investigators independently extracted the following available information from eligible studies using a standardized format: surname of the first author, year of publication, country of population studied, subjects' ethnicities, number of participants recruited for genotyped cases and controls, age of cases and controls, method of genotyping, the genetic polymorphism(s) assessed, allele/genotype frequency in cases and controls, and Hardy-Weinberg equilibrium (HWE) status in controls. Data that were not available in the source publications were obtained from the corresponding author whenever possible. In addition, we compared key study characteristics, such as the location, publication date, and authorship, to determine the existence of multiple publications from the same study. In cases of conflicting evaluations, disagreements were resolved through discussions and careful reexamination of full texts by the investigators.
Quality assessment
In addition, the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) quality score system was used to assess the methodological quality of included studies (da Costa et al., 2011). The quality scale consists of 40 items with scores ranging from 0 to 40. The eligible studies were classified into three levels based on their scores: low quality (0-19), moderate quality (20-29), and high quality (30-40), respectively. Information was independently extracted from all the eligible studies by two investigators using a piloted data standardized form. In cases of conflicting evaluation, consensus was reached by discussion.
Statistical analysis
The degree of interstudy heterogeneity was tested using Cochran's Q-statistic (Jackson et al., 2012) and the I2 test (Peters et al., 2006). When a significant Q test with p<0.05 or I2>50% indicated significant heterogeneity, the random-effect model was used to estimate the pooled odds ratios (ORs) with their corresponding 95% confidence intervals (95% CIs) under five genetic models (the allele model, the dominant model, the recessive model, the homozygous model, and the heterozygous model). Otherwise, the fixed model would be used. The significance of the pooled estimates was determined using the Z-test. Genotype distributions in controls were tested for HWE by the chi-square test. To explore potential sources of heterogeneity, subgroup analyses were performed based on ethnicity, source of control, HWE status, and genotype method, where applicable. Univariate and multivariate regression analyses were also performed to identify variables that could explain potential sources of heterogeneity (Jackson et al., 2012). Sensitivity analysis was conducted by omitting hospital-based and non-HWE studies to avoid confounding effects. To investigate whether publication bias might affect the validity of estimates, the Begg's funnel plot was constructed. The symmetry of the funnel plot was further evaluated by the Egger's linear regression test (Peters et al., 2006). All two-tailed p<0.05 were considered statistically significant. All analyses were performed using the STATA software, version 12.0 (Stata Corp, College Station, TX).
Results
Baseline characteristics of included studies
In accordance with the inclusion criteria for this meta-analysis, 10 case-control studies (Langdahl et al., 2002; Zhao et al., 2005; Hsu et al., 2006; Wu and Liu, 2006; Kim et al., 2007; Shui et al., 2008; Mencej-Bedrac et al., 2009; Seremak-Mrozikiewicz et al., 2009; Brambila-Tapia et al., 2012; Hussien et al., 2013) were included and 139 were excluded. A flow chart of the study selection process and specific reasons for any exclusion from this meta-analysis is shown in Figure 1. The characteristics and methodological quality of the included studies are summarized in Table 1. A total of 3227 subjects were involved in this meta-analysis, including 1673 osteoporosis patients and 1554 healthy controls. Publication years of the included studies range from 2002 to 2013. Of the 10 studies that met the criteria for inclusion in the meta-analysis, 7 examined the A163G polymorphism (Langdahl et al., 2002; Hsu et al., 2006; Wu and Liu, 2006; Shui et al., 2008; Seremak-Mrozikiewicz et al., 2009; Brambila-Tapia et al., 2012; Hussien et al., 2013) and 5 investigated the G1181C polymorphism (Langdahl et al., 2002; Zhao et al., 2005; Kim et al., 2007; Mencej-Bedrac et al., 2009; Seremak-Mrozikiewicz et al., 2009). In the seven studies on the A163G polymorphism, five studies reported that the genotype distribution in controls did not deviate significantly from HWE, and four out of the five studies on G1181C polymorphism complied with HWE. Overall, six studies were conducted in Asians and the other four in Caucasians. Eight studies used population-based (community populations) controls and two studies used hospital-based controls. The classical polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method was performed in seven studies, two studies used the TaqMan method, and the remaining one used the direct sequencing method. The quality scores of the included studies were moderate to high, with STROBE scores higher than 20.
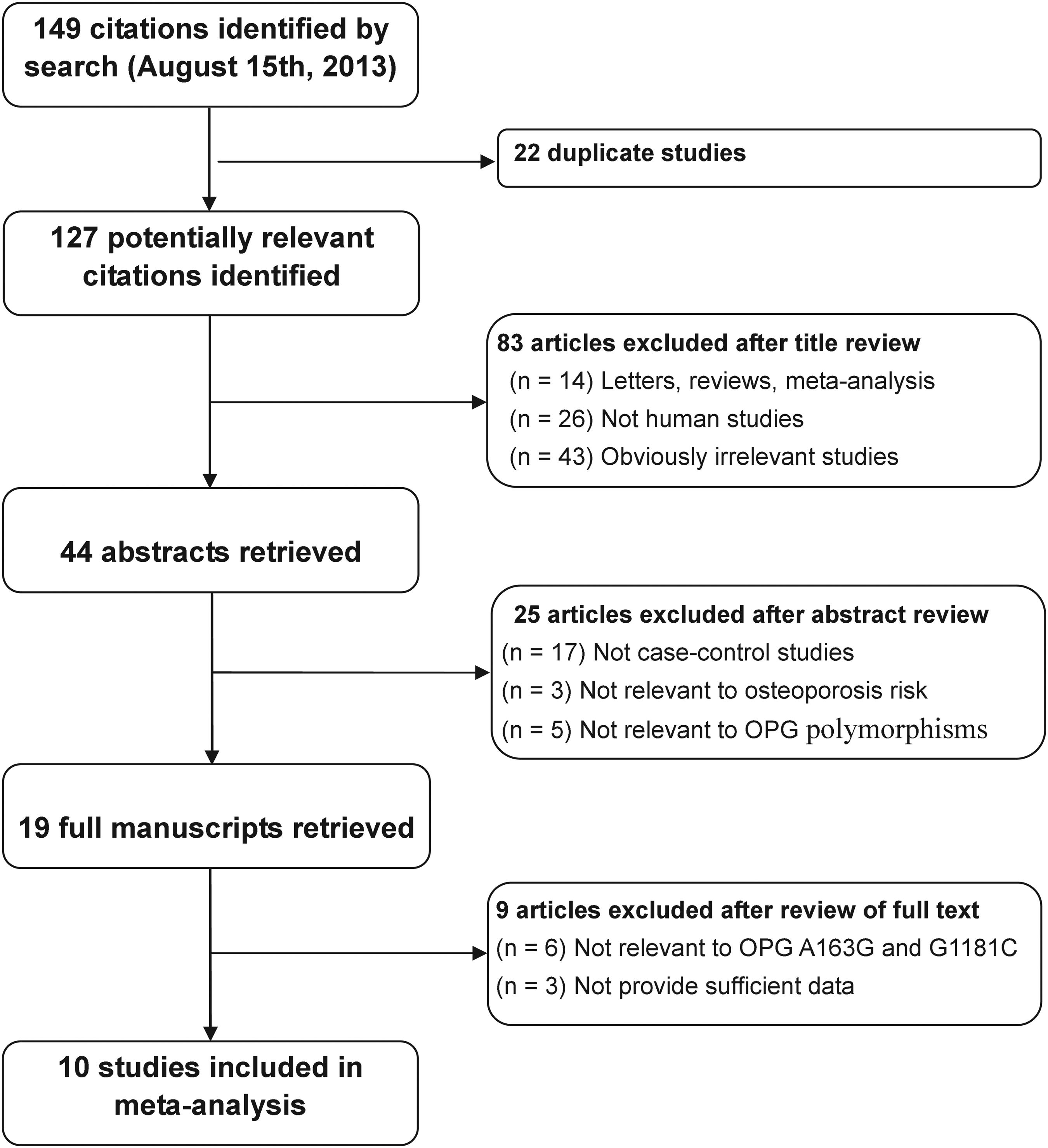
Flow diagram of selection of studies and specific reasons for exclusion from the present meta-analysis.
NA, no data; PB, population based; HB, hospital based; PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism.
OPG A163G polymorphism and increased osteoporosis risk
A summary of the meta-analysis findings on the relationship between OPG A163G polymorphism and susceptibility to osteoporosis is provided in Table 2. Data from 7 case-control studies, comprising 1078 osteoporosis cases and 1092 healthy controls, were pooled together for analysis of the A163G polymorphism. Since heterogeneity obviously existed (ph<0.001, I2=77.2%), the random-effect model was conducted. The meta-analysis results revealed that the G allele of the A163G polymorphism may be associated with an increased risk of osteoporosis (G allele vs. A allele: OR=1.25, 95% CI: 1.07-1.45, p=0.005; AG+GG vs. AA: OR=1.28, 95% CI: 1.06-1.55, p=0.010; GG vs. AA: OR=1.50, 95% CI: 1.41-2.77, p=0.022), although this association was not significant under the other two models (GG vs. AA+AG: OR=0.73, 95% CI: 0.52-1.02, p=0.063; GG vs. AG: OR=1.05, 95% CI: 0.72-1.54, p=0.804), which may be the reason that both genotypes carry the risk G allele, resulting in no significant differences. The results were not substantially changed after the exclusion of one hospital-based study (Table 2). After excluding studies in which the genotype distributions of controls significantly deviated from HWE, the remaining HWE studies revealed an even more significant association between OPG A163G polymorphism and an increased osteoporosis risk (G allele vs. A allele: OR=1.47, 95% CI: 1.20-1.81, p<0.001; AG+GG vs. AA: OR=1.58, 95% CI: 1.23-2.03, p<0.001; GG vs. AA: OR=2.25, 95% CI: 1.34-3.77, p=0.002). Subgroup analysis by ethnicity showed that the magnitude of the effect was similar in Caucasians and Africans, but not in Asians (Fig. 2A). Further subgroup analyses based on subject type suggested that the G allele of the A163G polymorphism was associated with an increased osteoporosis risk in the postmenopausal women subgroup, while no evidence of any significant association was observed in the men and women subgroups (Fig. 2B). In addition, a significant association was found in the analysis of the PCR-RFLP subgroup based on the genotype method (Table 2).
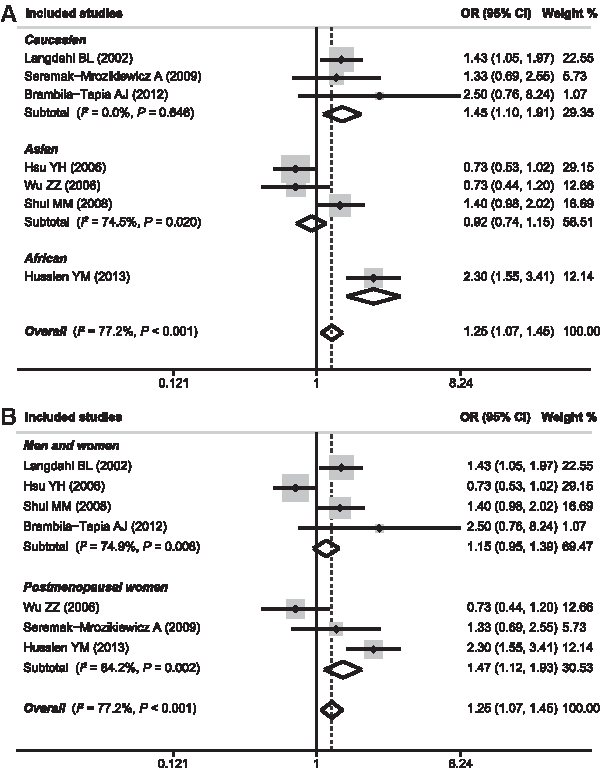
Forest plots of odds ratios (ORs) for the association between osteoprotegerin (OPG) A163G polymorphism and susceptibility to osteoporosis in subgroup analysis based on ethnicity
OR, odds ratio; 95% CI, 95% confidence interval; HWE, Hardy-Weinberg equilibrium; OPG, osteoprotegerin.
OPG G1181C polymorphism and decreased osteoporosis risk
An evaluation of the association between OPG G1181C polymorphism and osteoporosis risk is presented in Table 3. Data from 5 case-control studies, consisting of 1002 osteoporosis cases and 815 healthy controls, were pooled together for analysis of the G1181C polymorphism. The fixed-effect model was conducted since no heterogeneity obviously existed (ph=0.222, I2=29.9%). Contrary to the A163 polymorphism, the meta-analysis results revealed that the C allele of the G1181C polymorphism may be associated with a decreased risk of osteoporosis (C allele vs. G allele: OR=0.79, 95% CI: 0.69-0.90, p=0.001; GC+CC vs. GG: OR=0.79, 95% CI: 0.64-0.98, p=0.031; CC vs. GG+GC: OR=0.74, 95% CI: 0.59-0.93, p=0.010; CC vs. GG: OR=0.66, 95% CI: 0.50-0.88, p=0.005; CC vs. GC: OR=0.70, 95% CI: 0.55-0.89, p=0.003), especially in Asians (Fig. 3A). The results were not substantially changed after the exclusion of one hospital-based study as well as one non-HWE study (Table 3). Subgroup analysis by subject type also showed a significant association between the C allele of the G1181C polymorphism and a decreased osteoporosis risk in postmenopausal women subgroup under three genetic models (C allele vs. G allele: OR=0.75, 95% CI: 0.63-0.88, p=0.001; GC+CC vs. GG: OR=0.67, 95% CI: 0.52-0.87, p=0.002; CC vs. GG: OR=0.57, 95% CI: 0.40-0.82, p=0.002), but not in men and women subgroups (Fig. 3B). In addition, we performed stratified analysis based on the genotype method and the result indicated that a similar association was found in the non-PCR-RFLP subgroup (C allele vs. G allele: OR=0.68, 95% CI: 0.54-0.85, p=0.001; GC+CC vs. GG: OR=0.54, 95% CI: 0.38-0.78, p=0.001; CC vs. GG: OR=0.50, 95% CI: 0.31-0.79, p=0.003), while no significant association was found in the PCR-RFLP subgroup.

Forest plots of ORs for the association between OPG G1181C polymorphism and susceptibility to osteoporosis in subgroup analysis based on ethnicity
Meta-regression and publication bias
Potential sources of between-study heterogeneity were also investigated using univariate and multivariate meta-regression. We tested the influence of ethnicity, control sources, Hardy-Weinberg equilibrium, and SNP testing method on the per-study effect size in meta-regression, as shown in Table 4. The results showed that none of these covariates were a significant source of heterogeneity (All p>0.05). Begg's funnel plots and the Egger's linear regression test were used to assess potential publication bias of included studies for both A163G and G1181C polymorphisms under the allele model. The shapes of the funnel plots did not reveal any evidence of obvious asymmetry (Fig. 4). The Egger's test also did not display a strong statistical evidence of publication bias (A163G: t=0.39, p=0.715; G1181C: t=−0.71, p=0.527).
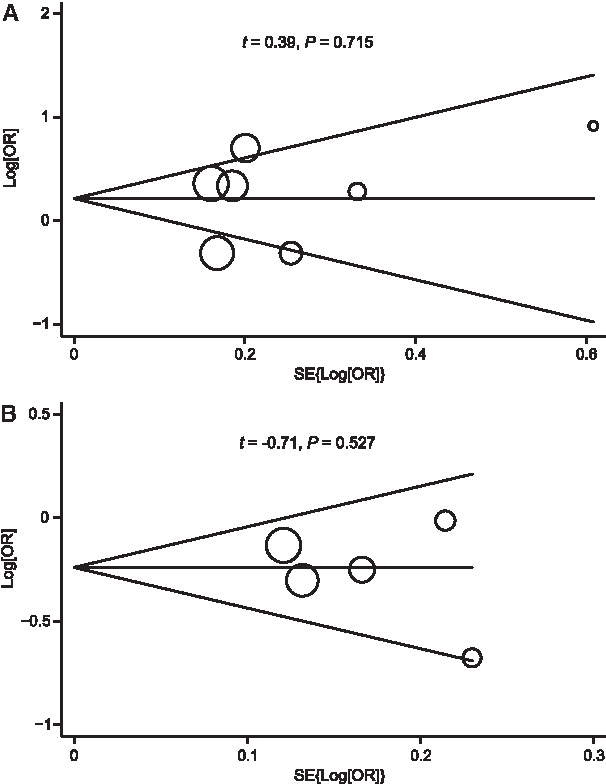
Begg's funnel plots of publication bias in selection of studies on OPG A163G
SE, standard error.
Discussion
Since OPG plays an important role as an inhibitor of osteoclast differentiation, polymorphisms in the gene coding for OPG might have an influence on the bone remodeling process (Boyle et al., 2003). Thus, the OPG gene is a candidate gene for identifying individuals at risk for developing osteoporosis. The human OPG gene is a member of the nuclear receptor superfamily involved in calcium and phosphate homeostasis and hence implicated in a number of diseases, such as osteoporosis (Arko et al., 2002). Gene mutation could affect the function of OPG and thus could be associated with the osteoporosis susceptibility. The G to A substitution at position 163 in the promoter region and the G to C substitution at loci 1181 in the first exon of the OPG gene have been well described (Ferrari, 2008). Several investigations have reported that the OPG A163G and G1181C polymorphisms were associated with the onset of osteoporosis; however, the results of individual studies were not as robust as the pooled results in meta-analysis. To date, there has been one interesting meta-analysis concerning the relationship between OPG genetic polymorphisms and bone mineral density (BMD). Lee et al. (2010) performed a meta-analysis of eight studies and found that the G1181C polymorphism is associated with lumbar BMD in Europeans and Asians and with femoral neck and total hip BMD in Europeans only, while no association was found between the A163G and T950C polymorphisms and BMD. To our knowledge, however, no meta-analysis has explored the association between OPG genetic polymorphisms and osteoporosis risk based on the genotype and allele frequency data. Therefore, the present meta-analysis was performed to determine whether or not these polymorphisms could predict susceptibility to osteoporosis.
For this study, we reviewed a broad selection of publications found in electronic databases and included 10 studies in our meta-analysis. We found that the G allele of A163G polymorphism may be associated with an increased risk of osteoporosis in Caucasians, but not in Asians. Although a significant association was also found in Africans, the small sample size from only one study limited the statistical power of this result. Unlike the A163G polymorphism, the results of our meta-analysis revealed that the C allele of the G1181C polymorphism may be associated with a decreased risk of osteoporosis, especially in Asians. Subgroup analyses based on subject type suggested that the G allele of the A163G polymorphism was associated with an increased osteoporosis risk in the postmenopausal women subgroup, while no evidence of any significant association was observed in the men and women subgroups. Similarly, subgroup analysis by subject type also showed a significant association between the C allele of the G1181C polymorphism and a decreased osteoporosis risk in the postmenopausal women subgroup, but not in the men and women subgroups. Begg's funnel plots and the Egger's linear regression test did not reveal any evidence of obvious asymmetry, which indicated the accuracy and consistency of the results.
The findings of our meta-analysis should be regarded cautiously due to heterogeneity of enrolled cases, limited statistical power, variable study designs, and different interventions, which may affect the results. In interpreting the results of this meta-analysis, some specific issues pertinent to this work should be addressed. First, for the A163G polymorphism, the sample sizes of seven included studies used in our analysis were not sufficiently large for a comprehensive analysis, especially for stratified analyses by menopausal status. It is therefore possible that the apparent effects of A163G on postmenopausal women were due to chance. As for the G1181C polymorphism, due to insufficient data, a stratified analysis of subject type also encountered the similar problem. Hence, large-scale and well-designed studies are warranted in the future. Second, most of the included studies were carried out in Asian and Caucasian populations; thus, more research needs to be conducted in the African population. Third, as with other complex traits, osteoporosis risk may also be modulated by other genetic markers besides the OPG gene. Thus, the current meta-analysis emphasizes that elucidating the pathogenesis of osteoporosis demands investigation of multiple gene variants and their combined influence on osteoporosis risk. Fourth, we did not fully cover all genetic variations in the OPG gene, since only the most common variants were studied. Fifth, the genetic influence of the OPG gene on osteoporosis risk may differ between premenopausal and postmenopausal women according to menopausal status, while no data on premenopausal women were available for the analysis, which demands further investigation about this issue in premenopausal women. Last, meta-analyses may miss true effects in the presence of even modest between-study heterogeneity since they are based on the assumption of etiologic homogeneity across studies. Due to the presence of heterogeneity, the summary estimates provided in the present study can only reflect a crude analysis. Thus, we could not exclude the possibility of false-positive/-negative findings. Despite these statistical limitations, our study is the first comprehensive meta-analysis of all eligible studies concerning the association between OPG A163G and G1181C polymorphisms and osteoporosis risk based on genotype and allele frequency data. Further, we explored interstudy variation using stratified analyses based on ethnicity, subject type, source of control, and SNP detection method.
In conclusion, the current meta-analysis of 10 studies examined the association of two common polymorphisms of the OPG gene with osteoporosis risk. Our findings showed that the G allele of the OPG A163G polymorphism may increase osteoporosis risk, whereas the C allele of G1181C polymorphism may protect individuals from osteoporosis. Both of these effects were observed in postmenopausal women. Thus, our results support the hypothesis that SNP markers at A163G and G1181C of the OPG gene may serve as biological indicators of osteoporosis risk. Further studies should pay attention to other potentially functional SNPs. In addition, how these polymorphisms affect osteoporosis risk is not known, and thus, future functional studies are warranted to understand the mechanisms underlying these associations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.