
Abstract
Abstract
Introduction
R
Case
A 33-year-old woman, gravida 1, para 0, underwent suction D&C for a hydatidiform mole. The histopathology report showed a complete hydatidiform mole. The patient remained asymptomatic after molar evacuation. Routine serial quantitative testing for serum beta–human chorionic gonadotropin (β-hCG) was performed. The patient's β-hCG levels remained persistently elevated after the suction curettage. Her β-hCG testing performed 1 week after suction curettage was 1974 mIU/mL. Repeat β-hCG testing after the second and third week were 1636 mIU/mL and 5592 mIU/mL, respectively. The rise in β-hCG on the third week post suction curettage prompted another serum evaluation showing 5789 mIU/mL of β-hCG. A metastatic workup and a chest X-ray did not show any contributing reasons for this patient's raised β-hCG level. A repeat ultrasound was performed. The ultrasound scan showed an irregular heterogenous mass occupying the endometrial cavity with dense vascularity, with no myometrial invasion noted (Fig. 1).
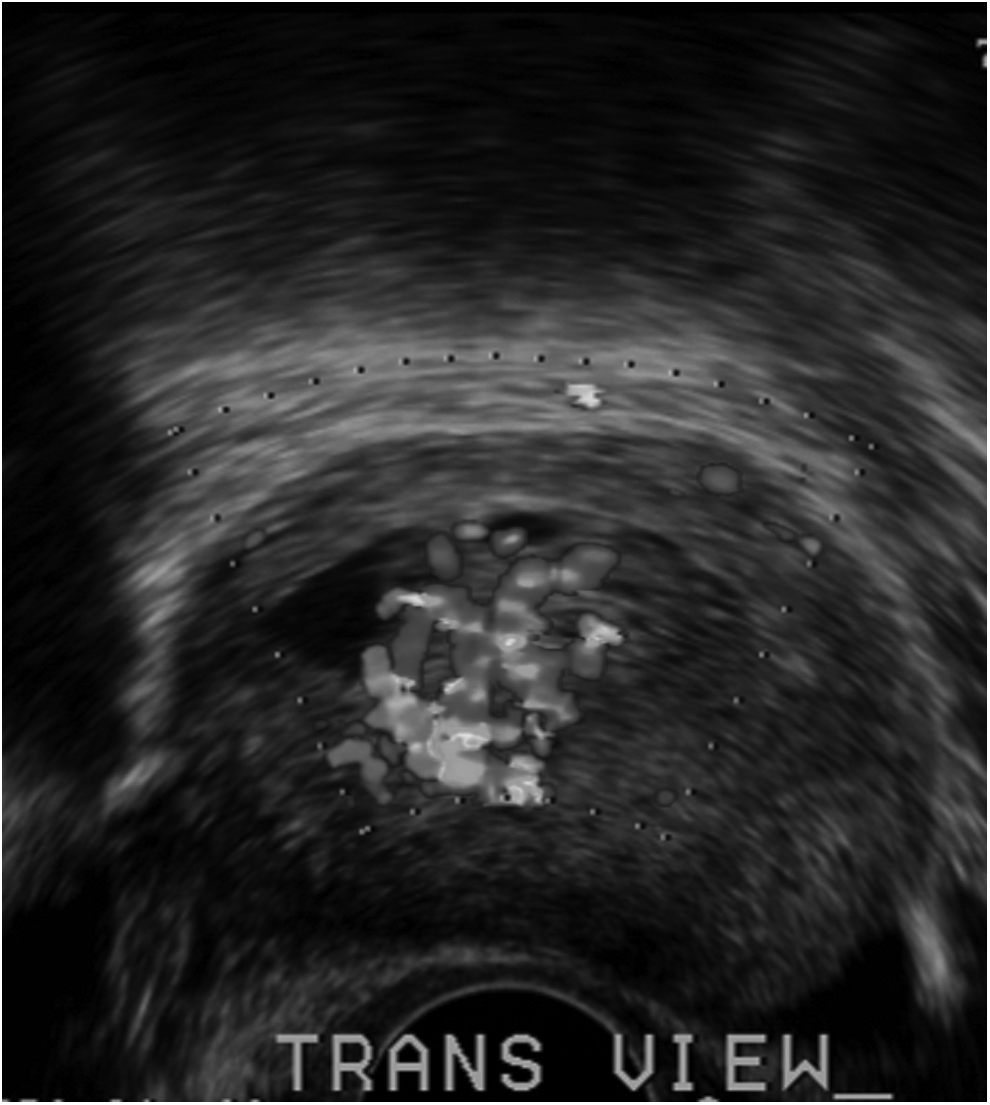
Ultrasound scan of retained molar tissues.
The patient underwent hysteroscopic resection of the retained molar pregnancy. Intraoperative findings showed retained molar tissue at the left cornu of the uterine cavity. During the procedure, electrocoagulation was used to maintain the patient's hemostasis (Fig. 2). Histopathologic findings confirmed the diagnosis of a retained hydatidiform mole. The β-hCG immunostaining showed highlighted trophoblasts and one chorionic villus with hydrophilic changes. Approximately 50% of the trophoblasts were positive for the presence of Ki-67 (MIB-1).

Hysteroscopic resection of retained molar tissues.
Transvaginal ultrasound scanning was performed 2 weeks after the hysteroscopic resection. This scan showed thickening of the patient's endometrium, measuring 1.41 cm. Her β-hCG level decreased to 345.2 mIU/mL. A repeat hysteroscopic resection of the retained molar pregnancy was performed under ultrasound guidance. Intraoperatively, a mass on the left cornual area of the uterus was resected. Histopathologic findings showed the presence of necrotic tissue. The patient received 5 doses of weekly methotrexate (50 mg/IM). Her β-hCG decreased to <2 mIU/mL after the third dose. She received the last 2 doses of chemotherapy as “clean-up” courses, and her β-hCG levels remained at normal levels thereafter.
Results
This patient had an unremarkable follow-up course.
Discussion
This case highlights the utilization of various modalities that can be used for treating retained trophoblastic tissues. After suction D&C, this patient underwent hysteroscopic resection. Another hysteroscopic resection was performed under ultrasound guidance, because of findings of a thickened endometrium. There is a higher likelhood of having retained trophoblastic tissues after conventional blind curettage. Hysteroscopic resection offers direct visualization of the uterine cavity, and selective curettage is performed only on the retained tissues without affecting the normal endometrium. 2
This case presented the authors with a diagnostic and clinical dilemma: Did this patient truly have a retained molar pregnancy or did she have a Stage I gestational trophoblastic neoplasia? Patients with retained products of conception usually present with vaginal bleeding, as manifested by this case. Ultrasound is a useful tool for diagnosing retained products of conception, and the most valuable parameter is the thickening of the endometrium. Other researchers have reported a cutoff value of 10 mm endometrial thickness, which increases the sensitivity of diagnosing retained products of conception by 80%. 3 The current patient had an endometrial thickness of 14.1 mm. Moreover, findings of an intrauterine mass and increased color flow Doppler images noted on ultrasound increase the likelihood of a patient having retained products of conception. However, such findings can still be manifested by gestational trophoblastic neoplasia, particularly if ultrasound finding show some degree of myometrial invasion. Thus, it is quite evident that ultrasound findings of retained products of conception and gestational trophoblastic neoplasia have some similarities. Other diagnostic modalities, such as magnetic resonance imaging (MRI) could be helpful for arriving at a diagnosis, because this imaging could show myometrial invasion clearly. However, MRI is expensive and not necessary for making a decision, as serum β-hCG levels still remain as the final arbiter. 4 The current patient presented with a prior history of a molar pregnancy and increasing serum β-hCG values despite evacuation, which favored a diagnosis of gestational trophoblastic neoplasia more. With this in mind, was the second hysteroscopic resection with ultrasound-guided D&C warranted or could methotrexate have been sufficient to target the trophoblastic tissues? Could the patient have also benefited from the hysteroscopic resection, which decreases tumor load and thereby decreases the number of chemotherapy sessions? The authors believe that the final diagnosis of this case was a Stage 1 gestational trophoblastic neoplasia that was probably an invasive mole.
Immunohistochemical techniques, such as staining for the presence of Ki67, can aid the diagnosis further, because such staining determines the rate of cell proliferation in the cells thereby predicting cell progression. 5 There have been conflicting studies on hydatidiform mole. Cheung et al. noted that Ki67 was not useful for predicting the outcome of molar pregnancies. However, a more-recent study showed that the Ki67 is expressed more in patients with gestational trophoblastic neoplasia than those with uneventful molar pregnancy, thereby showing a high predictive value of progression to gestational trophoblastic neoplasia. 6
Given that the current patient underwent three operations, the issue of intrauterine adhesions must also be addressed. A study of 50 women who underwent repeat curettage for placental remnants showed that 40% of them developed intrauterine adhesions. 7 This high incidence of intrauterine adhesions makes accurate diagnosis and appropriate management of prime importance.
Conclusions
Retained trophoblastic tissues can pose a clinical dilemma for any clinician. This study shows that selective hysteroscopic removal should be considered an alternative to conventional blind evacuation by curettage. This case highlights the utilization of various modalities, such as ultrasound, immunostaining with Ki-67, and ultrasound-guided curettage to arrive at the correct diagnosis and management.
Footnotes
Disclosure Statement
No financial conflicts exist.