
Abstract
Background: This study investigated the influence of human cytochrome P450 2D6 (CYP2D6) gene polymorphism in gastric cancer (GC) patients to understand the pharmacogenomic basis for patient response to postoperative fentanyl analgesia. Methods: The prospective study design contained 212 patients recovering from radical gastrectomy. Peripheral blood samples were collected after general anesthesia, and CYP2D6 genotypes were analyzed using polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method. After providing adequate instructions to operate the analgesia pump, patients self-administered fentanyl via patient controlled intravenous analgesia. The cumulative amount of fentanyl self-administered and the associated adverse effects were recorded at 6, 12, 24, and 48 h postoperatively. Results: Five patients, out of the 212 patients recruited to this study, failed to complete the study. The remaining 207 patients were classified into three groups based on their genotypes: W/W group (n=44), M/W group (n=112), and M/M group (n=51). Our results demonstrated that the cumulative amount of fentanyl consumption significantly increased in the M/M group at 6, 12, and 24 h postoperatively, compared with the W/W group (p<0.05). In addition, visual analogue scale (VAS) score in the M/M group was significantly higher than the W/W group in the analepsia period after general anesthesia and at 6 h postoperatively (p<0.05). No significant adverse effects were observed in all the groups (p>0.05). Conclusion: CYP2D6 polymorphism influenced patient response to postoperative fentanyl analgesia in GC patients.
Introduction
G
The human cytochrome P450 2D6 (CYP2D6) is one of the major enzymes involved in drug metabolism (Geier et al., 2013). CYP2D6 gene is mapped to chromosome 22q13.1, containing nine exons and eight introns, and is an important member of the CYP2D subfamily (Teh and Bertilsson, 2012). The CYP2D6 gene product plays an essential role in the metabolism of about 25% of the clinically useful drugs, and over 100 allelic variants of this gene have been detected, indicating high polymorphism (Wang et al., 2009) (www.imm.ki.se/cypalleles/cyp2d6.htm, access date: August 20, 2014). Several previous studies have demonstrated the functional impact of CYP2D6 polymorphisms on drug response and clearance (Ingelman-Sundberg, 2005; Ingelman-Sundberg et al., 2007; Zhou, 2009). CYP2D6 nonfunctional alleles produce inactive CYP2D6 protein, leading to poor metabolizer phenotype associated with reduced efficacy of tamoxifen, an anticancer drug, in 5-10% of Caucasian population (Scheer et al., 2012). CYP2D6 polymorphisms also impact the metabolism of opioids such as codeine, tramadol, and dihydrocodeine (Leppert, 2011). In addition, Samer et al. (2010) demonstrated that the altered activity of CYP2D6, as a result of genetic polymorphism, influenced oxycodone pharmacodynamics. However, the effects of CYP2D6 polymorphisms on fentanyl metabolism and clearance were understudied, especially in GC (Landau et al., 2008). In view of this, we investigated the influence of CYP2D6 polymorphism on the analgesic effect of fentanyl in GC patients after radical gastrectomy.
Materials and Methods
Ethics statement
All experiments in the study were carried out with the approval of the Institutional Review Board of the Second Affiliated Hospital of Zhengzhou University. Before the study design, each eligible patient or the patient's next of kin provided informed written consent, and the whole study was performed based on the Declaration of Helsinki (Nischal, 2014).
Study subjects
Between June 2011 and June 2013, 212 GC patients who underwent radical gastrectomy were randomly enrolled in this study conducted at the Second Affiliated Hospital of Zhengzhou University. The 212 patients contained 123 men and 84 women, with a median age of 46 years (range, 22-70 years), and a median weight of 57.5 kg (range, 45-70 kg). Eligible patients were defined as the American Society of Anesthesiology (ASA) physical status I-III (Wolters et al., 1996). The study exclusion criteria were as follows: (1) improper liver and kidney function; (2) severe cardiac dysfunction; (3) administration of drugs that impact cardiovascular functions or enhance/inhibit drug metabolism; (4) history of psychiatric illnesses; (5) history of epilepsy; (6) history of allergies to fentanyl; (7) history of diabetes; or (8) serious perioperative complications.
Induction and maintenance of anesthesia
All GC patients were given general anesthesia with midazolam (0.05 mg/kg), etomidate (0.2 mg/kg), fentanyl (5 μg/kg), and vecuronium bromide (0.12 mg/kg) through intravenous injection. The dosage of infusion was adjusted by the A-Line ARX Index (AAI) and hemodynamics change. Mechanical ventilation was carried out with tidal volume at 8-10 mL/kg. For maintenance of anesthesia, GC patients were treated with intravenous pumping of propofol (4-6 mg/kg/h)-remifentanil (5-15 μg/kg/h), and intermittent intravenous injection of fentanyl 0.1-0.2 mg per time. Additionally, the inspired concentration of sevoflurane was controlled within 1-2% and the maxim dosage of fentanyl was 12 μg/kg during laparotomy. Following laparotomy, fentanyl was replaced with intermittent intravenous injection of vecuronium bromide (0.05 mg/kg per time) to maintain muscle relaxation, and the AAI was maintained at 15-25. Ondansetron (8 mg) was injected through vein after skin closure. The radical operation was performed by two surgeons, with arterial blood gas analysis, fluid input and output and blood volume monitored during surgery.
Postoperative analgesia
Patients were transferred to postanesthesia care unit for observation. Endotracheal tube was withdrawn after recovery of spontaneous breathing and patients returned to the consciousness. Visual analogue scale (VAS) was conducted in patients who recovered consciousness (Hawker et al., 2011). The VAS consisted of a horizontal line 100 mm in length: no pain (0-4 mm); mild pain (<30 mm); moderate pain (40-60 mm); and severe pain (70-100 mm). When VAS was over 30 mm, patients were given 30 μg fentanyl via intravenous injection. When VAS was 10-30 mm, patients felt mild pain and analgesia pump was applied. No opioid antagonists or other analgesics were used after operation. Patient-controlled intravenous analgesia (PCIA) was carried out by applying an automatic infusion pump (Apon, ZZB-300): 30 μg/kg fentanyl (RenFu Pharmaceutical Co., Ltd., Yi Chang, China) was diluted with normal saline to 240 mL and then infused to patients without load amount at infusion rate of 1.5 mL/h. Doses of analgesic drugs for patients under PCIA regime was 20 μg/time for 5 min. Patients were instructed to operate the analgesia pump and the VAS score was maintained <30 mm. No opioid receptor antagonist or supplementary analgesics was administrated after the surgery. Noninvasive blood pressure, heart rate, pulse oximetry oxygen saturation (SpO2), VAS score, cumulative amount of self-administered fentanyl, and adverse effects (nausea, vomiting, respiratory depression, dizziness, and somnolence) were recorded at 6, 12, 24, and 48 h postoperatively.
Genotype determination
Peripheral blood sample (2 mL) was collected from each eligible patient after anesthesia and placed in tubes containing ethylene diamine tetraacetic acid (EDTA) as anticoagulant and stored in refrigerator at 80°C. Genomic DNA was extracted using E.Z.N.A SQ Blood DNA Kit (Omega, Norcross, GA). Genotyping CYP2D6 polymorphism was performed with polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). The sequence of the designed primers for PCR amplification: forward 5′-TCAACACAGCAGGTTCA-3′, reverse 5′-CTGTGGTTTCACCCACC-3′. PCR reaction system (total volume, 25 μL) contained: 2 μL genomic DNA template, 2.5 μL 10×PCR reaction buffer, 0.2 mM dNTP mixture, 1.0 mM each primer, 1.25 mM MgCl2, and 0.75 U Taq DNA polymerase. Negative control (without DNA template) was set for all PCR amplifications to exclude false-positive results. PCR amplification condition: denaturation at 95°C for 5 min, denaturation at 95°C for 30 s, annealing at 59°C for 10 s, extension at 72°C for 20 s (total 32 cycles), and final elongation at 72°C for 10 min. The PCR products were digested with endonuclease HphI (2.5 U; New England Biolabs, Ipswich, MA) with digestion reaction system containing 8 μL PCR products, 2 μL 10×digestion buffer, and 0.5 μL HPhI at 37°C for 16 h to detect the allele of gene CYP2D6. Digested PCR products were analyzed using 1.8% agarose gel, and ultraviolet photography was used to record the results. The PCR products of different genotypes were purified and DNA sequence analysis was performed to confirm the genotypes.
Statistical analysis
All statistical data were analyzed with SPSS 18.0 software. Measurement data were expressed as mean±standard deviation. Hardy-Weinberg equilibrium and comparison of enumeration data between groups were analyzed by chi-square test. Comparison of measurement data between groups were tested with variance analysis and t-test. Statistical significance was set at p<0.05.
Results
Electrophoresis results
CYP2D6 polymorphisms were genotyped using PCR-RFLP. Figure 1 shows the results of restriction enzyme digestion of the PCR products. PCR amplification and digestion with HphI resulted in the undigested 433 bp PCR product representing the T/T genotype. When HphI restriction site in the C/C wild-type PCR products was present, the 433 bp product was digested to produce 362 and 71 bp bands. In addition, the heterozygous variant (C/T) for CYP2D6 polymorphism showed three bands of 262, 100, and 71 bp, upon digestion.
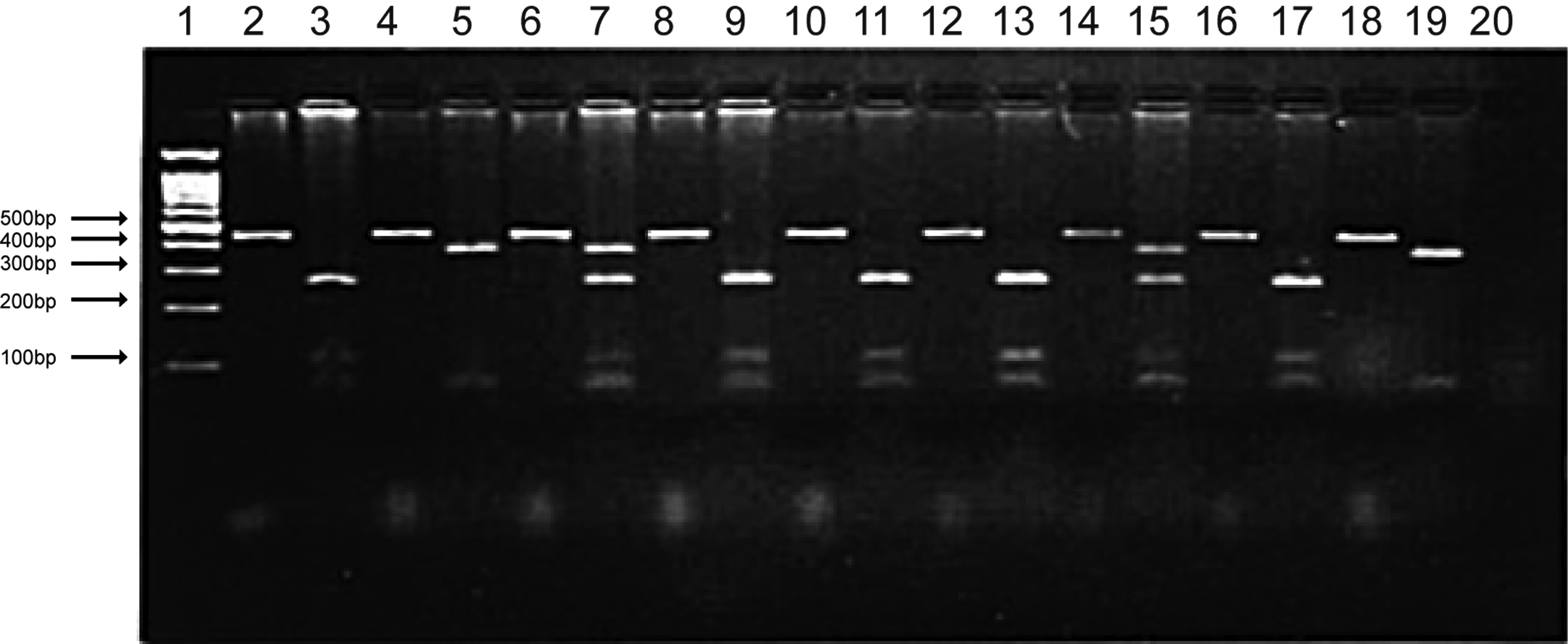
A representative photomicrograph of 1.8% agarose gel electrophoresis showing the products of restriction enzyme digestion after the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) technique.
Baseline characteristics and genotyping
A total of 212 patients were recruited in this study and 5 patients failed to complete the study. Among the five patients, three patients (two with W/M mutation and one with M/M mutation) terminated the study due to the failure of venous indwelling needle, one patient with W/W mutation encountered a mechanical failure and one patient with W/M mutation left due to severe nausea and vomiting. After excluding these five patients, the remaining patients were classified into three groups based on the genotyping results. Homozygous wild (W/W) was found in 44 patients, heterozygous mutant (M/W) in 112 patients, and homozygous mutant (M/M) in 51 patients. For statistical analysis, no significant differences were found in gender, age, weight, height, ASA classification, incision length, duration of surgery and anesthesia, or the intraoperative fentanyl dose among the patients with homozygous wild (W/W), heterozygous mutant (M/W), and homozygous mutant (M/M) (as seen in Table 1).
ASA classification, the American Society of Anesthesiologists physical status classification system.
Table 2 displayed the comparison of the postoperative cumulative amount of fentanyl among the W/W group, the M/W group, and the M/M group during postoperative PCIA period. Compared with the W/W group, the cumulative amount of fentanyl in the M/M group markedly increased at 6, 12, and 24 h after radical gastrectomy during PCIA period (305.6±100.9 mg vs. 262.1±94.2 mg, 430.4±145.5 mg vs. 373.1±109.1 mg, and 657.8±185.2 mg vs. 587.7±132.0 mg, respectively; all p<0.05). No difference in the cumulative amount of fentanyl between the M/W group and the M/M group was detected at 6, 12, 24, and 48 h after radical gastrectomy during PCIA period (all p>0.05). Comparison of the cumulative amount of fentanyl among the W/W group, the M/W group, and the M/M group also showed no statistical difference at 48 h after radical gastrectomy during PCIA period (p>0.05).
Compared with W/W group; p<0.05.
Visual analogue scale score
The comparison of VAS score among the W/W group, the M/W group, and the M/M group during postoperative PCA period is shown in Table 3. It was found that in the period of analepsia after general anesthesia and at 6 h after radical gastrectomy, VAS score in the M/M group was significantly higher than the W/W group (p<0.05). VAS score in the M/M group did not differ from the M/W group (p>0.05). At 24 and 48 h after radical gastrectomy during PCIA period, there was no difference in VAS score among the three groups (all p>0.05).
Compared with W/W group; p<0.05.
Adverse events of postoperative fentanyl analgesia
The incidence of commonly occurring (≥2%) adverse events after PCIA, such as nausea and vomiting, was very low in this study. In the 207 patients, postoperative nausea and vomiting (PONV) occurred in 4 patients of the W/W group (9.09%), 5 patients of the M/W group (4.46%), and in 2 patients of the M/M group (3.92%) at 48 h after surgery during PCIA period. No significant differences in the incidence of PONV were detected among the three groups (p>0.05). Another frequent adverse event (profuse sweating) was found in two patients in the W/W group, four patients in the M/W group, but none in the M/M group. In addition, no obvious respiratory depression was observed during PCIA period in this study.
Discussion
In this study, PCR-RFLP was used for analysis of CYP2D6 gene polymorphism and correlating the genotypes to the response to fentanyl PCIA in GC patients with acute pain after radical gastrectomy. To our knowledge, the influence of CYP2D6 polymorphism on the analgesic effect of fentanyl, used in GC treatment, had not yet been studied. Cancer pain could be induced by tumor involvement, toxicities of treatment, and diagnostic or therapeutic procedures (Kumar, 2011). Pain related to cancer is commonly mediated through neuropathic and nociceptive (inflammatory) mechanisms (Bennett, 2011). In addition, cancer patients might also experience pain caused by noncancer-related conditions, which resemble pain in individuals without cancer (Colson et al., 2011). We enrolled GC patients with acute pain after radical gastrectomy, instead of cancer patients, to study the effect of CYP2D6 polymorphism on the postoperative response to fentanyl analgesia.
Our results demonstrated that CYP2D6 polymorphisms influenced the early analgesic outcomes of fentanyl PCIA in GC patients, and the homozygous mutants showed a relatively poor analgesic effect with a need for higher dosing on the first day after surgery. CYP2D6 is responsible for metabolism of ∼25% of clinically used drugs and has been intensely studied for its genetic polymorphisms because of its relevance in geographically and ethnically diverse populations, where variations in enzyme activities could potentially cause drug-induced toxicity or make drugs ineffective (Teh and Bertilsson, 2012; Geier et al., 2013). Therefore, analysis of CYP2D6 polymorphisms can accurately predict the metabolic phenotype of individuals, based on which individualized dosing regimen could be developed for better clinical outcome. Our study found that the CYP2D6 (C188T) mutation in exon 1, which reduces the metabolic conversion rate of fentanyl in vivo into its major active metabolite M1, impacts the analgesic effect at PCIA, requiring increased dosing of early analgesics. Therefore, CYP2D6 polymorphisms may be the genetic factors responsible for the differences in response to fentanyl, through alterations in drug metabolism, observed between ethnic groups and across individuals within a given population.
PONV is the most common side effect of fentanyl (Zhang et al., 2011). PONV is mainly induced by emetogenic stimuli in perioperative administration including volatile anesthetics, postoperative opioids, and prolonged duration of anesthesia (Apfel et al., 2012). Patients treated with radical gastrectomy are particularly prone to PONV due to the surgery site and the stimulated gastric tube (Liao et al., 2013). Our results indicated no significant correlation between the incidence of postoperative adverse effects and different genotypes of CYP2D6, which might be caused by qualitative evaluation instead of quantitative method we adopted to assess adverse effect.
This is the first study documenting the influences of CYP2D6 polymorphisms on analgesic effect of fentanyl after radical gastrectomy. Some limitations remain in our study. Although we minimized the impact of confounding factors, elements affecting postoperative pain were extensive, including preoperative pain experience, patient awareness of the disease and pain, education levels, personality, and attention. Since CYP2D6 polymorphism was found to be a crucial factor impacting postoperative analgesic effect of fentanyl, future studies must investigate the contribution of this genetic factor, including its variants, to the perception of pain itself.
In conclusion, for the first time, our study demonstrated that CYP2D6 polymorphism significantly influenced the postoperative analgesic effect of fentanyl after radical gastrectomy in GC patients. Due to limitations in this study, further research is needed to confirm our findings.
Footnotes
Acknowledgment
We would like to acknowledge the reviewers for their helpful comments on this article.
Author Disclosure Statement
No competing financial interests exist.