
Abstract
Background: Advances in next-generation sequencing (NGS) technologies are driving a shift from single-gene to multigene panel testing for clinical genetic cancer risk assessment (GCRA). This study explored perceptions, experiences, and challenges with NGS testing for GCRA among U.S. community-based clinicians. Methods: Surveys delivered at initial and 8-month time points, and 12-month tracking of cases presented in a multidisciplinary web-based case conference series, were conducted with GCRA providers who participated in a 235-member nationwide community of practice. Results: The proportion of respondents ordering panel tests rose from 29% at initial survey (27/94) to 44% (46/107) within 8 months. Respondents reported significantly less confidence about interpreting and counseling about NGS compared with single-gene test results (p < 0.0001 for all comparisons). The most cited reasons for not ordering NGS tests included concerns about clinical utility, interpreting and communicating results, and lack of knowledge/skills. Multigene panels were used in 204/668 cases presented during 2013, yielding 37 (18%) deleterious (7% in low/moderate-penetrance genes), 88 (43%) with ≥1 variant of uncertain significance, 77 (38%) uninformative negative, and 2 (1%) inconclusive results. Conclusions: Despite concerns about utility and ability to interpret/counsel about NGS results, a rapidly increasing uptake of NGS testing among community clinicians was documented. Challenges identified in case discussions point to the need for ongoing education, practice-based support, and opportunities to partner in research that contributes to characterization of lesser known genes.
Introduction
G
Next-generation sequencing (NGS) technologies have made multigene panel, whole exome (WES), and whole genome sequence (WGS) testing increasingly accessible, offering significantly more genetic information for lower cost than single-gene testing (Collins, 2010; MacConaill and Garraway, 2010; Mardis, 2011). While NGS applications will undoubtedly play a central role in fulfilling the promise of precision medicine, questions prevail about how to counsel and consent patients for NGS tests and how to prescribe risk management and follow-up for patients with complex, ambiguous, or incidental NGS test results (Green and Guyer, 2011).
Practical concerns also exist about the time, money, education, and workforce resources needed to appropriately integrate NGS into clinical practice (Ormond et al., 2010; Berg et al., 2011; Mardis, 2011; Weitzel et al., 2011; Biesecker et al., 2012; Evans and Rothschild, 2012; Domchek et al., 2013). Despite recommendations that NGS testing be phased into clinical practice within the context of careful translational research, patent law and market forces are driving the incorporation of NGS testing across the spectrum of clinical care (Green and Guyer, 2011; Azvolinsky, 2013; Domchek et al., 2013; Langreth and Pettypiece, 2013).
Little is known about experiences with NGS testing among community-based clinicians who provide GCRA services. This study explored the perceptions, experiences, and challenges related to NGS testing among GCRA clinicians from different practice disciplines and clinical settings who participate in a nationwide Clinical Cancer Genetics Community of Practice (CCGCoP) (Blazer et al., 2005, 2011).
Materials and Methods
Participants/procedure
The study employed a mixed-methods approach. A 27-item survey was sent to 235 members of the CCGCoP, comprising physicians (MDs), advanced practice nurses/physician assistants (APNs/PAs), and genetic counselors (GCs) who provide GCRA services in community settings across 46 U.S. states. All CCGCoP clinicians completed a National Cancer Institute (NCI)-funded interdisciplinary intensive course in clinical cancer genetics between the years 2001 and 2012 (Blazer et al., 2005, 2011). An email invitation with a link to the initial survey was sent to CCGCoP members on July 6, 2012, with two reminders sent within 10 days. A second survey was administered on March 8-9, 2013, to members of the CCGCoP (n = 107) who attended a 2-day continuing medical education (CME)-accredited cancer genomics conference at City of Hope, Duarte, CA.
The second survey was administered using Audience Response System (Evansville, IN) with paper-and-pencil supplement for open-ended responses. Data on clinical experiences with NGS testing were collected from January 1, 2013, through January 1, 2014, on cases presented during weekly multidisciplinary CME-accredited web-based case conferences. The conferences serve as a distance-mediated source of GCRA practice support and are attended by ∼35-50 CCGCoP members weekly (MacDonald et al., 2010; Blazer et al., 2012).
The study population comprised healthcare professionals who voluntarily participated in the CCGCoP, a CME-accredited program of cancer genetics training and continuing practice support funded by the NCI (RC4CA153828, R25CA112486). Research was conducted in an established educational setting involving recognized approaches for assessing education and longitudinal practice outcomes. Informed consent for postcourse surveys and clinical practice data collection was obtained upon course initiation.
Instrumentation
Survey questions were developed by the City of Hope clinical cancer genetics faculty (three board-certified GCs, a PhD genetics-credentialed nurse, and a medical oncologist/geneticist), entered into SurveyMonkey (Palo Alto, CA), and piloted by 12 cancer genetics clinicians. The initial survey took ∼15 min to complete and included five professional demographic questions; seven yes/no and checkbox questions related to knowledge about and use of commercially available NGS tests for cancer risk; one hypothetical case scenario question with open-ended prompt requesting the rationale for ordering/not ordering a multigene panel for a high-risk breast cancer patient; and seven rating scale questions on professional self-efficacy related to basic genetics/genomics and interpreting/counseling about single-gene and NGS tests (scale from 0 = Not Confident to 4 = Very Confident).
The second survey included a subset of questions from the initial survey focused on the use of NGS tests, the same hypothetical case question, and five self-efficacy questions (survey questions are summarized in Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/gtmb). Clinician experiences with NGS testing and test results reported during weekly case conferences were manually recorded by the City of Hope cancer genetics faculty.
Data analysis
Quantitative survey data were entered into Microsoft Excel 2007 (Microsoft, Redmond, WA) spreadsheets, audited for accuracy, and imported into Statistical Analysis Software (SAS v.9.2; SAS, Inc., Cary, NC) for analysis. Descriptive statistics were computed for yes/no, multiple choice, rating scale items, and NGS test data. Contingency table analysis was used to examine associations between initial versus second survey respondents on professional demographic characteristics and on responses to the question related to the uptake of multigene panel testing and the hypothetical case scenario question.
One-way analysis of variance (ANOVA) was conducted to compare self-efficacy responses by practice discipline. Mixed-effects ANOVA of genetic test type by sample (initial vs. second survey) was conducted to examine differences that may have occurred over time. A mixed-effects ANOVA by discipline across genetic test type (single gene, multigene, WES/WGS) examined differences across test type and interaction between test type and discipline.
Coding and thematic analysis of open-ended responses were conducted by three clinical researchers through a series of iterations, and frequencies of responses coded under each theme were tallied. Quantitative and qualitative outcomes were triangulated to increase the depth and validity of the findings (Creswell, 2003). NGS test results for cases presented during case conferences were tallied and categorized using American College of Medical Genetics guidelines (Plon et al., 2008). Cases exemplary of challenges with NGS test results were extracted from case presentation summaries.
Results
Of 235 CCGCoP members invited to participate, 38 were lost to follow-up. Professional demographic characteristics of respondents are summarized in Table 1. Of 197 members invited to participate, 94 (48%) responded to the initial survey: 27 (28.7%) were MDs, 37 (39.4%) GCs, and 30 (31.9%) APNs. Forty-seven (50%) provided GCRA in community hospitals, 19 (20.2%) in private practice settings, and 18 (19.1%) in clinical settings with academic affiliations. The majority had been providing GCRA services for more than 1 year at the time of completing the initial survey. Of 107 members who responded to the second survey (54% response rate), ∼70% had also completed the initial survey.
All respondents are members of the Clinical Cancer Genetics Community of Practice (CCGCoP).
Breakdowns/comparisons include only respondents who provided all demographic data. Chi-square analysis revealed no significant differences between initial and second survey respondents by discipline (p = 0.206) or practice setting (p = 0.220). More respondents to the first survey had 1-5 years of GCRA experience, and more respondents to the second survey had <1 year of GCRA experience (p = 0.013).
94/197 = 48% initial survey response rate; 107/197 = 54% second survey response rate.
GC, genetic counselor; GCRA, genetic cancer risk assessment.
Comparisons of demographic features of initial and second survey respondents revealed no statistically significant differences between groups based on professional discipline or practice settings (p = 0.206 and p = 0.220, respectively). While the initial survey group had significantly more GCRA experience (more likely to have 1-5 years) than did the second survey group (more likely to have less than 1 year's experience) (p = 0.013), there was no significant association between GCRA experience and discipline (p = 0.926).
Of initial survey respondents, 98% were aware of multigene panels and 86% were aware of WES/WGS tests for clinical applications. The use of panel testing increased significantly over the 8 months between the initial (29%; 27/94) and second survey (44%; 46/107); the use of WES/WGS testing did not increase significantly over the study period (p > 0.021 and p = 0.348, respectively) (Fig. 1).
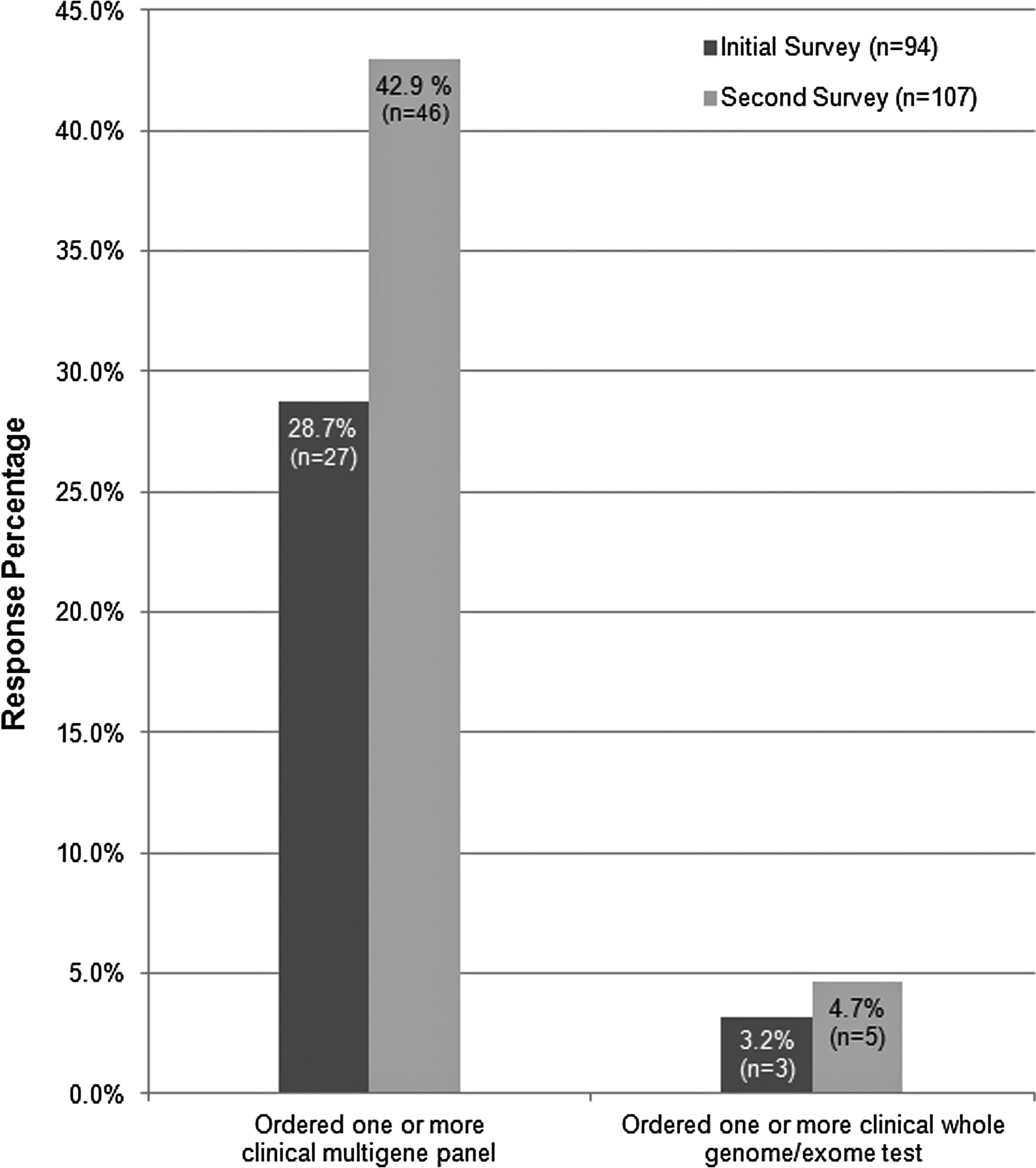
Uptake of multigene panel testing. The number of Clinical Cancer Genetics Community of Practice (CCGCoP) survey respondents who ordered one or more multigene panel tests increased significantly between July, 2012 (29%; 27/94), and March, 2013 (44%; 46/107) (p = 0.021). There was no increase in the number of WES or whole genome tests ordered over this time frame (p > 0.05). WES, whole exome.
Responses to the single-case scenario question “At this time, would you offer a multigene panel to a BRCA-negative female who was diagnosed as having triple-negative breast cancer at age 34 and has a strong family history of breast cancer?” (Fig. 2) revealed that 39% of initial and 58% of second survey respondents would offer a commercial multigene panel in this case, and 15% of initial and 9% of second survey respondents would order a panel only on a research basis. Initial survey respondents were significantly more likely to offer testing only on a research basis, while second survey respondents were more likely to offer testing if covered by insurance (p = 0.002).
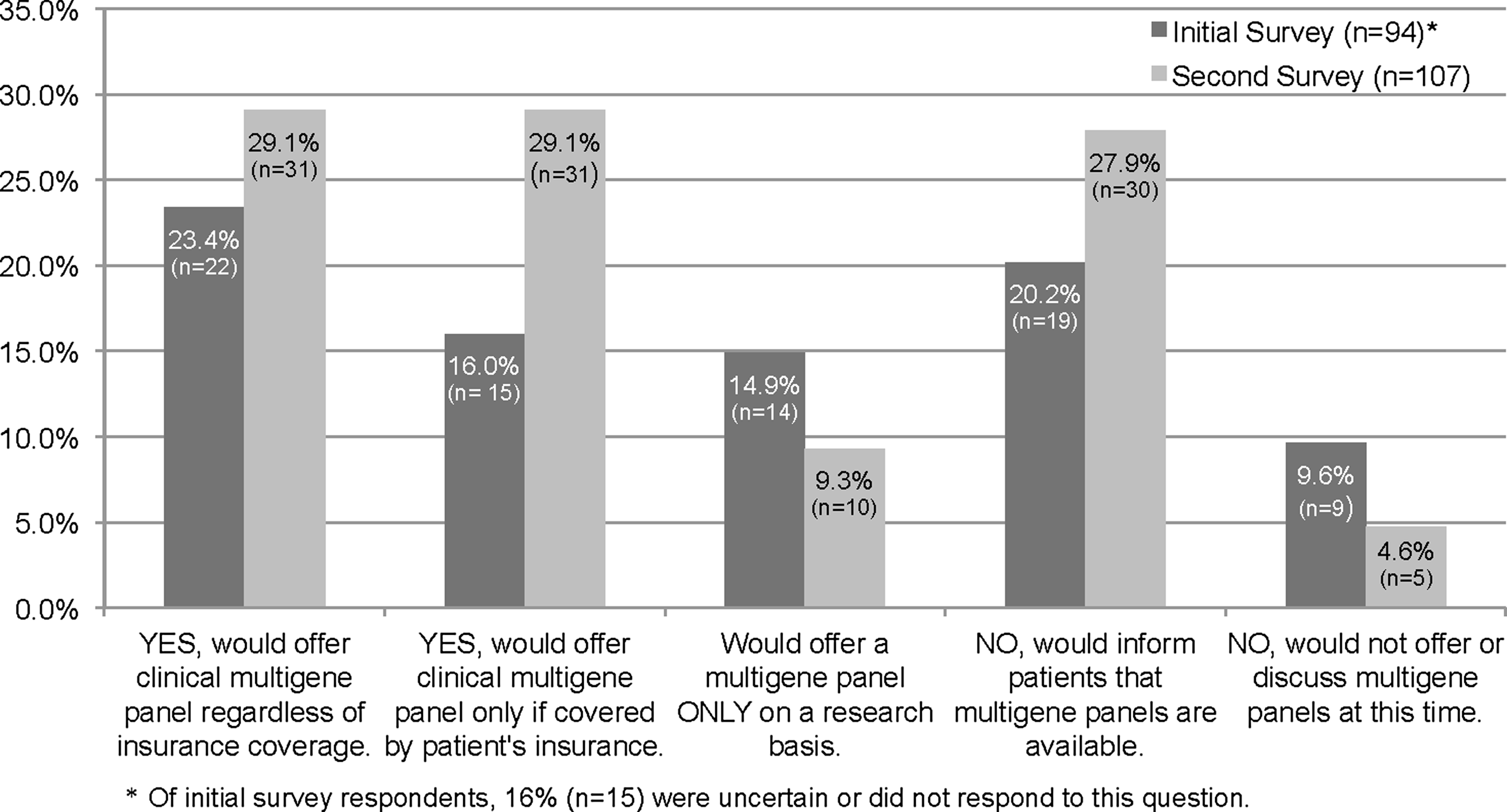
Case scenario responses. Responses to the hypothetical case scenario question, “Would you offer a multigene panel test for a BRCA-negative female who was diagnosed as having triple-negative breast cancer at age 34 and has a strong family history of breast cancer?” Initial survey respondents were significantly more likely to offer testing only on a research basis, while second survey respondents were more likely to offer testing if covered by insurance (p = 0.002).
Among respondents who would not offer panel testing, 20% of initial and 28% of second survey respondents would still inform patients about such tests, and 10% and 5%, respectively, would neither offer nor inform patients about NGS testing. The remaining respondents (16% initial survey only) were uncertain or did not respond to this question.
Open-ended responses about the case scenario are coded, tallied, and summarized with representative quotes in Table 2. Among clinicians who would offer a multigene panel for the patient in the scenario, potential knowledge and health benefit to patients/families (n = 14), need to better understand the contribution of germ line genetics to cancer risk (n = 12), and cost and time-saving benefits (n = 10) were most frequently cited. Among respondents who would not order a panel, the most frequently described reasons were unclear clinical utility (n = 26), lack of knowledge/professional expertise (n = 24), and financial cost to patient/concerns about insurance coverage (n = 23).
Number of responses on open-ended survey prompts documented within each category of influencing factor.
VUSs, variants of uncertain significance.
Responses to questions assessing self-efficacy with interpreting/counseling about different test results (Fig. 3) revealed that clinicians were very confident overall about interpreting/counseling about single-gene test results (mean = 4.8), but significantly less confident about variants of uncertain significance (VUSs) (mean = 4.45), multigene panel (mean = 2.86), or WES/WGS results (mean = 2.19) (p < 0.001 for all comparisons). Comparisons of self-efficacy scores by practice discipline revealed no significant differences between MDs, GCs, and APNs/PAs in confidence related to interpreting/counseling about single-gene deleterious results. GCs had greater confidence than MDs and APNs/PAs about interpreting/counseling about VUSs (p = 0.003), and MDs and GCs had greater confidence than APNs/PAs with interpreting/counseling about panels and WES/WGS results (p < 0.001 for all comparisons).
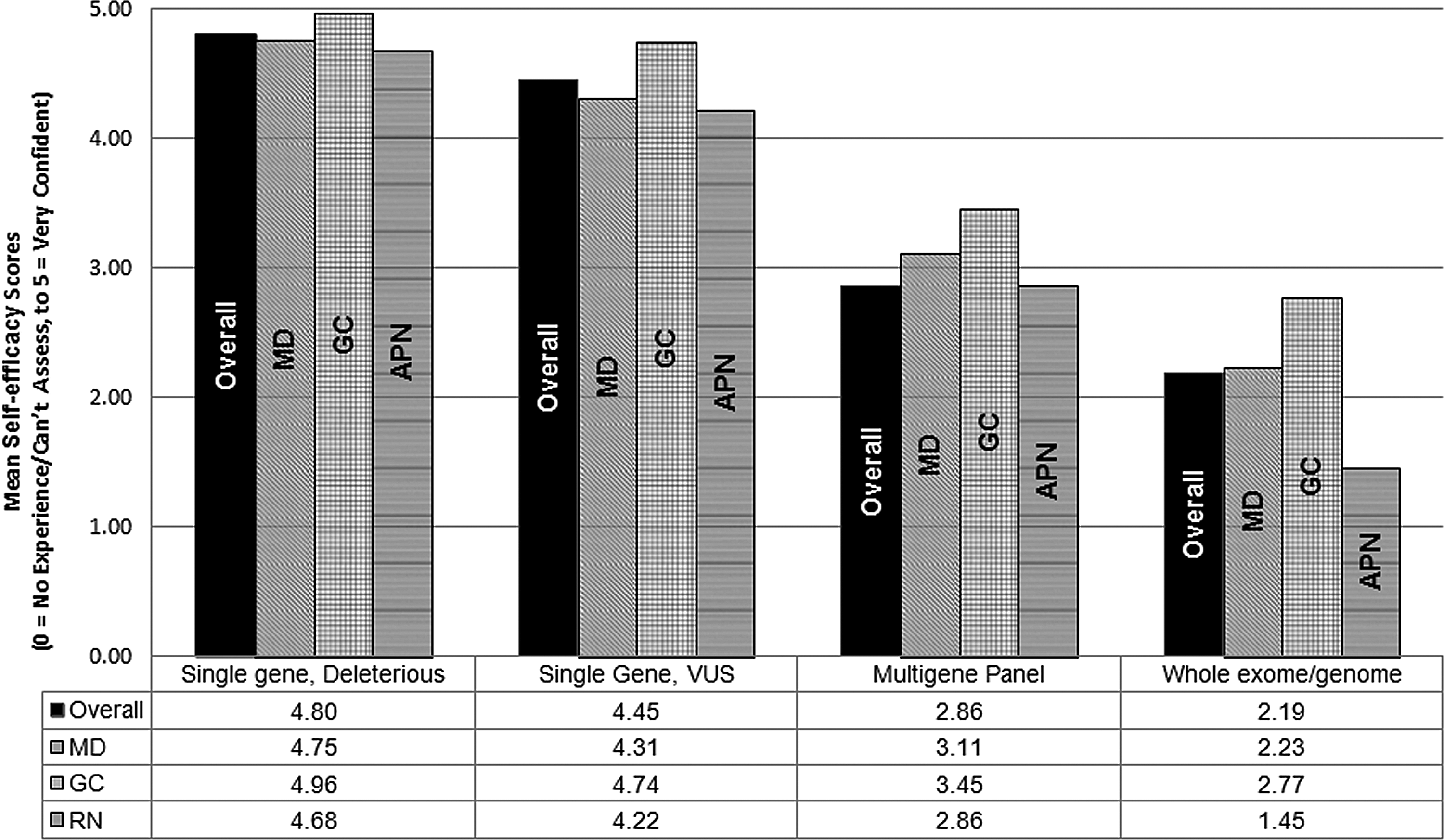
Clinician self-efficacy with interpreting and counseling about different types of genetic test results. Overall scores demonstrated a high level of confidence with interpreting/counseling about single-gene results, and significantly less confidence (in descending order) about variants of uncertain significance (VUSs), multigene panel, and WES/whole genome test results (p < 0.001 for all comparisons). By-discipline comparisons revealed no significant differences in interpreting/counseling about single-gene results; GCs had more confidence than MDs and APNs/PAs with interpreting/counseling about VUSs (p = 0.003); MDs and GCs had greater confidence than APNs/PAs with interpreting/counseling about multigene panel and WES/WGS results (p < 0.001 for all comparisons). WGS, whole genome sequence.
Of 668 cases presented during case conferences between January 1, 2013, and January 1, 2014, commercial multigene panels were ordered for 216 (32%) cases. Of these, 12 tests were cancelled due to denial for insurance coverage. Of 204 panels processed, 37 yielded positive (deleterious) results—22 (11%) in high-penetrance genes associated with syndromes that have risk management guidelines and 15 (7%) in low/moderate-risk genes for which the phenotype and/or management guidelines are not well established; 112 VUSs were reported in 88 (43%) cases, including 23 cases with 2 or more VUSs and 4 cases with a deleterious mutation; 2 cases had inconclusive results and 77 (38%) had uninformative-negative results (Fig. 4).
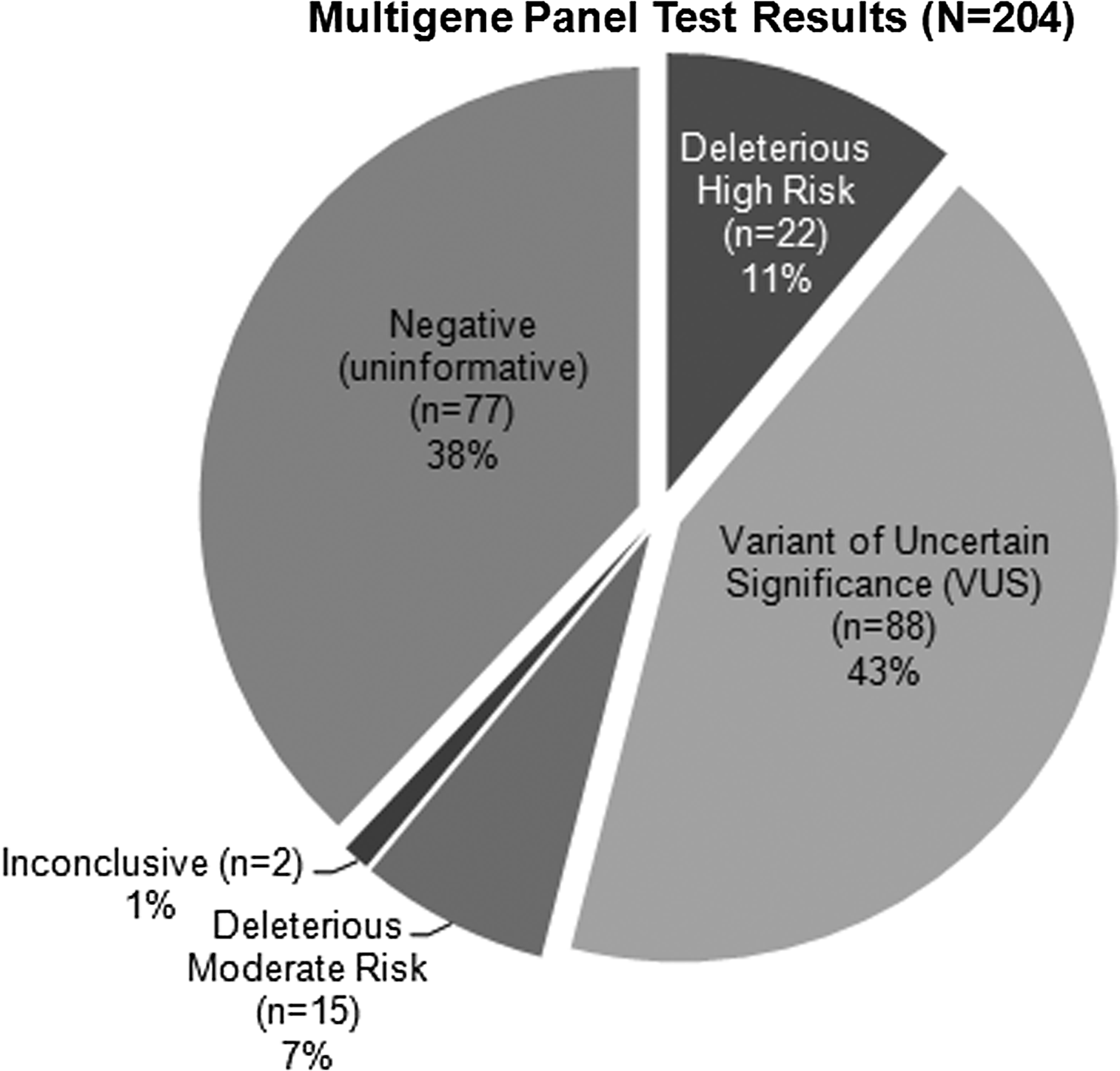
Summary of multigene panel results presented during case conferencing. Two hundred four commercial multigene panel tests were presented by community clinicians during web-based case conferences from January 1, 2013, through January 1, 2014. Twelve additional tests were ordered, but cancelled due to denial for insurance coverage.
Panel testing yielded complex or challenging results for a number of cases. For example, in one case, the NBN1 alteration c.643C>T (p.Arg 215 Trp), recognized as a deleterious mutation in the context of Nijmegen breakage syndrome, was reported on a panel result as deleterious by one laboratory and as a special interpretation result that was later recategorized as a VUS by another laboratory. In another case, a CDH1 duplication was reported as a VUS by one laboratory, but subsequent panel testing by a different laboratory that included CDH1 did not report the variant.
A number of cases revealed incidental findings, where deleterious mutations were identified in genes on prebundled commercial panels that did not explain the clinical phenotype, such as a 48-year-old male with colorectal cancer and family history of oligopolyposis found to have a BARD1 alteration c.1690C>T (p.Gln564*). Classified as clinically actionable by the vendor, the result, which is associated with breast and ovarian, but not colorectal, cancer risk, did not explain the patient's phenotype and had no bearing on his medical management, and it prompted concerns about its significance to other family members.
Discussion
As rapid advances in genomic technologies bring us closer to the era of precision medicine, clinicians are facing the challenge of responsibly integrating these technologies into practice. To our knowledge, this is the first study to offer insights related to NGS testing among clinicians who deliver GCRA services in community settings, outside of a research context. Despite low reported self-confidence with interpreting/counseling about multigene panels (2.86 on a five-point scale) and stated concerns about lack of evidence to inform clinical utility, this study documented a doubling of NGS testing uptake within 8 months among CCGCoP clinicians.
Counter to recommendations by the National Human Genome Research Institute and other key stakeholder groups that NGS testing for less well-defined genes should take place in clinical research settings before diffusion into clinical practice, many surveyed in this study began incorporating multigene panels into their practices in the absence of published data on penetrance or clinical outcomes and well before initial reports on experiences from academic centers (Khoury et al., 2011; Walsh et al., 2011; Pritchard et al., 2012; Selkirk et al., 2012; Domchek et al., 2013; Euhus and Robinson, 2013; Gray et al., 2014; Hiraki et al., 2014; Kurian et al., 2014; Mauer et al., 2014).
Beyond the potential time and cost-saving advantages of ordering multigene panels for patients whose phenotype/family history suggests multiple differential diagnoses, a confluence of other factors are likely contributing to the steady increase in clinical NGS testing. These include the invalidation of BRCA-related patents by the Supreme Court, which allowed a number of commercial laboratories to incorporate BRCA1 and BRCA2 into comprehensive cancer panels; aggressive marketing by these laboratories to community clinicians; and a surge in referrals for GCRA prompted by globally publicized participation in BRCA testing by celebrity Angelina Jolie (Azvolinsky, 2013; Borzekowski et al., 2014; Langreth and Pettypiece, 2013).
Despite the cited concerns regarding insurance coverage among initial survey respondents, all but 12 of the panel cases tracked in this study were authorized for coverage using CPT billing codes for BRCA or the mismatch repair (MMR) genes associated with Lynch syndrome, a billing practice that evolved over the course of the study. However, 10 of the 12 cases denied insurance coverage for panel testing were denied because the patient's insurance had previously covered BRCA or MMR gene testing. Consequently, clinicians who might have initiated testing with single-gene analysis began to initiate testing with multigene panels due to concerns that coverage for single-gene testing would preclude coverage for additional testing later.
The spectrum of mutations identified through NGS testing in this study parallel those emerging from the clinical research setting, and likewise raise several of the concerns voiced by the research community (Kurian et al., 2014; Mauer et al., 2014). These include challenges associated with how to interpret, counsel, and follow patients with deleterious mutations in multiple genes and/or in genes lacking evidence for clinical actionability; how to prepare, counsel, and manage risk in the setting of incidental findings in high-penetrance genes where there is no evidence of genotype/phenotype correlation in the patient or family; and how to address the compounded finding of VUSs, particularly for lesser known genes.
The challenges associated with interpreting/counseling patients about VUSs with single-gene testing are well recognized (Petrucelli et al., 2002; Meiser, 2005; Patenaude et al., 2006; Vos et al., 2008, 2011; Cypowyj et al., 2009; O'Neill et al., 2009; Murray et al., 2011; Culver et al., 2013). Self-confidence about single-gene VUS counseling in this study was high, likely because CCGCoP members have GCRA training and access to case-based support. Accurate VUS interpretation/counseling is likely to be more challenging for clinicians without GCRA training or experience. The increasing volume of VUSs reported with NGS testing also raises concerns about the logistics of recontacting patients and updating medical records as the plethora of VUSs are reclassified. Of greater concern, some test results tracked in this study prompted unanticipated challenges due to different variant classification procedures and potential differences in the analytic sensitivity of tests between laboratories.
Even among respondents who endorsed multigene panels for their potential to elucidate the contribution of germ line genomics to the etiology of cancer, several expressed concerns. As one MD respondent suggested, “I like the idea of NGS panels, but I wish there was a way to select the genes in the panel, or opt out of genes that have a lower likelihood of being involved.” While a la carte reporting might minimize challenges associated with incidental findings or alterations in genes that lack sufficient clinical utility, the responsibility of selecting which genes to include in a customized panel can pose a different set of challenges for the clinician, and selecting against rare and moderate-risk genes will delay efforts to characterize them.
Complexities and challenges aside, uptake of multigene panel testing continues to rise. Currently, upward of 80% of cases presented during the weekly CCGCoP conference series have had panel testing. Moreover, while few respondents reported ordering WES analysis for GCRA over the course of the study, most were aware of the commercial availability of WES for clinical applications, and adoption of WES/WGS for cancer risk is on the horizon (Biesecker, 2012; Ku et al., 2012; Hilbers et al., 2013; Dewey et al., 2014; Feero, 2014).
With growing pressure from commercial laboratories to order NGS panels, the issue is no longer when or by whom, but how to support clinicians employing NGS testing for GCRA. The clinicians in this study most frequently described the following needs during NGS case presentations:
• Access to evidence-based resources at the point of care to support interpretation, counseling, and risk management guidelines that incorporate NGS results. • Skills and knowledge to interpret NGS test reports and engage the clinical laboratories to address questions about complex or ambiguous results, testing methods/sensitivity, and variant classification approaches. • Mechanisms for long-term patient follow-up for complex, ambiguous, indeterminate, or uninformative test results. • Resources to support clinician contributions to the large-scale data collection needed to determine the clinical significance of low/moderate-penetrance genes, VUSs, and alterations in multiple genes. • Continuing education and point-of-care learning resources for clinicians providing GCRA and accessible education resources for other healthcare professionals engaged in the care of patients seeking or eligible for GCRA.
Limitations
As the study was conducted on a convenience sampling of clinicians with GCRA training and experience, findings may not be generalizable to the larger community of clinicians. While there was a difference between initial and second survey respondents in the length of GCRA practice experience, all participants in the study were actively engaged in delivering GCRA services at the time they completed the surveys. We considered it most important that the survey participants be actively engaged in GCRA to be able to provide responses based on experiences, but we do not believe that the differences between the initial and second survey respondents significantly contributed to the study findings.
Seventy percent of second survey respondents completed the initial survey; however, the surveys were anonymous, so it was not possible to conduct respondent-specific comparisons of initial and second survey responses. Case tracking was limited to cases presented in a multidisciplinary case conference series, where cases presented may be more complex. While it may be expected that experienced clinicians would be early adopters of new genetics/genomics tools, findings suggest that experienced clinicians are proceeding with caution, arguably because they recognize the limits of the evidence base and their own preparedness to navigate the challenges of complex or novel NGS test results. The challenges associated with NGS testing may be magnified among clinicians who lack special training or access to point-of-care resources from academic health centers such as those available to this community of practice.
Conclusions
The findings of this study document that despite practical concerns, there is an increasing uptake of NGS testing for cancer risk among community-based clinicians engaged in GCRA practice. Complex and ambiguous results from multigene panel tests conducted by these clinicians reflect the concerns articulated by the genomics/ethical, legal, and social implications (ELSI) research community and illustrate the need to close gaps in translational research on genes included on panels, engage clinical laboratory expertise, and improve approaches to recontacting patients over time. Finally, findings from this study support the need for workforce training and practice-based support for clinicians incorporating NGS into GCRA practice and for mechanisms to engage clinicians as contributors to the development of new GCRA practice models and research defining the contribution of genomic variation to cancer risk.
Footnotes
Acknowledgments
Research reported in this publication was supported, in part, by the NCI of the National Institutes of Health under Award Numbers, RC4CA153828, R25CA112486 (PI: J.N.W.), and R25CA171998 (PIs: K.R.B. and J.N.W.). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors wish to acknowledge Dr. Deborah MacDonald and Carin Espenschied for assistance with initial survey development and pilot data analysis; Tracy Sulkin for survey dissemination data collection; Lily Van Tongeren for manuscript preparation and submission; Sharon Sand, Kai Yang, and Benjamin Weissman for data management and pilot analysis; and the members of the CCGCoP, who are dedicated to best practices in cancer genetics risk assessment and patient care.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.