
Abstract
Abstract
Introduction
U
Pregnancy in the semiuterus is also associated with complications, such as abortions, preterm labor, malpresentations, and increased incidence of cesarean sections.
This retrospective study was conducted to analyze the obstetrical and gynecologic implications of unicornuate uterus and rudimentary horn. Strategies for managing these cases are also offered.
Materials and Methods
This study was conducted in a tertiary-care teaching hospital, the Postgraduate Institute of Medical Sciences in Rohtak, Haryana, India. Thirty eight cases, which were diagnosed as unicornuate uterus with a noncommunicating rudimentary horn at laparotomy (April 2007 to March 2012), were retrospectively analyzed. These cases were divided into three groups. Group 1 (n=4) consisted of patients who presented with gynecologic complaints and in whom the condition was diagnosed at laparotomy. Group 2 (n=18) consisted of patients with pregnancy in the rudimentary horn. Group 3 (n=16) consisted of patients who had pregnancy in the semiuterus; most of them underwent cesarean section, during which this malformation was diagnosed. Age, presenting complaints, previous reproductive history, diagnostic investigations, preoperative diagnoses, and intraoperative findings were studied.
Results
Group 1 had 4 cases of adolescents who presented with gynecologic complaints (Table 1). Their mean age was 15.5 years (range, 14–18 years), and all presented with dysmenorrhea and had hematometra in the noncommunicating rudimentary horn on laparotomy. None had any evidence of endometriosis. In only 1 case, diagnosis of a bicornuate uterus was made by USG prior to laparotomy. The remaining 3 cases were diagnosed as rudimentary horn on magnetic resonance imaging (Fig. 1). Rudimentary horn excision and salpingectomy was performed in all 4 cases.
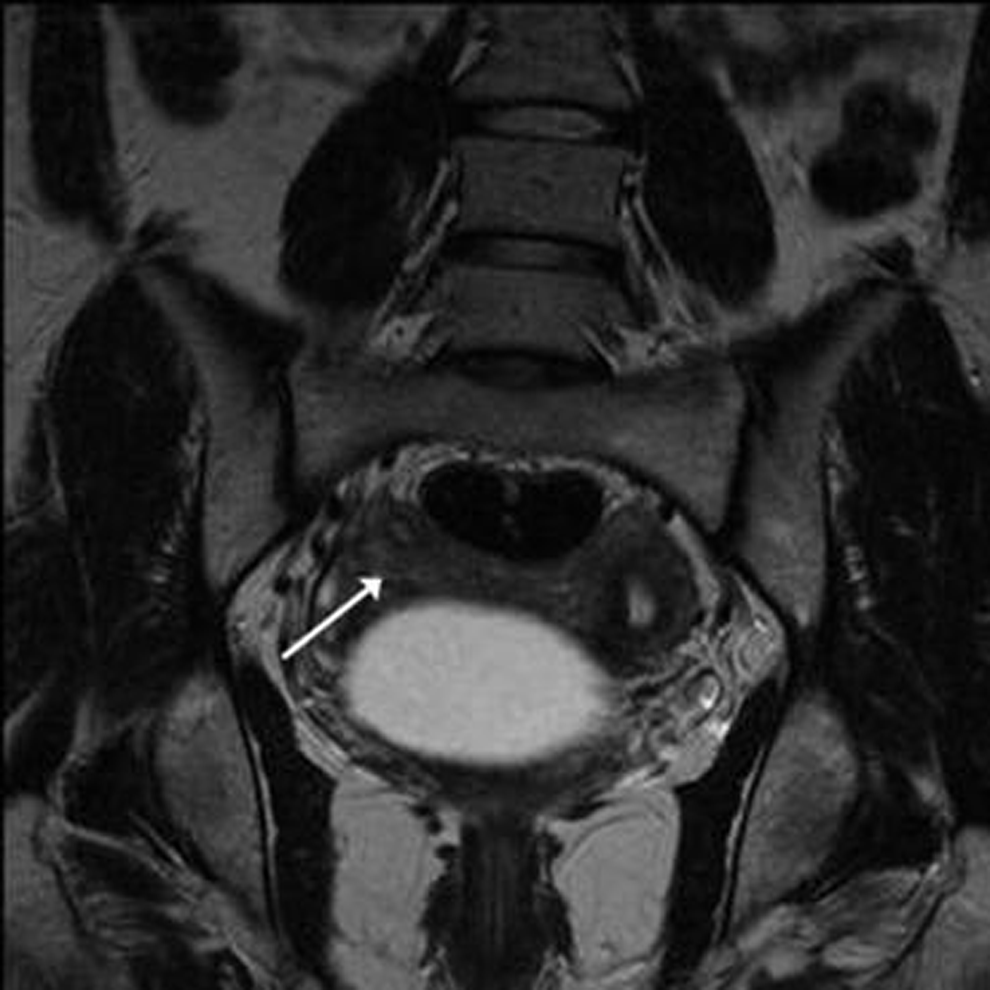
Magnetic resonance imaging showing rudimentary horn in an adolescent (arrow).
Group 2 had 18 cases of rudimentary horn pregnancies (Table 2), with a mean age of 24.8 years (range, 20–30 years), and 94.4% of these patients presented in the second trimester, and 5.5% presented in the first trimester. The most common presenting complaint was pain in the abdomen in 55.5% of the cases, followed by loss of fetal movements in 27.7% of the cases, and failure of induction in 16.6% of the cases. All of these patients underwent laparotomy for the following reasons: 12 patients for hemoperitonium, 5 for failed induction, and 1 for an abdominal pregnancy secondary to rudimentary-horn pregnancy rupture. In 72.22% of the cases, rudimentary horn was found to be ruptured, and in 27.78% of the cases it was intact. Preoperative diagnosis was possible in 13 patients (72.22%); in the remaining 5 patients (27.78%) the condition not expected. Blood transfusion was required in 66.67% of the patients, in the range of 2–6 units (mean, 2.3 units). In all of the patients, removal of the rudimentary horn along with ipsilateral salpingectomy was performed (Fig. 2).

Laparotomy findings suggestive of unruptured rudimentary horn pregnancy.
Group 3 had 16 cases of pregnancies in the semiuterus, where diagnosis of rudimentary horn was made incidentally at the time of cesarean section/laparotomy (Table 3). The mean age of these patients was 24 years (range, 19–30 years), and 50% of the cases were para 1, 43.75% of the cases were para 0, and 6.25% of the cases were para 2. In 93.75% of these cases, diagnosis was made incidentally during cesarean section and, in 1 case, during laparotomy for a ruptured tubal ectopic pregnancy. The most common indication for cesarean section was breech presentation in 73.33% of the cases, followed by fetal distress in 6.67% of the cases, cord prolapse in 6.67% of the cases, oblique positioning in 6.67% of the cases, and antepartum eclampsia in another 6.67% of the cases cases. The gestational age at the time of cesarean was >37 weeks in 81.25% of the patients and 36 weeks in 12.5% of the patients. In 1 patient (6.25%), laparotomy for a ruptured tubal ectopic pregnancy at 7 weeks; during the procedure, diagnosis of unicornuate uterus with a rudimentary horn was made incidentally. A ruptured tubal ectopic pregnancy was found in the Fallopian tube attached to the rudimentary horn. Removal of the rudimentary horn with ipsilateral salpingectomy was performed in all 16 patients.
A renal scan was performed for all of the 4 cases in group 1, of which 2 had renal agenesis and other 2 had normal kidneys. In group 2, only 6 cases of 18 cases had renal scans. Three had renal agenesis, followed by 1 with a pelvic kidney, and the remaining 2 had normal scan results. In group 3, only 4 cases of 16 had renal scans and all these results were normal.
Discussion
Müllerian-duct anomalies are congenital anomalies of the female genital tract resulting from nondevelopment or nonfusion of the Müllerian ducts, or failed resorption of the uterine septum. Unicornute uterus is a type 2 classification (American Society of Reproductive Medicine, 1988) 3 with unilateral hypoplasia or agenesis that can be subclassified further into communicating rudimentary horn, noncommunicating rudimentary horn, or rudimentary horn with no cavity or no horn. The incidence of Müllerian anomalies in the fertile population is 3.2%. Unicornuate uterus accounts for 2.4%–13% of all Müllerian anomalies. 4 Unicornute uterus commonly has a rudimentary horn and, in 72%–85% of cases, it is a noncommunicating type. 5 The connection between the horn and the uterus may be a fibrous or a fibromuscular band. Because of the functioning endometrium, hematometra develops in a noncommunicating rudimentary horn, leading to spasmodic dysmenorrhea and sometimes endometriosis in an adolescent. In some studies, the incidence was as high as 20% but none of the 4 cases in group 1 of the current study had any evidence of endometriosis.
Pregnancies occurring in the noncommunicating rudimentary horn are thought to result from transpertioneal migration of spermatozoa or fertilized ova. This suggestion is based on the finding of corpus luteum of the contralateral ovary in 10% of cases.1,6 Abdominal pain is the commonest symptom associated with rudimentary horn. This pain usually commences from the end of the first trimester and the beginning of the second trimester. Vaginal bleeding is rare, but when it occurs, it is more likely to be associated with pregnancy in a communicating horn. The usual outcome of rudimentary-horn pregnancy is rupture in the second trimester in 90% of cases, with fetal demise; however cases of pregnancy progressing to the third trimester and resulting in a live birth after cesarean section have been documented.7,8 Twelve (66.66%) of the cases in the current study also presented in shock. In some cases, loss of fetal movements caused by intrauterine death and failure of induction subsequently can also be reason enough to suspect the presence of a rudimentary-horn pregnancy, as was seen in 5 of the cases in group 2. Missed abortion and intrauterine death occurs because of a decreased blood supply and defective endometrium.
As rupture of the rudimentary horn can be life-threatening, early diagnosis can be life-saving. Although the literature shows very low preclinical (8%) and preoperative detection rates (29%), a simple pelvic examination in the first trimester or in the early part of the second trimester in every patient complaining of pelvic pain can be, at times, very helpful. Bimanual palpation of a mass extending outside the uterine angle. Baart's de la Faille's sign; displacement of the fundus to the contralateral side with rotation of the uterus and elevation of the affected horn (Ruge Simone syndrome); and deviation of uterus to one side with an adnexal mass in pregnancy may indicate the presence of rudimentary horn. 9 When performing hysterosalpingography (HSG), visualizing a uterus deviated to one side with a unilateral tubal block can also arouse suspicion of the presence of a rudimentary horn. 10 The sensitivity of USG is only 26%, and this decreases with advancing pregnancy age. Tsafrir et al. suggested the following criteria for sonographic diagnosis of rudimentary horn pregnancy: (1) a pseudo pattern of an asymmetrical bicornuate uterus: (2) absent visual continuity in tissue surrounding the gestation sac and uterine cervix; and (3) the presence of myometrial tissue surrounding the gestation sac. 11 In addition, MRI can be used to confirm the diagnosis before an invasive procedure is undertaken. Once diagnosis is strongly suspected, laparoscopy or laparotomy is necessary, and the rudimentary horn should be excised along with the Fallopian tube to prevent future ectopic pregnancy in that tube. In the current study, preoperative diagnosis was strongly suspected in all 12 cases of hemoperitoneum and in only 1 case of failed induction on sonography.
Whenever a surgeon encounters a rudimentary horn during a cesarean section, that horn should always be excised, whether it is communicating or noncommunicating, to avoid the future risk of rudimentary-horn pregnancy. A pregnancy located in the semiuterus of the anomaly is also associated with a high incidence of abortions, preterm labor, cervical incompetence, malpresentation, and cesarean-section rates. In group 3 of the current study, of 16 patients, 1 patient had 7 abortions previously, 3 patients had histories of preterm labor, and 2 patients had histories of premature rupture of the membranes in previous pregnancies.
Evaluation of the renal system should be done in all cases when any kind of uterine anomaly is noted because of high incidence of association between the rudimentary horn or uterine and renal anomalies. In the current study, only 14 of 38 cases had renal scanning; 5 cases had renal agenesis and 1 case had a pelvic kidney; the remaining 8 cases had normal scan results.
Conclusions
Rudimentary horn is a rare anomaly but can have grave consequences if a gravid horn ruptures. Applying a high index of suspicion during evaluation of every patient of early pregnancy with pelvic pain, and using simple bimanual examination and USG can be of great help. Prophylactic resection of the horn along with its Fallopian tube should always be considered, if rudimentary horn is detected incidentally during a cesarean section or during evaluation for infertility.
Footnotes
Disclosure Statement
No competing financial conflicts exist.