
Abstract
Aims: TPOX triallelic genotypic pattern has been described in the setting of forensic and paternity testing but not in bone marrow transplantation (BMT) monitoring for graft engraftment. Materials and Methods: A total of 50 cases have been studied using the AmpFLSTR® Identifiler™ polymerase chain reaction amplification kit as part of the workup of patients and donors before and after BMT at the American University of Beirut Medical Center. Results: Of the 50 studied cases, 49 showed typical allelic patterns of the variable short tandem repeats detected by the assay; however, one single patient showed a biallelic TPOX genotype in the pre-BMT specimen but a triallelic pattern in the post-BMT sample. Conclusion: Triallelic patterns of TPOX should also be considered in the context of BMT monitoring testing where misinterpretation of the allelic pattern can lead to wrong unwanted conclusions related to the graft condition and proper quantification of donor DNA.
Introduction
TPO
Alleles at the TPOX locus have different numbers of a four nucleotide repeat motif arranged in tandem (Anker et al., 1992). The TPOX triallelic genotype results from the duplication of the short tandem repeats (STRs) segment and flanking regions (Picanço et al., 2014). There are two types of triallelic patterns: type 1 where after polymerase chain reaction (PCR) amplification, the first two peaks have a different intensity than the third visualized peak and this type refers to the condition when a mutation occurs in early somatic cells and type 2 where after PCR amplification, three similar peaks are seen and this is associated with a constitutional chromosomal rearrangement (Clayton et al., 2004). The type 2 triallelic pattern can either be associated with clinical symptoms or have a minimal effect on normal development, depending on whether the cause behind this pattern is a chromosomal duplication or a partial maternal isodisomy for chromosome 2p, respectively (Bakker et al., 2001; Lukka et al., 2006).
Moreover, and as per Lane (2008), TPOX triallelic genotype is a condition affecting females to a higher extent than males, and fathers with this condition transmitted this genotype to their female descendants only, proposing that the additional allele is located on the X chromosome.
The frequency of the TPOX triallelic genotype varies between populations and appears to be the highest among Africans. Various researchers investigated the prevalence of this pattern among different populations. For instance, a study by Huel et al. (2007) among 32,800 participants from Serbia, Bosnia, and Kosovo revealed the presence of one individual with TPOX triallelic genotype (∼0.003%), whereas around 0.18% of 10,000 individuals from the surrounds of Alabama, USA, carried this genotype (Crouse et al., 1999). Interestingly, Lane (2008) reported a genotype frequency of ∼2.4% for TPOX triallelic individuals, among native South Africans, Namibians, Angolans, and Ghanaians.
The TPOX locus, as part of the CODIS STR loci used by the Federal Bureau of Investigation (FBI), serves as a genetic marker to differentiate individuals and is used in forensic and paternity testing. This is possible through the visualization of the amplified DNA fragments that vary in size depending on the carried genotype (Diaz V et al., 2009).
In this study, we are reporting an interesting pattern of a triallelic TPO genotype, which is occurring in a bone marrow transplantation (BMT) clinical setting with an unusual pattern of allelic expression. Previous literature showed some occurrences in forensic or paternity studies, and we are, hereby, drawing the attention of molecular pathologists, geneticists, and transplant physicians about this possible finding also in the bone marrow engraftment monitoring studies post-transplantation.
Materials and Methods
Subjects under study
A total of 50 cases have been studied using this kit assay as part of the workup of patients and donors before and after BMT at the American University of Beirut Medical Center.
DNA isolation and quantification
Genomic DNA was isolated from peripheral blood samples collected from the donor and the patient before and after stem cell transplantation using a column-based DNA isolation technique (QIAamp DNA Blood Mini Kit from Qiagen). Two hundred microliters of blood material was digested with 20 μL of protease, lysed in 200 μL of lysis buffer, and incubated at 56°C for 10 min. The lysate was precipitated with 200 μL pure ethanol and filtered using QIAamp Mini Spin Column, then washed twice with washing buffer, and later eluted in elution buffer. The DNA concentration was quantified by spectrophotometry.
Polymerase chain reaction assay and setup
The AmpFLSTR® Identifiler™ polymerase chain reaction (PCR) amplification kit (Applied Biosystems, Life Technologies) is used as part of the pre-BMT and post-BMT engraftment studies in our institution. The AmpFLSTR Identifiler® PCR amplification kit is a STR multiplex assay that amplifies 15 tetra-nucleotide repeat loci (D8S1179, D21S11, D7S820, CSF1PO, D3S1358, TH01, D13S317, D16S539, D2S1338, D19S433, vWA, TPOX, D18S51, D5S818, and FGA) and the Amelogenin (gender-determining marker) in a single PCR amplification using ABI 3500 DNA genetic analyzer from Applied Biosystems. The AmpFLSTR Identifiler Allelic Ladder was used to genotype the analyzed samples.
PCR setup, amplification, and DNA profiling
One nanogram of genomic DNA was amplified with 15 μL of the 15 autosomal STR loci and the gender-determining marker, Amelogenin master mix (contained in the AmpFLSTR Identifiler PCR amplification kit) using 0.5 U of the AmpliTaq Gold® DNA polymerase per reaction by direct PCR using Agilent thermocycler (Agilent Technologies). The PCR conditions are as follows: preincubation at 95°C for 11 min, 30 cycles with 94°C/1 min, 59°C/1 min, and 72°C/1 min, with a final elongation step at 60°C for 60 min. For fragment analysis, 1.5 μL of the PCR product was mixed with 24.5 μL of Hi-Di formamide and 0.5 μL GeneScan™-500 LIZ size standard and then denatured at 95°C for 5 min.
The denatured fragments were detected by capillary electrophoresis using the ABI 3500 genetic analyzer from Applied Biosystems. The electrophoresis fragments were analyzed using the GeneMapper IDX software.
Results
Of the 50 cases studied, 49 showed typical allelic patterns of the variable STRs detected by the assay; however, one single patient showed a very interesting pattern: the 65-year-old male, in the pre-BMT specimen, had a biallelic TPOX genotype and expressed the alleles 9 and 11 (Fig. 1). After the BMT, this patient expressed a triallelic TPOX genotype with the alleles 8, 9, and 11 being expressed (Fig. 2). The post-BMT engraftment study revealed a chimerism result of 97% donor DNA. Looking back at the genotype of the donor, we found that the donor, a 60-year-old female who is the sister of the patient, carried a triallelic TPOX genotype with the alleles 8, 9, and 11 (Fig. 3).
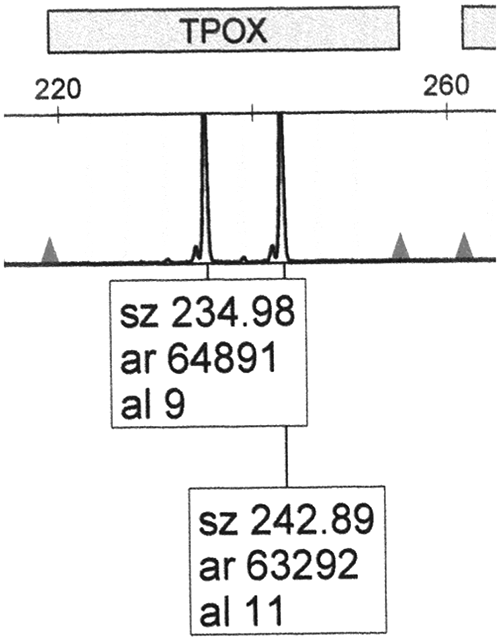
Illustration of the TPOX genotype for the patient pre-bone marrow transplantation.
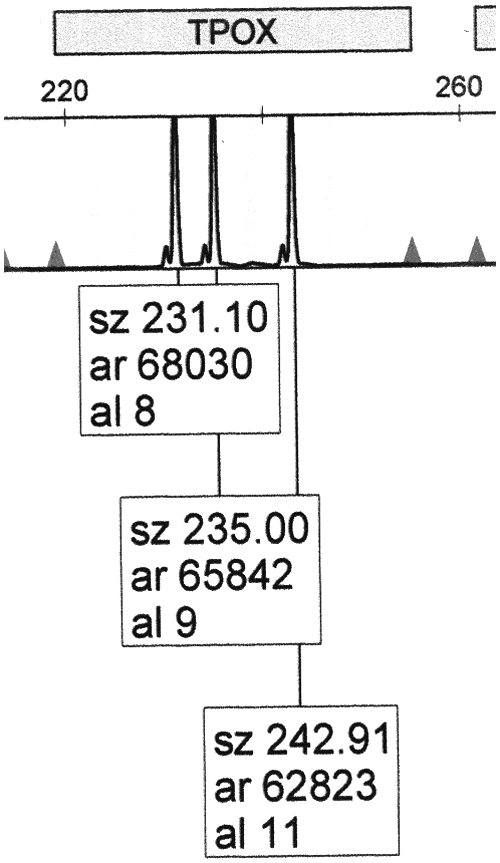
Illustration of the TPOX genotype for the patient post-bone marrow transplantation.
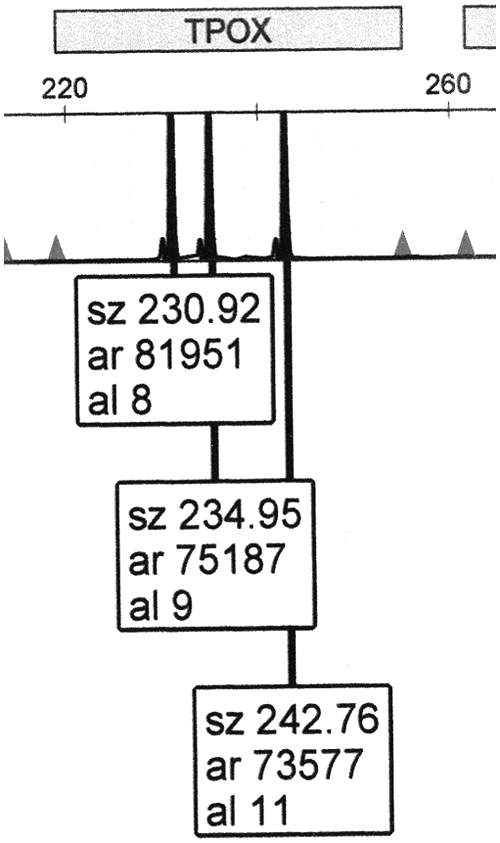
Illustration of the TPOX genotype for the donor.
As shown in Figures 2 and 3, the three peaks at the TPOX locus are of equal intensity, indicating that the triallelic pattern here is of type 2.
Discussion
In our center, this is the first detected case of TPOX triallelic genotype among 50 tested patients and donors. The discovery of this case was part of the pre-BMT and post-BMT services that are done in our laboratory, and unlike other studies where the identification of these cases was part of a paternity testing or forensic applications. Thus, it is important to share this information with transplant physicians, pathologists, and laboratory specialists who perform DNA engraftment studies for monitoring of BMT patients.
The triallelic TPOX pattern has been previously reported and is not unique to our community. Lane (2008) suggested that the extra TPOX allele in 90% of identified triallelic cases is usually featuring allele 10, while other alleles were not frequently found. Moreover, allele 10 was detected in TPOX triallelic individuals to a higher level than in biallelic individuals and suggested that not expressing allele 10 as part of the triallelic genotype could be explained by a slippage mutation from an ancestral third-extra allele 10 (Lane, 2008). In our first report of TPOX triallelic pattern, allele 10 was not a part of the genotype but instead alleles 8, 9, and 11 were expressed, which is an additional feature in this interesting pattern.
We conclude that triallelic patterns of TPOX are not only restricted to forensic or paternity studies but should also be remembered in the context of BMT monitoring testing where misinterpreting the allelic genotype pattern can erroneously lead to unwanted conclusions related to the graft condition and proper quantification of donor DNA.
Footnotes
Author Disclosure Statement
No competing financial interests exist.