
Abstract
Aims:
Poly (ADP-ribose) polymerase-1 (PARP-1) plays an important role in the repair of damaged DNA and has prognostic significance in a variety of human malignancies. However, little is known about its expression levels and clinical implication in patients with acute myeloid leukemia (AML).
Materials and Methods:
Quantitative reverse transcription-polymerase chain reaction was done to evaluate PARP-1 expression levels in the bone marrow of 65 patients with non-M3 AML and 54 healthy counterparts. The correlation of PARP-1 expression with clinicopathological features of non-M3 AML patients was also analyzed.
Results:
Non-M3 AML patients have higher PARP-1 expression than the healthy controls (p < 0.01). Patients with adverse cytogenetic risk have higher PARP-1 expression than other cytogenetic risk groups (p = 0.004). The PARP-1 median expression level divided AML patients into PARP-1 low-expressed and PARP-1 high-expressed groups. High expression levels of PARP-1 were associated with worse overall survival (OS) (p = 0.01) and relapse-free survival (RFS) (p = 0.005). Moreover, multivariate analysis revealed that high PARP-1 expression was an independent risk factor for both OS and RFS.
Conclusions:
Our results suggest that PARP-1 overexpression may define an important risk factor in non-M3 AML patients and PARP-1 is a potential therapeutic target for AML treatment.
Introduction
P
PARP-1 overexpression has been reported in different malignancies, including breast cancer (Bieche et al., 2013), hepatocellular carcinoma (Nomura et al., 2000), gastric cancer (Liu et al., 2016), and some types of hematologic malignancies (Gaymes et al., 2009; Diamantopoulos et al., 2017). Besides, its overexpression associates with poor prognosis (Nomura et al., 2000; Bieche et al., 2013; Chow et al., 2013). It has been shown that inhibition of PARP-1 suppresses tumorigenic growth through various mechanisms, including selective killing of tumor cells deficient in homologous recombination components, tumor-related gene deregulation, and induction of apoptosis (Cockcroft et al., 2006; Tong et al., 2009).
Conflicting results have been reported regarding the PARP-1 roles in distinct hematologic malignancies such as acute lymphoblastic leukemia (ALL) or chronic lymphocytic leukemia (CLL), mainly due to the multiple functions of PARP-1 protein. Although in children with ALL overexpression of PARP-1 is correlated with a poor therapeutic response (Kruk et al., 2015), in CLL patients PARP-1 seems to mediate apoptosis (Diamantopoulos et al., 2014). In acute myeloid leukemia (AML) cells, PARP-1 inhibition shows antiproliferative and proapoptotic effects. Furthermore, it has been shown that pharmacological inhibition of PARP-1 delays disease progression and increases survival in AML in vivo (Wang et al., 2015).
It has been shown that excessive proliferation and oxidative stress may result in DNA damage accumulation that subsequently activates DNA damage response gene such as PARP-1 (Esposito and So, 2014). Furthermore, abnormal response to DNA damage in AML patients may affect progression of the disease and leads to refractory response to standard chemotherapeutic drugs (Esposito and So, 2014).
In this study, we investigated the correlation between PARP-1 mRNA levels and clinicopathological characterizations of non-M3 AML patients. Our results provide a better understanding about the roles of PARP-1 in development and progression of AML.
Materials and Methods
Patients
Sixty-five bone marrow (BM) samples from newly diagnosed non-M3 AML patients or samples from a recent study (Pashaiefar et al., 2018) were investigated. All patients had diagnosis of de novo non-M3 AML at our center. The patients were diagnosed and classified based on French-American-British (FAB) and World Health Organization (WHO) criteria (Bennett et al., 1985; Vardiman et al., 2009). The clinical and laboratory data of the patients are shown in Table 1.
BM, bone marrow; CR, complete remission; FAB, French-American-British; NR, nonresponse; WBC, white blood cell.
All patients were treated as previously described (Pashaiefar et al., 2018), including induction chemotherapy consisting of one or two courses of daunorubicin (60 mg/m2 daily for 3 days) combined with cytarabine (100 mg/m2 daily for 7 days). The patients who achieved complete remission (CR) received at least one course of 5 + 2 consolidation chemotherapy regimen (100 mg/m2 cytarabine daily for 5 days plus 60 mg/m2 daunorubicin daily for 2 days). Eight patients received allogeneic hematopoietic stem cell transplantation (HSCT) in first remission. The patients who received allogeneic HSCT were censored on the day of HSCT. The study was approved by the ethics committee of Tehran University of Medical Sciences and written informed consents were obtained from all the participants. The healthy control group composed of 54 volunteers including 22 men and 32 women with the median age of 40 years (range: 17-74 years).
The mononuclear cells were separated from the BM specimens by Ficoll-Paque density-gradient centrifugation according to the manufacturer's instruction (GE Healthcare). After washes with phosphate-buffered saline (PBS; pH = 7.4, 0.15 M), the AML samples that contained ≥80% blast cells were directly lysed in TriPure isolation reagent.
Cytogenetic analysis and mutation detection
As previously described (Pashaiefar et al., 2018), G-banding and fluorescent in situ hybridization (techniques were done to detect cytogenetic abnormalities of the patients. Chromosomal aberrations were described based on the International System of Human Cytogenetic Nomenclature (ISCN 2013) recommendations (Shaffer et al., 2013) and patients were cytogenetically categorized according to the current National Comprehensive Cancer Network guidelines (O'Donnell et al., 2012).
Mutations in NPM1 (exon 12) and FLT3 (internal tandem duplications) were successfully screened in all the patients by high-resolution melting analysis (HRMA) as previously reported (Tan et al., 2008). Positive specimens were confirmed using capillary electrophoresis-based fragment analysis.
RNA extraction, cDNA synthesis, and quantitative reverse transcription-polymerase chain reaction analysis
TriPure isolation reagent was used for RNA extraction according to the manufacturer's instructions (Roche, Germany). The concentration and purity of the extracted RNA were determined using a NanoDrop spectrophotometer. Reverse transcription of 1000 ng of extracted RNA to complementary DNA (cDNA) was performed with a cDNA synthesis kit (Takara, Japan).
The expression level of PARP-1 was evaluated by SYBR Green-based quantitative reverse transcription-polymerase chain reaction (qRT-PCR) using StepOnePlus Real-Time PCR System (Applied Biosystems) under the following cycling conditions: an initial denaturation at 95°C for 10 min, followed by 40 cycles of 95°C for 30 s and 60°C for 45 s. To check the specificity of primers, melting curve analysis was done at the end of each run. Standard curve was provided using a serial dilution (fivefold dilutions) of cDNA samples to determine the efficiency of PCRs. qRT-PCR was performed in a final volume of 20 μL containing 10 μL qPCR Master Mix (Takara), 2 μL of cDNA samples, 0.5 μL of each forward and reverse primers, and 7 μL ddH2O. To normalize the PARP-1 expression levels, ABL1 was applied as the reference gene (Beillard et al., 2003). The relative quantification of the PARP-1 gene expression was determined by the 2−ΔCt method. The primers were designed using Primer3 software (Untergasser et al., 2012). The primer sequences and characteristics are shown in Table 2.
qRT-PCR, quantitative reverse transcription-polymerase chain reaction.
Statistical analysis
The SPSS 20.0 software package was used for all statistical analysis. The association of categorical variables was examined by Pearson χ2 analysis or Fisher exact test. All the continuous variables were checked for normality with the Kolmogorov-Smirnov test. Mann-Whitney U-test and Kruskal-Wallis test were performed to compare the distribution of non-normally distributed variables between categories.
As previously described (Pashaiefar et al., 2018), the overall survival (OS) was measured from the date of first diagnosis until the date of death of any cause or until the date of last follow-up. Relapse-free survival (RFS) was measured from the date of CR until the date of relapse, death of any cause or last follow-up. Relapse was defined as at least 5% BM blasts or development of extramedullary leukemia. CR was defined based on the European Leukemia Net guidelines (Döhner et al., 2010) and patients who failed to achieve criteria of CR were described as nonresponse. Survival curves for RFS and OS were plotted by using Kaplan-Meier method and compared using the log-rank test. The effect of PARP-1 expression on OS and RFS was further analyzed by a Cox proportional hazards model adjusted to other well-known risk factors. For all the statistical analyses, p-values <0.05 were considered to be statistically significant.
Results
PARP-1 transcript levels were increased in non-M3 AML patients
The levels of PARP-1 mRNA expression were markedly upregulated in patients with non-M3 AML (median 1.74, range: 0.03-6.45), compared with the healthy controls (median 1.05, range 0.054-3.92) (p < 0.001, Fig. 1). Patients with adverse cytogenetic risk have higher expression of PARP-1 than those of intermediate and good cytogenetic risk groups (p = 0.004) (Fig. 1). Moreover, no statistically significant difference in PARP-1 mRNA expression was observed between different subgroups of non-M3 AML patients according to the FAB criteria (p = 0.26).
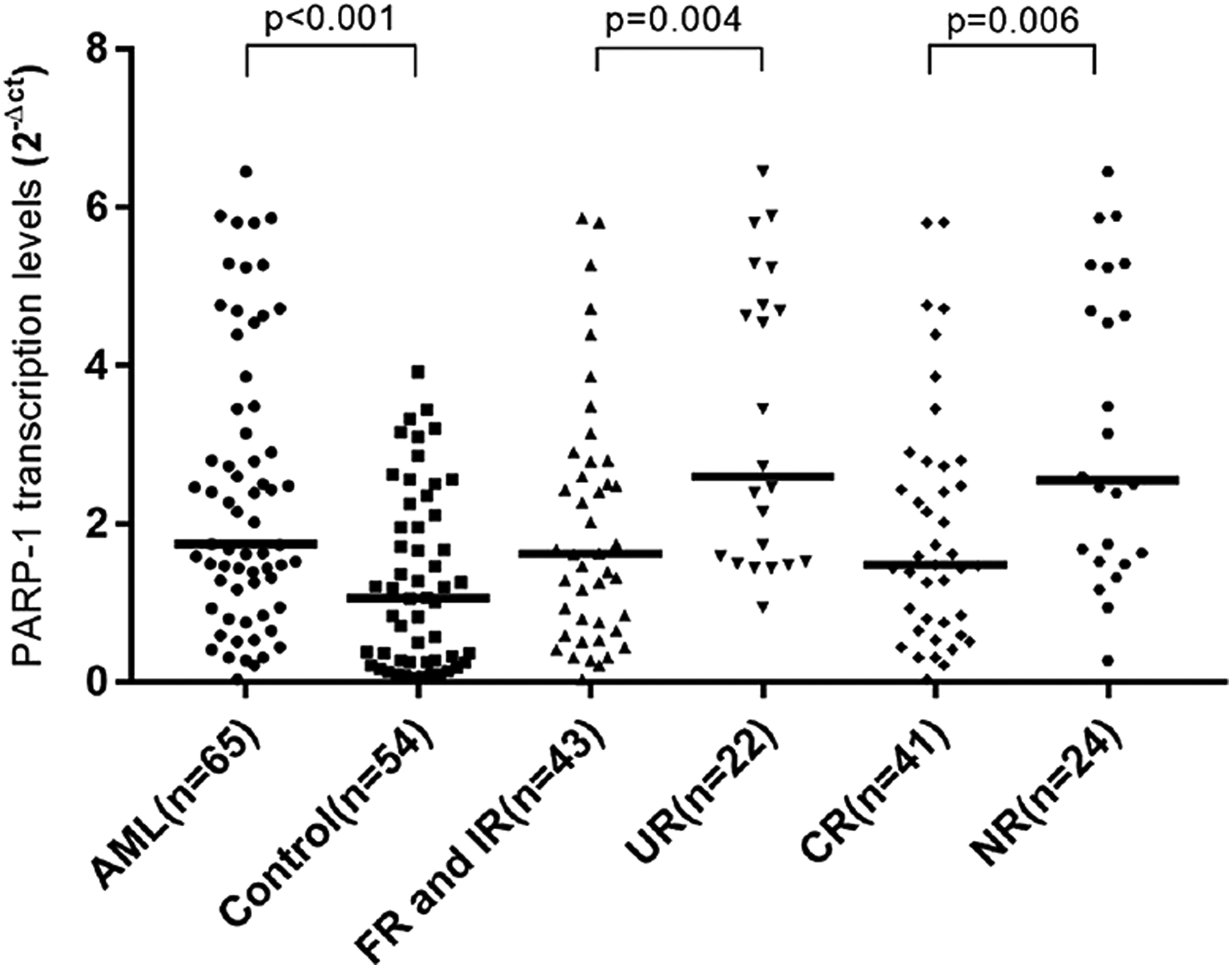
PARP-1 transcription levels in non-M3 AML patients, cytogenetic risk subgroups, and normal control. The line that is marked in each column represents the median. The Mann-Whitney U-test was used for statistical analysis. AML, acute myeloid leukemia; CR, complete remission; FR, favorable risk; IR, intermediate risk; NR, nonresponse; UR, unfavorable risk group.
Correlation of PARP-1 expression with clinical and laboratory features of non-M3 AML patients
According to the median level of PARP-1 mRNA expression (1.74), non-M3 AML patients were classified into two groups: low PARP-1 expression (PARP-1low) group (<1.74) and high PARP-1 expression (PARP-1high) group (≥1.74). We found no statistically significant difference between PARP-1high and PARP-1low patients according to the age, gender, peripheral white blood cells (WBCs) count, hemoglobin, platelet count, percentage of BM blasts as well as in distribution of FAB classification, karyotypic classification, and NPM1 and FLT3 gene mutations (Table 3). However, there was a statistically significant difference between the two groups of patients in the rates of CR after induction therapy (p = 0.04). Besides, patients with refractory response to chemotherapy had higher PARP-1 expression levels before treatment (p = 0.006).
p-values are from Mann-Whitney U-tests or Pearson χ2 tests for continuous and categorical variables, respectively.
Association of PARP-1 expression levels and clinical outcome of non-M3 AML patients
Survival data were obtained for all 65 non-M3 AML patients with the median of 9 months follow-up (range 1-17 months). High PARP-1 expressing patients tended to have shorter OS (median 2.5 months vs. 12.5 months, p = 0.01) and RFS (median 1.5 months vs. 9.46 months, p = 0.005) than low PARP-1 expressing patients (Fig. 2). A multivariable analysis was conducted to identify the prognostic significance of PARP-1 expression levels, in addition to the well-known prognostic factors, including age, WBC, FLT3 and NPM1 gene mutations, and cytogenetic classification. After adjusting for other risk factors, PARP-1 expression remained as a significant prognostic factor for both OS and RFS in non-M3 AML patients (Table 4).
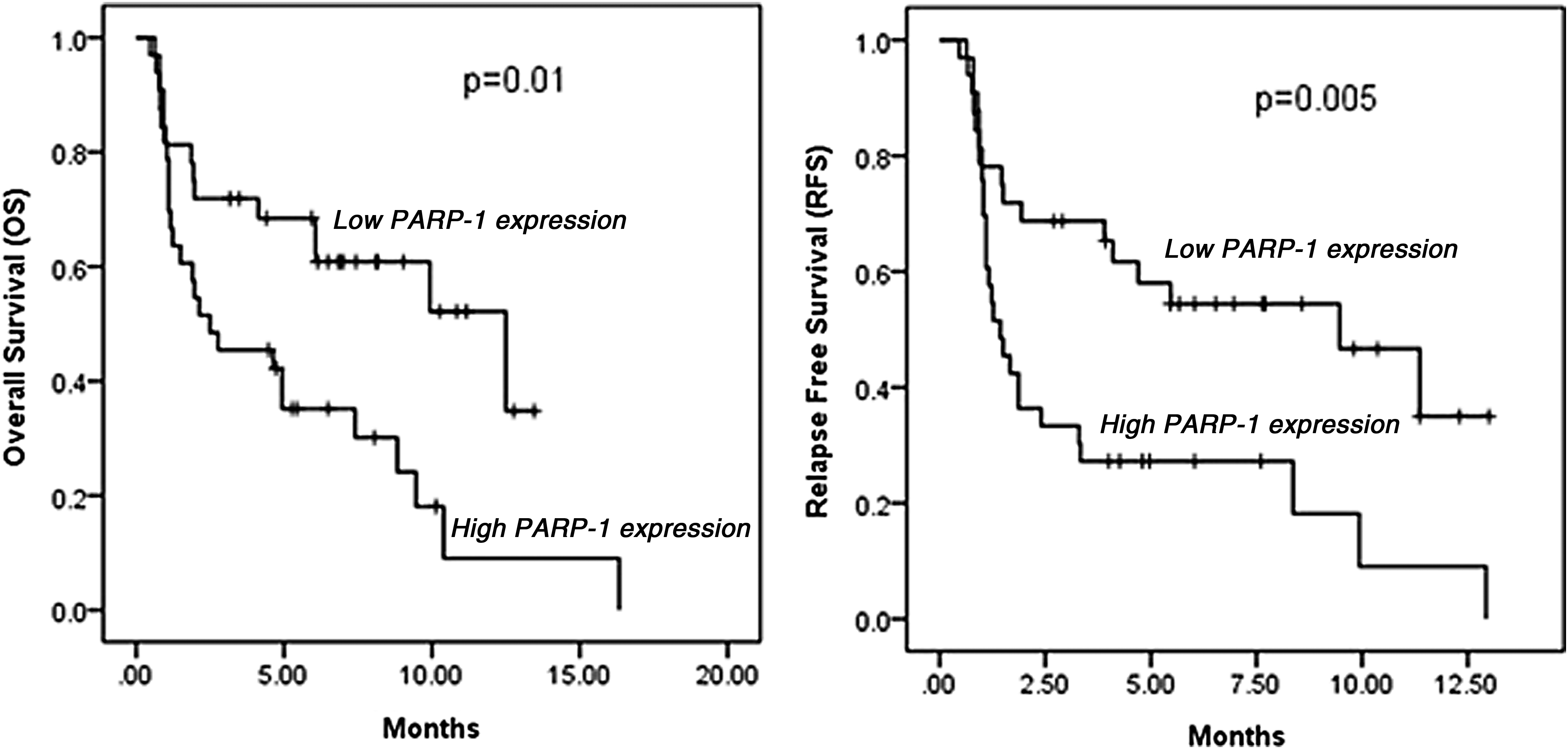
Kaplan-Meier survival curves according to PARP-1 expression levels in non-M3 AML patients.
We did not observe the impact of NPM1 mutation on outcome of patients, which might be due to the small size of patients with NPM1 mutation in our cohort. Only variables with a p-value of 0.2 or less in univariate analysis were included in the multivariate analysis.
CI, confidence interval; HR, hazard ratio; OS, overall survival; RFS, relapse-free survival.
Discussion
In the presence of DNA lesions, PARP-1 acts as a sensor to detect DNA damage, binds to single- and double-strand DNA breaks, and plays an important role in the DNA repair process (Wang et al., 2012). Emerging pieces of evidence show that apart from its important roles in DNA damage repair, PARP-1 has several cancer-related functions, including regulation of transcription, DNA methylation, autophagy, control of cell cycle progression, and cell proliferation (Schreiber et al., 2006; Kraus and Hottiger, 2013; Wang et al., 2015).
It has been recently shown that in vitro inhibition of PARP-1 in AML cell lines decreases cell proliferation and induces apoptosis, suggesting an important function of PARP-1 in the pathogenesis of AML (Wang et al., 2015). However, little is known about expression levels and clinical implication of PARP-1 gene in AML. Therefore, here we investigated the PARP-1 mRNA expression in de novo non-M3 AML patients to evaluate the influence of PARP-1 mRNA expression levels on the clinical features and prognosis of the patients.
We found that PARP-1 was significantly upregulated in non-M3 AML patients compared with the healthy controls. However, no statistically significant difference in PARP-1 mRNA expression was observed in non-M3 AML patients with different FAB subtypes. High expression of PARP-1 was seen in the adverse cytogenetic risk group of non-M3 AML patients compared with intermediate and favorable risk groups, suggesting an important role of PARP-1 in the AML progression.
According to previous studies, induced replication and oxidative stress lead to DNA damage accumulation in AML blasts (Zhou et al., 2013). Therefore, PARP-1 overexpression may be due to DNA damage accumulation in these blasts. Correlation of PARP-1 expression levels with cytogenetic risk groups was previously reported in B cell ALL and myelodysplastic syndrome patients (Pournazari et al., 2014; Diamantopoulos et al., 2017) and emphasizes the important function of PARP-1 in the pathogenesis and progression of human hematologic malignancies.
We found that PARP-1 mRNA expression levels correlated with inferior OS and RFS in univariate analysis. Moreover, multivariate analysis indicated that PARP-1 mRNA expression levels were an independent prognostic factor in de novo non-M3 AML patients. It is not fully elucidated how PARP-1 aggravates AML pathogenesis. Wang et al. (2015) have shown that PARP-1 upregulates the expression of myeloproliferative leukemia virus oncogene through poly ADP-ribosylation, which further activates the PI3K-AKT and MAPK pathways and induces AML cells proliferation and prevents apoptosis (Wang et al., 2015).
PARP-1 is also involved in DNA methylation by regulation of expression levels or protein activity of DNA methyltransferase-1. This involvement is very important, because abnormal patterns of DNA methylation are a characteristic feature of AML cells, and a recent report has suggested that AML patients might benefit from combination of hypomethylating agents and PARP inhibitors (Orta et al., 2014).
It is very important to have a better understanding of the precise mechanisms through which PARP-1 participates in leukemogenesis, to be able to use PARP inhibitors for AML treatment. We have also evaluated the association between response to chemotherapy and initial levels of PARP-1 expression in non-M3 AML patients. Our data indicate that high expression levels of PARP-1 were seen in refractory patients, suggesting that PARP-1 may contribute to treatment failure in this group of the patients. Chemotherapy agents generate more DNA damage in AML cells and probably upregulate PARP-1 gene. The aberrant DNA repairing activity resulted from PARP-1 overexpression in AML cells may enhance the antiapoptotic property of AML blasts, which results in poor response to chemotherapy. This finding suggested that inhibition of PARP-1 might be an effective option to overcome chemoresistance in AML. At least five PARP inhibitors are in different phases of clinical trial for solid tumor (Ohmoto and Yachida, 2017). Moreover, in vitro efficacy of PARP inhibitors has been reported in several lymphoid and myeloid malignancies (Zhao and So, 2016).
Taken together, our findings indicate that upregulation of PARP-1 gene might be used as a poor and independent prognostic factor in non-M3 AML patients. If confirmed by other studies and larger patient series, our findings may have two potential clinical applications. First, the correlation of PARP-1 expression levels with OS and RFS of non-M3 AML patients introduces a new risk factor for non-M3 AML patients that can be used in risk stratification of AML patients. What could be helpful toward this direction is quantifying PARP-1 expression levels in a large cohort of patients that may set a cutoff point. Second, higher expression levels of PARP-1 in refractory AML patients suggest that PARP-1 inhibitors can be used in clinical trials for AML patients.
Our study has the limitation in that we did not investigate the PARP-1 protein or activity levels in our patients. However, a recent study has shown that there is a significant correlation between PARP-1 mRNA and protein as well as PARP activity in AML patients (Faraoni et al., 2015). This correlation suggests that the mRNA levels of PARP-1 may predict the levels of PARP-1 protein and PARP activity in these patients.
Footnotes
Acknowledgment
This research was supported by Hematology/Oncology and Stem Cell Transplantation Research Center, Tehran University of Medical Sciences, Tehran, Iran (grant number: 29237).
Author Disclosure Statement
No competing financial interests exist.