
Abstract
Objective: In this study, we investigated two VKORC1 gene polymorphisms, -1639G/A and 1173C/T, for effects on warfarin maintenance dosage in valvular heart disease (VHD) patients after cardiac valve replacement (CVR). Methods: A total of 219 VHD patients receiving warfarin therapy after CVR surgery were recruited to this study between June 2010 and December 2013. Basic clinical data, prothrombin time, warfarin maintenance dose, and blood samples were collected from all patients. Polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) analyses were used to analyze the VKORC1 -1639G/A and 1173C/T polymorphisms. SPSS version 19.0 software was used for statistical analysis of the data. Results: Patients with either the AG+or GG genotype (n=32) of the VKORC1 -1639G/A polymorphism required a significantly higher warfarin dose compared to patients with the AA genotype (n=187) (4.36±1.03 mg/day vs. 2.95±0.94 mg/day; p<0.001). Similarly, patients carrying the CT genotype (n=28) of the VKORC1 1173C/T polymorphism also required a significantly higher warfarin dose compared to those with the TT genotype (n=191) (4.19±0.99 mg/day vs. 3.00±0.94 mg/day; p<0.001). Linear regression analysis showed that gender, age, weight, and VKORC1 -1639G/A and 1173C/T polymorphisms were correlated with individual differences in warfarin maintenance dose (all p<0.05). Conclusion: We present evidence that the two VKORC1 polymorphisms, -1639G/A and 1173C/T, are key genetic factors influencing individual differences in warfarin maintenance dose in VHD patients who underwent CVR. Gender, age, and weight also independently correlated with warfarin maintenance dose.
Introduction
W
Due to the narrow anticoagulant therapeutic index, the significant interindividual differences in clinical efficacy, and the adverse side effect, warfarin maintenance dose is very difficult to establish in patients, with inadequate anticoagulation due to suboptimal dosage resulting in embolism and overdose linked to hemorrhage (Fung et al., 2012). The effectiveness and safety of warfarin are measured by prothrombin time and thromboplastin reagents and expressed as an international normalized ratio (INR) designed to standardize the results (Jacobson, 2012).
Multiple clinical and environmental factors contribute to the variability in warfarin maintenance dose, including age, gender, body weight, dietary intake, comorbidities, comedications, and variations in pharmacokinetics and pharmacodynamics (Jorgensen et al., 2012). Apart from these environmental factors, recent efforts also identified genetic determinants influencing warfarin dose requirements (Sconce et al., 2005). In this context, a previous study showed that VKORC1 gene polymorphisms modulate warfarin efficacy (Mushiroda et al., 2006).
VKORC1 is required in recycling of vitamin K 2, 3-epoxide to active vitamin K hydroquinone, a reduced vitamin K form that functions as a cofactor necessary for the activation of vitamin K-dependent clotting factors (Lee et al., 2006). VKORC1 mediates the γ-carboxylation of vitamin K-dependent proteins, coagulation factors II, VII, IX, and X, and hemostatic proteins C, S, and Z (Perez-Andreu et al., 2012). Not surprisingly, VKORC1 is the main target of anticoagulants used in the treatment of several thrombotic diseases such as AF, myocardial infarction, CVR, stroke, and venous thrombosis (Matagrin et al., 2013). A few SNPs of VKORC1 result in amino acid substitutions in the VKORC1 protein and have a significant clinical impact on warfarin maintenance dose in patients (Ragia et al., 2013).
In this context, two common VKORC1 polymorphisms, 3730G>A located in the 3′-untranslated region and 1173C>T located in intron 1, are linked to interindividual differences in warfarin dose, with a mean warfarin dose found to be higher in patients carrying CC genotype of VKORC1 1173C>T compared to patients with CT or TT genotypes (Zhu et al., 2007). The VKORC1 -1639G>A (rs9923231) polymorphism is located in the VKORC1 promoter and results in a lower expression and activity of VKORC1 in subjects carrying AA genotype (Yin and Miyata, 2007). Moreover, in T2DM patients, VKORC1-1639G>A polymorphism exhibits a strong association with an increased risk of atherosclerosis caused by increased calcification (Tavridou et al., 2011). Importantly, VKORC1 -1639G>A is an important indicator to predict the response to warfarin therapy (Vear et al., 2014).
In this study, we investigated the correlations between VKORC1 polymorphisms, -1639G/A and 1173C/T, and warfarin maintenance dose to understand the influence of genetic factors on adjusting warfarin maintenance dose and to provide a valuable clinical indicator for safe warfarin dosage in CVR patients.
Materials and Methods
Subjects
In this study, 219 CVR patients (mean age, 46.61±9.64 years), including 98 males and 121 females, on warfarin therapy were recruited at Henan Provincial Corps Hospital of Chinese People's Armed Police Force, between June 2010 and December 2013. Patient's inclusion criteria of the qualified testers in this study were as follows: CVR patients were on a stable dose of warfarin and examined with INR (ranges, 2.0-3.0) once a month. Exclusion criteria of the qualified testers were as follows: (1) a history of hepatic disease or serum transaminase levels 1.5 times higher than normal levels; (2) impaired nephron function with serum creatinine (Scr) >120 μM; (3) patients taking INR-related medication such as aspirin, heparin, and vitamin K or medicines influencing the pharmacokinetics of warfarin such as amiodarone, barbital, rifampicin, and inhibitors or inducers of cytochrome P450.
Clinical data collected included name, sex, age, weight, prothrombin time, diagnoses, surgery method (Bentall surgery, aortic valve replacement [AVR], mitral valve replacement [MVR], and double valve replacement [DVR]), prescribed dosage of warfarin and combined medication, intake of food rich in vitamin K, and smoking habits. In addition, patient contact information was obtained and side effects of warfarin were documented. Warfarin maintenance dose refers to the mean dose of warfarin with the INR ranging from 2.0 to 3.0 in a continuous sequence, recorded once every 7 days.
This study was approved by the Ethics Committee of Henan Provincial Corps Hospital of Chinese People's Armed Police Force, All study participants had no consanguinity and miscegenation, and they all provided written informed consent.
Genotyping
Heparin-treated blood samples (2 mL) were collected from all patients and stored at −20°C. The genomic total DNA for genotyping was extracted using the Genomic DNA Extraction Kit (Beijing SBS Genetech Co., Ltd., China) and stored at −20°C. The genotypes were analyzed by polymerase chain reaction-restriction fragment length polymorphism (PCR) and all VKORC1 -1639A/G and 1173C/T primers were synthesized by Invitrogen (Invitrogen Trading Co. Ltd., Shanghai, China).
The forward and reverse primers for -1639G/A were 5′-GCCAGCAGGAGAGGGAAATA-3′ and 5′-AGTTTGGACTACAGGTGCCT-3′, respectively, and for 1173C/T were 5′-TAGGACTGT-CAACCCAGT-3′ and 5′AGTGACATG-GAATCCTGA-3′, respectively. The PCR (25 μL) contained the following: 2.0 μL template DNA, 0.5 μL 100 μM forward and reverse primers for -1639G/A (1 μL 100 μM forward and reverse primers for 1173C/T), 2.5 μL 10×PCR buffer (containing Mg2+), 2 μL dNTP 2.5 mM, and 0.25 μL TaqDNA polymerase and double distilled water (pH 8.2). PCR steps were as follows: initial denaturation at 95°C/5 min, followed by 35 cycles of denaturation at 94°C/30 s, annealing at 60°C/30 s (annealing at 55°C/30 s for 1173C/T), and extension at 72°C/45 s. The final extension was carried out at 72°C/7 min.
The PCR products of -1639G/A and 1173C/T were digested by BcnI and HinfI restriction enzymes, respectively. The restriction enzyme reaction contained the following: 8 μL of PCR product, 2 μL buffer, 8.5 μL dH2O, and 1.5 μL of restriction enzymes (10 U/μL) at 37°C overnight. The digested products (9 μL) were analyzed on 2.5% w/v agarose gels electrophoresed at 120 V for 30 min (with bromophenol blue as an indicator and ethidium bromide as a staining agent) and observed under ultraviolet light.
Genotype analysis
The PCR product size for VKORC1 -1639A/G was 273 bp. Wild-type homozygous GG digested by BcnI resulted in two fragments of 198 and 75 bp. The mutant heterozygote AG yielded three fragments of 198, 75, and 273 bp after restriction digestion, while the AA mutant homozygotes produced one 273 bp fragment due to the lack of MspI restriction site. The PCR product size for VKORC1 1173C/T was 335 bp. Wild type (CC type) cannot be digested by HinfI, resulting in two fragments (251 and 84 bp), the mutant heterozygotes (TC) showed four fragments (251, 205, 84, and 45 bp), and the mutant homozygotes (TT type) displayed three fragments (205, 84, and 45 bp) (Fig. 1).
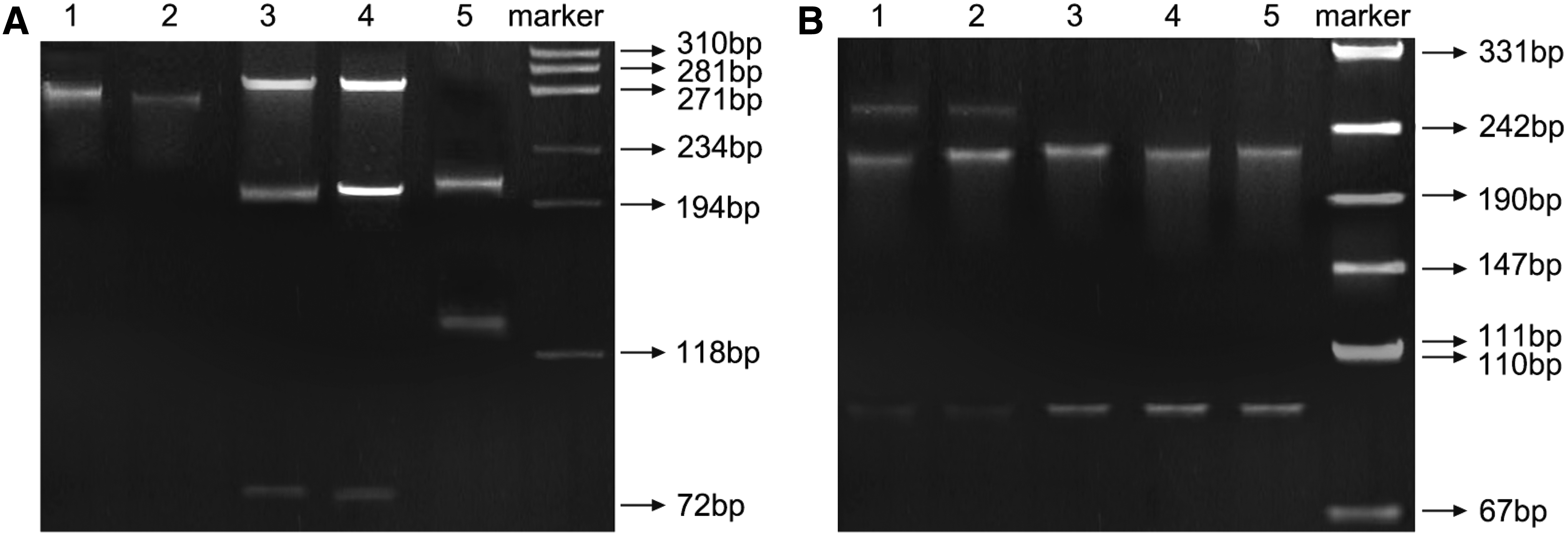
Electrophoretogram of polymerase chain reaction (PCR) products of VKORC1 -1639
Statistical analyses
The chi-square test was used to verify gene distribution in conformity with the Hardy-Weinberg equilibrium and to compare gender differences between different genotypes. The ANOVA test was used to detect differences in warfarin maintenance dose and clinical features between the different genotypes. Linear regression and stepwise regression were used to analyze the correlation between the dose of warfarin and the variables. All analyses were performed using the SPSS version 19.0 software. Data are presented as mean±standard deviation (SD). A two-tailed significance level was used in all tests and a p-value less than 0.5 was considered statistically significant.
Results
Patient characteristics
A total of 219 CVR patients were enrolled in this study at our hospital. The patient group contained 98 males (44.7%, mean age, 45.54±9.85) and 121 females (55.3%, mean age, 47.48±9.46). The average weight for all the enrolled patients was 58.62±10.19 kg, and for male patients the average weight was 62.51±10.13 kg, while in female patients the average weight was 55.47±9.12 kg. The average height was 161.70±7.72 cm for all the enrolled patients, 166.78±6.35 cm for male patients, and 157.59±6.18 cm for female patients. Among the 219 patients, 45 patients were smokers (20.5%) and 174 were nonsmokers (79.5%), 13 patients (5.9%) were receiving Bentall, 48 patients (21.9%) were receiving AVR, 66 patients (30.1%) were receiving MVR, and 92 patients (42.0%) were receiving DVR.
Genotype and allele frequencies
The genotype and allele frequencies of VKORC1 -1639G/A and 1173C/T showed no significant deviation from the Hardy-Weinberg equilibrium (both p>0.05), suggesting their representativeness of the population. The frequencies of distribution of AA, AG, and GG genotypes of VKORC1 -1639G/A were 85.4% (187/219), 13.7% (30/219), and 0.9% (2/219), respectively, and the allele frequencies of A and G of VKORC1 -1639G/A were 92.2% and 7.8%, respectively. The frequencies of distribution of TT, CT, and CC genotypes of VKORC1 1173C/T were 87.2% (191/219), 12.8% (28/219), and 0.0% (0/219), respectively (CC genotype of 1173C/T is rare in the population and the frequency of CC genotype in 1173C/T in our study was 0), and the allele frequencies of C and T of VKORC1 1173C/T were 6.4% and 93.6%, respectively (Table 1).
Warfarin maintenance dose and patient characteristics
In this study, the average maintenance dose of warfarin was 3.04 mg/day. Due to the low number of GG genotype carriers of VKORC1 -1639G/A (n=2), the GG genotype frequency was combined with the frequency of AG, as AG+GG genotype. The average maintenance dose of warfarin in AG+GG genotype carriers (n=32) was significantly higher than the AA genotype carriers (n=187) (4.36±1.03 mg/day vs. 2.95±0.94 mg/day, p<0.001).
However, baseline clinical characteristics such as gender, age, weight, height, and smoking showed no statistical significance between the AG+GG genotype and AA genotype (all p>0.05). Warfarin maintenance dose in CT carriers of VKORC1 1173C/T (n=28) was significantly higher than the TT patients (n=191) (4.19±0.99 mg/day vs. 3.00±0.94 mg/day, p<0.001). However, the baseline clinical characteristics such as gender ratio, age, weight, height, and smoking also showed no differences between the CT genotype and TT genotype (all p>0.05) (Table 2).
Linear regression analysis of warfarin maintenance dose
Linear regression analysis was used to obtain correlations between gender, age, height, weight, smoking, VKORC1 polymorphisms, and warfarin maintenance dose. Gender, age, weight, and VKORC1 -1639G/A and 1173C/T gene polymorphisms significantly correlated with warfarin maintenance dose (all p<0.05), while no statistical correlation was found between height, smoking status, and warfarin maintenance dose (both p>0.05) (Table 3). When stepwise logistic regression analysis was performed for each gender separately, VKORC1 -1639G/A, VKORC1 1173C/T, and weight significantly correlated with individual differences in warfarin maintenance dose in male patients, but in female patients, VKORC1 -1639G/A, VKORC1 1173C/T, and age significantly correlated with individual differences in warfarin maintenance dose (all p<0.05) (Table 4).
R2, determination coefficient; adjusted R2, correction coefficient.
R2, determination coefficient; adjusted R2, correction coefficient.
Discussion
In this study, we obtained correlations between VKORC1 -1639G/A and 1173C/T gene polymorphisms and the individual differences in relation to warfarin maintenance dose in a group of 219 patients who underwent CVR. Our results showed tight correlations of VKORC1 -1639G/A and 1173C/T gene polymorphisms with warfarin maintenance dose. The average maintenance dose of warfarin in carriers of VKORC1 -1639G/A AG+GG genotype was significantly higher than the carriers of AA genotype. The warfarin maintenance dose in carriers of CT genotype of VKORC1 1173C/T was significantly higher than the TT carriers.
Warfarin inhibits the vitamin K cycle and prevents activation of coagulation factors II, VII, IX, and X in the liver. Thus, warfarin dose requirement is also related to genes encoding other proteins participating in the vitamin K cycle (Cabral et al., 2013; Solvik et al., 2014). VKORC1 is a key enzyme in vitamin K recycling and its inhibition prevents generation of reduced vitamin K, suppressing the activation of vitamin K-dependent coagulation factors (de Visser et al., 2011; Harrington et al., 2011).
VKORC1 -1639G>A polymorphism is located in the promoter and regulates VKORC1 expression, directly affecting warfarin maintenance dose. In this study, higher warfarin maintenance dose in the AG+GG genotype, compared to AA genotype, showed that the VKORC1 promoter mutation correlated with a low warfarin dose and high warfarin sensitivity. The VKORC1 -1639A/G promoter polymorphism was in linkage disequilibrium with the VKORC1 1173C/T intronic polymorphism and may explain why the 1173 TT genotype required a lower average daily dose compared to the CT genotype (Limdi et al., 2008; Yuan et al., 2005).
Consistent with our results, Liang et al. (2012) found that the AG genotype of VKORC1 -1639G>A SNP was associated with a higher maintenance dose than the AA genotype. D'Andrea et al. (2005) also demonstrated that the mean warfarin dose required was higher in patients carrying the CC genotype of VKORC1 1173 compared to patients carrying the CT or TT genotypes.
The results of our linear regression analysis further confirmed the influence of VKORC1 -1639G/A and VKORC1 1173C/T polymorphisms on the observed individual differences in the warfarin maintenance dose. Other factors such as gender, age, and weight may also play a role as independent factors in influencing the interindividual differences in warfarin dose. In this context, Miao et al. (2007) demonstrated significant contributions of age, weight, and the VKORC1 genotype on individual differences in warfarin maintenance dose. Interestingly, Garcia et al. (2005) found that the mean warfarin dose requirement declined with age and may be linked to inadequate anticoagulation in younger patients, while resulting in overdose in elderly patients.
In our study, a further stepwise logistic regression analysis based on gender revealed the different affects of VKORC1 polymorphisms on warfarin dosage requirements. In male patients, VKORC1 -1639G/A, VKORC1 1173C/T, and weight significantly correlated with individual differences in warfarin maintenance dose, while in female patients, VKORC1 -1639G/A, VKORC1 1173C/T, and age were the significant factors linked with individual differences in warfarin maintenance dose.
In conclusion, VKORC1 -1639G/A and VKORC1 1173C/T gene polymorphisms are powerful determinants of warfarin maintenance dosage carriers of AG+GG genotype of VKORC1 -1639G/A that require a higher warfarin maintenance dose compared to the AA genotype. Similarly, carriers of CT genotype of VKORC1 1173C/T required a significantly higher warfarin maintenance dose than patients carrying TT. However, although VKORC1 polymorphisms may be the critical factors influencing interindividual differences, our study revealed that gender, age, and weight were also independent factors influencing warfarin maintenance dose. Our stepwise logistic regression analysis showed gender-based affects of VKORC1 polymorphisms on warfarin dosage requirements.
However, this study included only the Chinese population, thus our conclusion may be influenced by variations due to ethnic differences. Furthermore, although VKORC1 gene polymorphisms appeared to be the determining factors, other related genes also might influence warfarin maintenance dose and will need to be closely examined in future studies. In this study, we analyze both genetic and environment factors that affect warfarin dose, and our results may provide valuable tools to aid in reducing the side effects in patients on warfarin prescription.
Footnotes
Acknowledgments
We would like to thank our researchers for their hard work and reviewers for their valuable advice.
Author Disclosure Statement
No competing financial interests exist.