
Abstract
Aims:
We explored the relationship between the mutation at the p.G245S site in TP53 and the short-term recurrence of hepatocellular carcinoma (HCC).
Materials and Methods:
101 HCC patients were included in this study. The TP53 p.G245S mutation frequency spectrum was examined by direct sequencing of genomic DNA from tissue specimens of HCC patients. Univariate and multivariate Cox regression analyses were performed to evaluate the independent prognostic factors of tumor recurrence. ROC curve analysis was applied to determine the cut-off value for the p.G245S mutation frequency and to verify the predictive ability of the Cox model compared with single risk factor indices.
Results:
A multivariate Cox regression analysis showed that TP53 p.G245S mutation frequency (HR = 1.231, 95% CI: 1.006-1.505, p = 0.043), AFP (HR = 2.432, 95% CI: 1.297-4.561, p = 0.006), MTM (HR = 2.656, 95% CI: 0.930-7.583, p = 0.068), and PVTT (HR = 14.297, 95% CI: 3.085-66.243, p = 0.001) were independent prognostic factors for short-term recurrence. The cut-off value for the TP53 p.G245S mutation frequency (18.5%) was determined by ROC analysis. A predictive model integrating the TP53 p.G245S mutation frequency with PVTT, MTM, and AFP values appears to an excellent predictive indicator of short-term recurrence in HCC patients (AUC = 0.849, 95% CI = 0.748-0.950, p = 0.000001). Survival analysis indicated that the probability of short-term recurrence-free survival was significantly different among different TP53 p.G245S mutation frequency, MTM, PVTT, and AFP risk groups (p < 0.05).
Conclusion:
The mutation frequency of the p.G245S site is a novel prognostic risk factor for the short-term recurrence of HCC.
Introduction
Hepatocellular carcinoma (HCC)
Many HCC patients experience intrahepatic or distant organ metastasis during the course of treatment or shortly after hepatectomy. For resectable patients, the 5-year recurrence rate can be as high as 70% (Forner et al, 2018). Equally as difficult and challenging as the early diagnosis of HCC is the early detection of HCC recurrence. HCC recurrence after surgery is divided into short-term recurrence within 1 year and long-term recurrence over 1 year (Jung et al, 2019). Unlike long-term recurrence, which is considered a new-onset tumor, short-term recurrence is mainly related to the high invasiveness of the primary tumor, such as microvascular invasion (MVI) and intrahepatic metastasis (Hirokawa et al, 2016; Hu et al, 2014; Jung et al, 2019).
The existing studies on the risk factors for the short-term recurrence of HCC mainly focused on the clinical characteristics of patients, including preoperative hepatitis B virus (HBV) DNA level, preoperative serum alpha-fetoprotein (AFP) level, tumor size, tumor number, MVI, and so on (Hirokawa et al, 2016; Hu et al, 2014; Jung et al, 2019; Sohn et al, 2014). There is no effective prediction model for short-term HCC recurrence to help clinicians choose individualized treatment regimens, optimize treatment modes, and improve patient prognosis.
TP53 is a tumor suppressor gene with the highest correlation with human tumors. More than 50% of malignant tumors have TP53 mutations (Mirgayazova et al, 2020; Monti et al, 2020). TP53 mutations are closely related to the occurrence and development and even the histological type of HCC. Most HCC patients with TP53 mutation have MVI and local sarcomatoid changes, accompanied by HBV infection and elevated serum AFP levels, which leads to a poor prognosis (Calderaro et al, 2017).
A new histological subtype, macrotrabecular-massive (MTM), which is closely related to clinicopathological features and prognosis of HCC, was reported in 2017 (Calderaro et al, 2017; Torbenson et al, 2019). TP53 mutations were reported to have a significant correlation with the MTM histological subtype of HCC (Calderaro et al, 2017). c.733G>A (p.Gly245Ser) is reported as a TP53 gene “hotspot” mutation in ovarian cancer that involves changes in multiple target sites on the exon of TP53 (Deniger et al, 2018). However, no study has shown its association with the short-term recurrence of HCC.
The study aimed to explore the relationship between the TP53 p.G245S mutation frequency and the short-term recurrence of HCC and further clarify the utility of gene mutation information coupled with histological type and clinical characteristics in the prediction of short-term recurrence to finally establish an effective short-term recurrence prediction model.
Materials and Methods
Patients
A total of 101 patients histologically diagnosed with HCC between April 2020 and February 2021 at Ningbo Medical Center Lihuili Hospital were included in the study. The inclusion criteria were as follows: (1) pathologically diagnosed HCC; and (2) not receiving any radiotherapy, chemotherapy, or immunotherapy before surgery. The exclusion criteria were as follows: (1) pregnant and lactating women; (2) patients with a history of other cancers; and (3) patients with incomplete clinical or follow-up data. The patients were divided into a short-term recurrence group (recurrence within 1 year) and a non-short-term recurrence group. The study was approved by the Ethics Committee of Ningbo Medical Center Lihuili Hospital (Project Identification Code: KY2020PJ125), and all methods were performed in accordance with the relevant guidelines and regulations. Informed consent was obtained from all patients before the study.
Clinical characteristics and follow-up
Clinical characteristics, including HBV, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), γ-glutamyl transpeptidase (GGT), prothrombin time (PT), thrombin time (TT), albumin (Alb), total bilirubin (TB), direct bilirubin (DB), international normalized ratio (INR), AFP, AFP-L3, carbohydrate antigen 19-9 (CA19-9), cirrhosis, tumor number, tumor size, differentiation, MTM, MVI, portal vein tumor thrombus (PVTT), and clinical stage, were collected for all patients. All the obtained surgical specimens were histologically assessed by different pathologists.
Pathological examination results included pathological differentiation, MVI, tumor diameter, number of tumors, cirrhosis, tumor capsule, and PVTT. Measurements of AFP value was performed with a microchip capillary electrophoresis and liquid-phase binding assay on the μ TASWakoi30 auto-analyzer (Wako Pure Chemical Industries, Ltd., Osaka, Japan). Baseline data were collected from our hospital clinical database. Patients were consistently followed up after HCC resection at intervals of 3 months. Patient follow-up was aimed at determining recurrence-free survival.
Origin of specimens
A total of 101 surgical specimens of HCC were collected from the Ningbo Medical Center Lihuili Hospital, which were confirmed by pathological diagnosis and stored in liquid nitrogen until DNA was extracted.
Genomic DNA isolation
Genomic DNA (gDNA) was isolated from tumor tissues using the QIAamp DNA Mini Kit (Qiagen). The concentration of the purified gDNA was determined by an Infinite M200 PRO reader (Tecan).
PCR amplification
PCR amplification was performed in an ABI 9700 PCR System (Applied Biosystems, Inc.). The PCR protocol was as follows: initial denaturation at 95°C for 3 min, followed by 40 cycles at 94°C for 30 s, 56°C for 30 s, and 72°C for 1 min, ending at 72°C for 7 min. The primers were designed using PyroMark Assay Design 2.0. The primer sequences were as follows: 5′-ATCTCCTAGGTTGGCTCTGACTG-3′ for TP53:733-F, 5′-GGCTCCTGACCTGGAGTCTT-3′ for TP53:733-F (5′-Biotin), and 5′-AACAGTTCCTGCATGG-3′ for TP53:733-S.
Pyrosequencing and data analysis
Pyrosequencing of PCR amplification products was carried out using PyroMark Q96 (Qiagen, Germany) and its companion (Pyro Q-AQ) software used to automatically analyze the proportion of single nucleotide polymorphisms in selected gene loci.
Mutation site selection
TP53 gene exon mutation sites were obtained from the Stanford Molecular Pathology Laboratory gene analysis platform “cancer somatic mutation panel (CSMP)” (Yousef and Jothy, 2014). The pretest detected seven sites (c.524G>A p.Arg175His, c.524G>T p.Arg175Leu, c.733G>A p.Gly245Ser, c.733G>C p.Gly245Arg, c.733G>T p.Gly245Cys, c.742C>G p.Arg248Gly, c.742C>T p.Arg248Trp, c.743G>A p.Arg248Gln, c.743G>C p.Arg248Pro, c.743G>T p.Arg248Leu, c.817C>A p.Arg273Ser, c.817C>G p.Arg273Gly, c.817C>T p.Arg273Cys, c.818G>A p.Arg273His, c.818G>C p.Arg273Pro, c.818G>T p.Arg273Leu, c.916C>T p.R273X) on exon 7/8 of TP53. All of the confirmed TP53 mutation sites were determined by pyrophosphate sequencing, and c.733G>A p.Gly245Ser was selected according to the most significant difference between the short-term recurrence group and the non-short-term recurrence group. In this study, we detected the mutation frequency of this site in the expanded sample.
Establishment of the Cox prediction model
A Cox proportional hazards model was used for independent risk factor analysis and modeling. According to the results of the regression analysis, a Cox prediction model was constructed to predict the probability of early recurrence. Receiver operating characteristic (ROC) curve analysis was performed for the simplified differential diagnosis to verify the predictive ability of the Cox model compared with other risk factor indices.
Statistical analysis
Statistical analysis of the numerical variables was performed using unpaired Student's t-test for parametric data. Categorical variables were compared using Pearson's chi-square test or Fisher's exact test. Survival curves were calculated using the Kaplan-Meier method and compared using the log-rank test. Univariate and multivariate Cox proportional hazards regression models were used to evaluate the independent prognostic factors of OS and tumor recurrence. Univariate analysis was carried out to investigate potential prognostic factors, then the factors with a p-value <0.05 in the univariate analysis were entered into stepwise variable selection method multivariate analysis using multivariate Cox model to identify independent risk factors, respectively.
The establishment of Cox model was based on the results of independent risk factors derived from multivariate analysis. ROC curve analysis was applied to determine the cutoff value of TP53 and verify the predictive ability of the Cox model compared with other risk factor indices. All statistical analyses were performed using SPSS 25.0 (IBM Corporation, 2020). p < 0.05 was considered statistically significant.
Results
Patient characteristics
The baseline characteristics of the included patients are presented in Table 1. Univariate analysis showed that TP53 p.G245S mutation frequency (t = 2.44, p = 0.016), AFP (χ2 = 8.52, p = 0.014), MTM (χ2 = 15.883, p < 0.001), MVI presence (χ2 = 6.449, p = 0.011), tumor number (χ2 = 6.209, p = 0.013), tumor size (t = 2.115, p = 0.037), PVTT (χ2 = 6.604, p = 0.01), T stage (χ2 = 18.907, p < 0.001), and CNLC grade (χ2 = 14.32, p < 0.001) were significantly different between the short-term and non-short-term recurrence groups (p < 0.05, Table 1).
The Baseline Characteristics of Short-Term Recurrence Patients and Non Short-Term Recurrence Patients
AFP, alpha-fetoprotein; Alb, albumin; ALT, alanine aminotransferase; ALP, alkaline phosphatase; AST, aspartate aminotransferase; CA19-9, carbohydrate antigen 19-9; DB, direct bilirubin; GGT, γ-glutamyl transpeptidase; HBV, hepatitis B virus; INR, international normalized ratio; MTM, macrotrabecular-massive; MVI, microvascular invasion; PT, prothrombin time; PVTT, portal vein tumor thrombus; TB, total bilirubin; TT, thrombin time.
Cox regression analysis
Univariate Cox regression showed that TP53 p.G245S mutation frequency (hazard ratio [HR] = 1.266, 95% CI: 1.035-1.548, p = 0.022), AFP (HR = 1.846, 95% CI: 1.075-3.170, p = 0.026), MTM (HR = 4.560, 95% CI: 1.892-10.989, p = 0.001), MVI presence (HR = 2.601, 95% CI: 1.058-6.395, p = 0.037), tumor number (HR = 3.227, 95% CI: 1.334-7.806, p = 0.009), tumor size (HR = 1.218, 95% CI: 1.060-1.401, p = 0.006), and PVTT (HR = 7.492, 95% CI: 2.418-23.207, p < 0.001) were prognostic factors for short-term recurrence (Table 2).
Univariate Cox Regression Analyses of Short-Term Recurrence in Hepatocellular Carcinoma Patients
HR, hazard ratio; SE, standard error.
Upon multivariate Cox regression analysis, TP53 p.G245S mutation frequency (HR = 1.231, 95% CI: 1.006-1.505, p = 0.043), AFP (HR = 2.432, 95% CI: 1.297-4.561, p = 0.006), MTM (HR = 2.656, 95% CI: 0.930-7.583, p = 0.068), and PVTT (HR = 14.297, 95% CI: 3.085-66.243, p = 0.001) were determined to be independent prognostic factors for short-term recurrence (Table 3).
Multivariate Cox Regression Analyses of Short-Term Recurrence in Hepatocellular Carcinoma Patients
AFP, MTM, PVTT, and TP53 p.G245S mutation were included in the multivariable model.
ROC curve analysis
The 18.5% cutoff value of TP53 p.G245S mutation frequency was determined by ROC curve analysis and had a sensitivity of 0.700 and a specificity of 0.630 (Fig. 1). Subsequently, the patients were divided into a low-risk group and a high-risk group of short-term recurrence based on the cutoff value. There was no statistical difference in MTM (p = 0.068), but MTM was still included in the multivariate Cox regression model. We hypothesized that this might be related to the strong association among AFP, MTM, and PVTT (Calderaro et al, 2017; Shan et al, 2022). And it was found that a good AUC could be obtained when MTM was included in the model, which was better than that of a single variable.
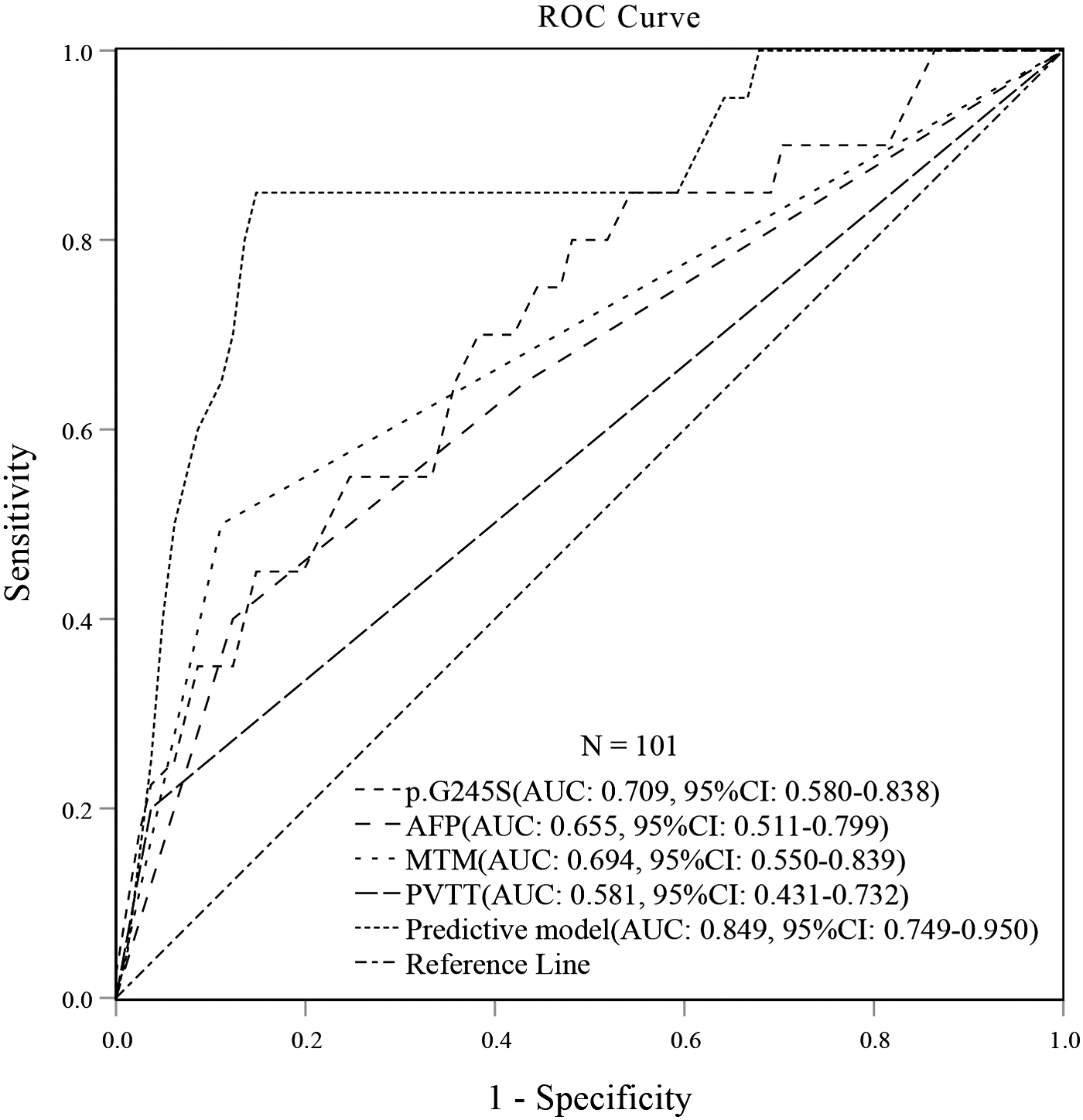
ROC curve analysis of the association between TP53 p.245S mutation, AFP, MTM, PVTT, and HCC short-term recurrence. AFP, alpha-fetoprotein; HCC, hepatocellular carcinoma; MTM, macrotrabecular-massive; PVTT, portal vein tumor thrombus; ROC, receiver operating characteristic.
Consequently, TP53 p.G245S mutation, AFP, MTM, and PVTT were finally included in the Cox model. The cutoff value of the prediction model (0.285*TP53 p.245S mutation +2.409*PVTT +0.750*MTM +0.609*AFP) was 6.89, with a sensitivity of 0.850 and a specificity of 0.840. The prediction model integrating TP53 p.G245S mutation frequency, PVTT, MTM, and AFP could be a predictive indicator of short-term recurrence in HCC patients (area under the curve [AUC] = 0.849, 95% CI: 0.748-0.950, p < 0.001). The concordance index (C-index) is calculated to measure discrimination with 1000 bootstrapping techniques and the prediction Cox model has good prediction accuracy (C-index: 0.751, 95%CI: 0.624-0.878).
Prognostic outcomes
The cutoff value of TP53 p.G245S mutation frequency (18.5%) and AFP (<20, 20-250, and >250) were determined by our preanalysis and ROC curve analysis. The cutoff value of MTM (positive and negative) and PVTT (positive and negative) were determined according to pathological results.
The overall 1-year recurrence rate for patients was 19.8%. The short-term recurrence rate for patients with a low risk of TP53 p.G245S mutation frequency was 16.5%, whereas for those with a high risk it was 54.6% (p = 0.011). The short-term recurrence rate in patients without MTM was 29.3% compared with 63.5% in patients with MTM (p = 0.00016). Patients with PVTT had a short-term recurrence rate of 78.6% compared with 33.1% in patients without PVTT (p < 0.0001). For AFP <20, 20-250, and >250, the short-term recurrence rates were 23.1%, 47.1%, and 46.5%, respectively (p < 0.0001). There were significant differences in short-term recurrence among the different TP53 p.G245S mutation frequency risk groups, MTM groups, PVTT groups, and AFP level groups (p < 0.05), as shown in Figure 2A-D.
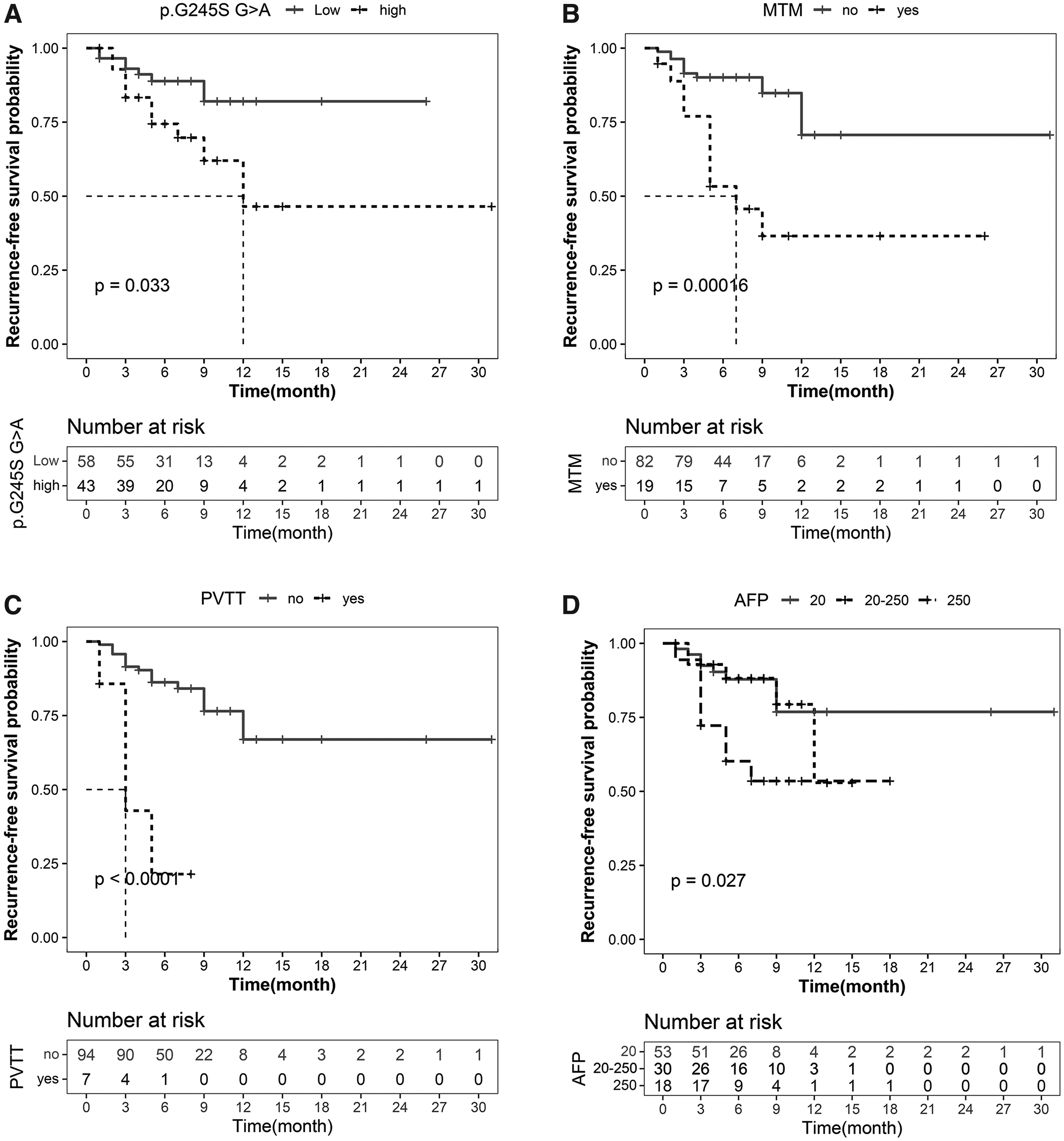
The short-term recurrence-free survival probability.
Discussion
The prediction of HCC recurrence, especially short-term recurrence, is a challenge for surgeons. At present, there is no conclusive consensus regarding the short-term recurrence of HCC and its risk factors. For the identification of the short-term recurrence of HCC, some centers define recurrence within 6 months after surgery as short-term recurrence, whereas some centers still use 2 years as the standard (Hirokawa et al, 2016; Imamura et al, 2003; Lee et al, 2019; Shimoda et al, 2016; Sohn et al, 2014; Zhou et al, 2015). According to our experience at our center, recurrence 1 year after surgery was considered short-term recurrence in this article. Among the 101 HCC patients enrolled in this study, the incidence of early recurrence was 19.8%.
Previous studies on risk factors for short-term recurrence of HCC mainly focused on the clinical characteristics of patients, including HBV DNA level, AFP level, tumor size, tumor number, MVI, and PVTT (Hirokawa et al, 2016; Hu et al, 2014; Jung et al, 2019; Sohn et al, 2014). Most of the studies explored the relationship between single characteristics and the short-term recurrence of HCC and lacked assessments of the correlations between HCC gene mutation and histological type and short-term recurrence. In contrast, our study first revealed that the TP53 p.G245S mutation frequency is strongly associated with short-term recurrence in HCC patients, and based on this, combined with MTM, PVTT, and AFP, an effective short-term recurrence prediction model was established.
TP53 is a tumor suppressor gene whose mutation occurs in >50% of malignant tumors (Mirgayazova et al, 2020; Monti et al, 2020). TP53 mutation is closely associated with the occurrence, development, and even the clinical manifestations of HCC. Studies have shown that TP53 mutations in HCC are mostly related to the frequent activation of RAS-MAPK, MET, PI3K/AKT, and other signaling pathways (Rebouissou and Nault, 2020). The activation of the aforementioned pathways induces the phosphorylation of dynamin-related protein 1 (DRP1), accelerates mitochondrial division, and promotes the proliferation of tumor cells (Dimri and Satyanarayana, 2020; Fonseca et al, 2019; Kashatus et al, 2015; Serasinghe et al, 2015); furthermore, overexpression of epidermal growth factor receptor, vascular endothelial growth factor, and matrix metalloproteinases was induced to promote tumor invasion and metastasis (Dimri and Satyanarayana, 2020).
Therefore, HCC with this mutation manifests high invasiveness, low differentiation, MVI, HBV infection, elevated AFP, and local sarcomatoid changes, resulting in the poor prognosis of patients (Calderaro et al, 2017; Cancer Genome Atlas Research Network, 2017; Hosny et al, 2008; Rebouissou and Nault, 2020). It has further been shown that the R249S mutation of TP53 is by far the most frequent mutation in HCC (Hosny et al, 2008; Nogueira et al, 2009; Pandima Devi et al, 2010; Shen et al, 2020). R249S might promote carcinogenesis in the liver but not in other tissues, and the R249S mutation could be detected in the plasma DNA of 38% of HCC patients (Szymańska et al, 2004; Szymańska and Hainaut, 2003). In this article, we found a new mutation site of TP53, p.G245S, whose mutation frequency was significantly different between the short-term recurrence and non-short-term recurrence groups. Patients with a high risk of TP53 p.G245S mutation frequently presented with short-term recurrence.
In recent years, along with the further understanding of the tissue biological characteristics of HCC, an increasing number of researchers have shifted their attention to the tissue type of HCC. French pathologists reported (Calderaro et al, 2017) a histological subtype of HCC, MTM, which is closely related to clinicopathological features and prognosis, and preliminarily analyzed its molecular expression and biological characteristics in 2017. HCC with MTM always showed vascular invasion (including large vessels and microvessels), poor differentiation, high proliferation, and cell pleomorphism. Its genotypes were TP53 mutation, FGF19 amplification, and activation of the angiogenesis pathway. Based on the aforementioned findings, researchers speculate that MTM is a subtype with strong invasion and poor prognosis (Calderaro et al, 2017). In our research, the MTM histological type was proven to be an important indicator of short-term recurrence. We found that the short-term recurrence rate of patients who had MTM was as high as 63.5%.
Extensive research has shown that AFP is the most commonly used and important index to diagnose HCC and monitor therapeutic effects. Patients with high preoperative AFP levels have a higher recurrence rate and poor prognosis (Shimoda et al, 2016). In addition, tumor size, tumor number, MVI, and PVTT were associated with short-term recurrence (Hirokawa et al, 2016; Hu et al, 2014; Jung et al, 2019). Our results are consistent with these findings.
On the basis of these results, we studied the correlation between short-term HCC recurrence and gene mutation, histological type, PVTT, and AFP. We subsequently established an effective short-term recurrence prediction model. Nevertheless, our study had the following limitations. First, the TP53 gene mutations were not detected in peripheral blood. Second, no experiments were done to explore if TP53 p.G245S mutation make a difference on the p53's protein functions when compared with the wild type p53. Third, although we found a correlation between the TP53 p.G245S mutation frequency and short-term recurrence, combined with MTM, PVTT, and AFP, the in-depth mechanism of TP53 mutation was not explored. This will be the major research interest of our future study.
Conclusion
The mutation frequency of the TP53 p.G245S site was a novel prognostic risk factor for the short-term recurrence of HCC, and an effective short-term recurrence prediction model based on the TP53 p.G245S site combined with MTM, PVTT, and AFP was developed for HCC patients.
Footnotes
Acknowledgments
The authors thank the patients with hepatocellular carcinoma who participated in this research for their clinical tissue samples.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
Our research was funded by the Ningbo Medical and Health Brand Discipline (PPXK2018-03) and the Science and Technology Program of Zhejiang Health (2021KY1035).