
Abstract
Abstract
Introduction
S
In RCTs comparing laparoscopic to abdominal myomectomy, operative time has ranged from similar3,4,6,9 to significantly longer for laparoscopic myomectomy.5,7 In the meta-analysis by Jin et al., operative time was, on average, 13 minutes longer for laparoscopic compared to abdominal myomectomy. 8
In the largest prospective study to date, Sizzi et al. reported on 2050 women undergoing laparoscopic myomectomy between 1998 and 2004. 10 Overall, minor, and major complication rates were 11.1%, 9.1%, and 2%, respectively. Factors associated with complications after multivariable analysis included removal of >3 myomas, an intramural or broad-ligament myoma, and any myoma ≥5 centimeters. Operative time was shorter in patients without complications (106.5 versus 114.1 minutes; p<0.01); however, this association was not significant after multivariable analysis.
Sizzi et al. also found that longer operative time was associated with increasing dominant myoma diameter and number of myomas removed. 10 Other studies have confirmed this finding and have also demonstrated an association between myoma size and increased blood loss. Wang and colleagues reported on 176 laparoscopic myomectomy procedures and noted that myoma weight >80 g was associated with increased operative time (121.5 versus 79.1 minutes; p<0.001), increased blood loss (346.3 versus 123 mL; p<0.001), and blood transfusion (22.1% versus 3.2%; p<0.001); however, there was no difference in length of hospital stay or overall complications between the groups. 11
Similarly, Sinha et al. conducted a prospective study of 51 patients and demonstrated that increased myoma weight was associated with longer operative time (correlation coefficient: 0.77; p<0.001) and increased blood loss (correlation coefficient: 0.81; p<0.001). Because of the small number of complications in this series, conclusions could not be drawn regarding any potential association between operative time, myoma size, and complications. 12
Studies comparing conventional laparoscopic to robotic-assisted laparoscopic myomectomy have shown that operative time may be equivalent or increased with robotic myomectomy, with similar blood loss, hospital stay, complication rates, and fertility outcomes.13–16
The association between operative time and complications has been well-established in the general surgery literature, with many studies isolating operative time as an independent risk factor for postoperative complications, including infectious morbidity, ileus, and increased length of hospital stay.17–21 A large national study by Giger and colleagues identified operative time as an independent risk factor for perioperative complications after laparoscopic cholecystectomy. 20
The multi-institutional American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) was established as a quality-improvement initiative to deepen understanding of surgical outcomes through the prospective collection of data across surgical disciplines. It captures 240 patient variables from more than 460 institutions in the United States and is uniquely poised to assess outcomes data.
The potential relationship between longer operative time and perioperative complications in laparoscopic myomectomy has not yet been delineated clearly. The aim of the current study was to utilize the ACS-NSQIP database to evaluate the association between operative time during laparoscopic myomectomy and 30-day perioperative complications.
Materials and Methods
Data source and population
Data from the ACS-NSQIP database were retrospectively retrieved for all laparoscopic myomectomy procedures recorded from 2005 to 2012 at all institutions participating in NSQIP. Given utilization of de-identified patient data, the Northwestern University institutional review board deemed that formal review was not necessary. The details of ACS-NSQIP data collection methods have previously been described and validated.22–24 Patients were selected using Current Procedural Terminology (CPT) codes for laparoscopic myomectomy, namely, 58545 (1–4 intramural myomas weighing ≤250 g and/or surface myomas) and 58546 (5 or more intramural myomas and/or weight >250 g). Given that CPT codes do not differ between conventional and robotic-assisted laparoscopic myomectomy, NSQIP cannot distinguish between these modalities, and thus both types of laparoscopic myomectomy were analyzed together. Patients were excluded if they had an American Society of Anesthesiologists (ASA) classification of 5, gynecologic cancer, and operative times <20 minutes. Also excluded were patients undergoing concomitant procedures at the time of laparoscopic myomectomy, as identified by CPT code.
Primary outcomes
Primary outcomes of interest were 30-day complication rates in relation to operative time. Surgical complications included superficial, deep, and organ space surgical-site infection (SSI), and wound disruption. Medical complications included: pneumonia; unplanned intubation; ventilator dependence >48 hours; renal insufficiency; acute renal failure; urinary tract infection (UTI); peripheral neurologic deficits; cardiac arrest; blood transfusion; venous thromboembolism, including deep venous thrombosis (DVT) and pulmonary embolism (PE); sepsis/septic shock; and death. Overall complication rates encompassed patients with ≥1 surgical or medical complications.
Definitions of complications were based on NSQIP criteria. UTI was defined as: (1) fever, symptoms of UTI, and culture with >105 colonies/mL of single organism; or (2) fever or symptoms plus: positive dipstick; pyuria; positive gram stain; two cultures with >102 colonies/mL of the same uropathogen; <105 colonies/mL of a single uropathogen in a patient being treated with antimicrobial therapy; or physician's diagnosis. DVT was defined as identification of a new blood clot via duplex, venogram, or computed tomography (CT) scan. The patient must have been treated with anticoagulation therapy, placement of a vena cava filter, or clipping of the vena cava. PE was defined as a V–Q scan interpreted as high probability of PE or a positive CT spiral examination, a trans-esophageal echocardiogram, a pulmonary arteriogram, or a CT angiogram. Return to the operating room was defined as any scheduled or unscheduled return to the operating room within 30 days. Operative time was defined as minutes from initial incision to closure.
Statistical analysis
Patient demographics, comorbidities, and procedural variables were tracked as potential risk factors for both prolonged operative time and complications. Operative times were divided into 60-minute intervals. Within these intervals, the frequencies of overall, surgical, and medical complications, and return to the OR were calculated.
Based upon the observed inflection point at 240 minutes for both overall and medical complications, patients with operative times <240 and ≥240 minutes were compared. Bivariate analyses were performed to identify clinical and procedural variables associated with operative times ≥240 minutes and variables associated with complications; and to assess the association between operative times ≥240 minutes and complications. Comparisons were performed using Chi-square or Fisher's exact tests for categorical variables and independent samples t-tests for continuous variables.
Multivariable regression modeling was then approached in the following manner: Separate regression models were created for overall complications, medical complications, surgical complications, blood transfusion, and return to the operating room. Initial bivariate analyses were performed for each of these complication categories in order to determine the association between complications and each of the following variables in addition to operative time: age; race; diabetes; smoking; alcohol use; history of chemotherapy or radiation; dyspnea; chronic obstructive pulmonary disease (COPD); congestive heart failure (CHF); previous cardiac surgery or percutaneous cardiac intervention (PCI); hypertension; peripheral vascular disease; hemiplegia; history of stroke or transient ischemic attack (TIA); recent wound infection; disseminated cancer; known bleeding disorder; sepsis/septic shock; prior operation within 30 days; ASA classification; wound infection; outpatient status; myoma bulk (with larger bulk indicated by CPT code 58546); and total relative value units (RVU).
Variables meeting a cutoff alpha value of ≤0.1 on bivariate analysis were included in the multivariable regression model for each complication type. Resident physician involvement was unable to be utilized in final regression modeling, as this variable was only reported for a minority (32.1%) of the study population. Frequency analysis for reported body mass index (BMI) data revealed that multiple data points for BMI reflected inaccurate calculations, which were likely erroneously based on weight in kg rather than lbs; given the inability to retrieve accurate information because of the data de-identification in NSQIP; thus, BMI was excluded from both bivariate comparisons and regression analysis. Separate regression models were created for each complication type based upon operative time as a continuous variable and as a dichotomous variable (<240 or ≥240 minutes). For the continuous models, odds ratios (ORs) per hour of operative time were calculated based on regression results. An alpha value of <0.05 was considered statistically significant for multivariable analyses. All analyses were performed using SPSS, version 21 (Chicago, IL).
Results
For the years between 2005 and 2012, 1017 laparoscopic myomectomy procedures meeting inclusion criteria were identified in the NSQIP database. Of these, 5.5% had operative times <60 minutes, 25.5% between 60 and 119 minutes, 28.9% between 120 and 179 minutes, 19.3% between 180 and 239 minutes, 12.0% between 240 and 299 minutes, and 8.8%>300 minutes. The mean operative time was 172.0 (standard deviation [SD]=89.9) minutes.
A total of 54 patients (5.3%) experienced complications, with the most common complications being blood transfusion (3.4%), SSI (1.1%), and UTI (0.5%). Return to the operating room within 30 days occurred in 0.4% of patients. There were no deaths.
Overall and medical complications increased with increasing operative time (Table 1; Fig. 1). Patients with operative times <60 minutes had an overall complication rate of 1.8%, compared to 16.7% when operative time exceeded 300 minutes. Medical complication rates increased from 1.8% to 15.6% from the shortest to longest operative time intervals. Rates of surgical complications and return to the operating room were low across all intervals; thus, no clear pattern was observed for these categories based on operative time. Both overall and medical complications more than doubled between the 180–239– and 240–299–minute intervals of operative time.
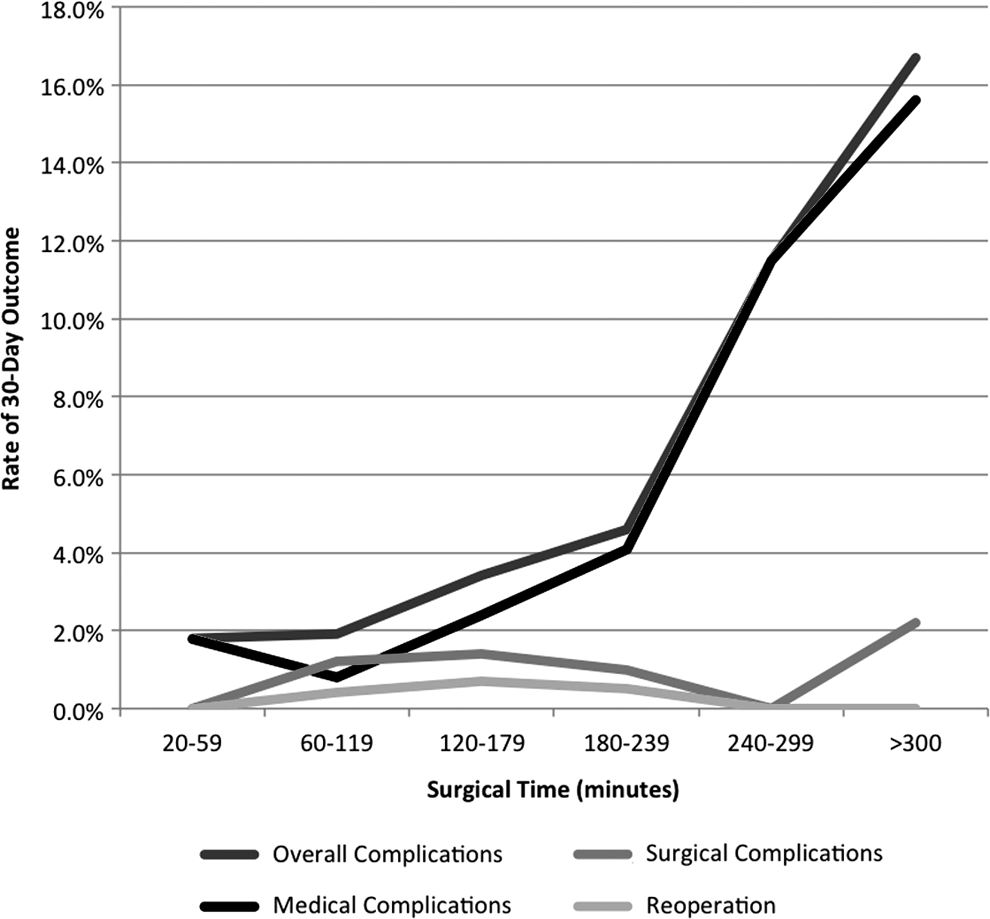
Rates of overall, medical, and surgical complications and return to operating room by 60-minute intervals of operative time.
Patients with operative times <240 and ≥240 minutes were compared (Table 2). Overall, patients were healthy, with rates of diabetes, hypertension, COPD, and smoking reported at 2.8%, 9.1%, 0.5%, and 9.1%, respectively. No patients had histories of CHF, PCI, or cardiac surgery; stroke/TIA; hemiplegia; or disseminated cancer. The majority of patients (93.8%) were classified as ASA class 1 or 2. Patients with operative times <240 and ≥240 minutes were similar with respect to all demographic and clinical characteristics. In procedures for which resident physician involvement was reported, procedures <240 and ≥240 minutes did not differ based on resident physician involvement (68.3% versus 73.8%; p=0.40). Surgical complexity, as estimated by RVU, was also similar for procedures <240 and ≥240 minutes (21.3±7.8 versus 21.3±8.0; p=0.98). Inpatient status (43.4% versus 23.1%; p<0.001) and greater bulk of myomas removed, as indicated by CPT code 58546 (47.6% versus 28.0%; p<0.001), were both significantly associated with operative time ≥240 minutes.
Bolding denotes significant value, p<0.05.
COPD, chronic obstructive pulmonary disease; CHF; congestive heart failure; PCI, percutaneous cardiac intervention; TIA, transient ischemic attack; ASA, American Society of Anesthesiologists; CPT, Current Procedural Terminology; RVU, relative value units; N/A, not applicable.
Compared to operative time <240 minutes, operative time ≥240 minutes was associated with increased overall complications (13.7% versus 3.1%; p<0.001), medical complications (13.2% versus 2.2%; p<0.001), blood transfusion (9.9% versus 1.7%; p<0.001), and pneumonia (1.4% versus 0%; p=0.001). There was no difference in surgical complications or return to the OR between groups (Table 3).
SSI, surgical site infection; UTI, urinary-tract infection; MI, myocardial infarction; DVT, deep venous thrombosis; PE, pulmonary embolism; N/A, not applicable.
Patients with and without complications were similar with respect to all clinical characteristics and comorbidities (Table 4). Operative time was significantly longer in patients experiencing complications (250.0±115.1 minutes versus 167.7±86.3 minutes; p<0.001) and patients with complications were more likely to have operative time ≥240 minutes (53.7% versus 19.0%; p<0.001). Patients with complications were also more likely to have larger myoma bulk as indicated by CPT code 58546 (44.4% versus 31.4%; p=0.045) and inpatient stays (61.1% versus 25.4%; p<0.001). Patients with and without complications were similar with respect to resident physician involvement, when reported (59.1% versus 70.1%; p=0.28), and total RVU (17.5±2.2 versus 16.9±2.0; p=0.07).
COPD, chronic obstructive pulmonary disease; ASA, American Society of Anesthesiologists; CPT, Current Procedural Terminology; RVU, relative value units.
Multivariable regression modeling was performed for overall, medical, surgical complications, blood transfusion, and return to the operating room to determine if there was an independent association between operative time and complications (Table 5). Operative time ≥240 minutes was independently associated with increased risk of medical complications (OR: 5.32; 95% confidence interval [CI] 2.77–10.20; p<0.001), blood transfusion (OR: 4.80; 95% CI: 2.27–10.11; p<0.001), and overall complications (OR: 3.92; 95% CI: 2.17–7.07; p<0.001). When operative time was modeled continuously, it was found to be independently positively associated with medical complications (OR per hour: 1.65; 95% CI: 1.38–1.98; p<0.001), blood transfusion (OR per hour: 1.66; 95% CI: 1.36–2.03; p<0.001), and overall complications (OR per hour: 1.52; 95% CI: 1.29–1.79; p<0.001). Multivariable analysis did not show an association between operative time and surgical complications or return to the operating room. Other variables that were independently associated with complications included inpatient status, preoperative steroid use (associated with medical complications and blood transfusion), wound class >2 (associated with surgical complications), and preoperative sepsis (associated with return to the operating room).
Separate regression models were created for overall complications, medical complications, surgical complications, return to the operating room, and blood transfusion. Risk factors meeting a cutoff alpha value of <0.1 on bivariate analysis were included in the multivariable regression model for each complication type. All results in this table reflect regressions based on continuous modeling of operative time. Regressions based upon operative time as a dichotomous variable are reported in the text.
Bolding denotes significant value, p<0.05.
OR, odds ratio; CI, confidence interval; CPT, Current Procedural Terminology.
Discussion
The relationship between operative time and perioperative morbidity has been extensively discussed in the general surgery literature, but data for gynecology are inconsistent. The current body of literature regarding laparoscopic myomectomy includes several excellent studies that suggest that operative time may be associated with complications. In Sizzi et al.'s large prospective study, operative time was significantly associated with complications on bivariate but not on multivariate analysis. 10 Size and weight of myomas removed correlated with longer operative time in Sizzi et al.'s study 10 and with increased blood loss in two additional studies.11,12 The present study was aimed to investigate the relationship further between operative time and 30-day perioperative complications after laparoscopic myomectomy. There was a direct, independent association between longer operative time and increased 30-day overall complications, medical complications, and blood transfusion.
The overall complication rate in the current study was 5.3%, which was lower than previously reported by Sizzi et al. at 11.1%. 10 This discrepancy is likely explained by differences in definitions of complications and complications included in each study.
For instance, Sizzi et al. reported on several complications that are not tracked in NSQIP, including uterine rupture, bowel injury, sarcoma, uterine-manipulator injury, hemorrhage not requiring blood transfusion, transient fever, and failure to perform the planned procedure. 10 The UTI rate in the current study was 0.5%, compared to 3.4% in Sizzi et al.'s study 10 ; the reason for this difference is unclear but may relate to differing criteria for UTI. The transfusion rate in Sizzi et al.'s study 10 was 0.14%, compared to 3.4% in the current study; again, the explanation for this difference is not clear but may relate to differences in practice patterns or myoma bulk between the two studies. The rate of return to the operating room in the current study was 0.4%, compared to 0.09% reported by Sizzi et al. 10 ; the higher rate in the current study likely relates in part to the fact that return to the operating room in NSQIP includes both scheduled and unscheduled surgeries occurring within 30 days of the index surgery. There were no deaths reported in either study.
In the current study, a significant association was found on bivariate analysis between increasing myoma bulk and both longer operative time and perioperative complications, consistent with the findings of Sizzi et al. and others.10–12 However, after multivariable regression analysis, myoma bulk was not found to be independently associated with overall, medical, or surgical complications and, surprisingly, was also not found to be independently associated with blood transfusion.
In the current study, complications were independently associated with inpatient status; it is logical that longer length of stay may be necessary in patients who are experiencing complications. Steroid use was independently associated with increased risk of medical complications and blood transfusion. While a relationship between steroid use and blood transfusion is not readily explainable, this finding may relate to changes in vasculature or tissue properties that are beyond the scope of this data set. The association of steroid use with medical complications likely relates to increases in infectious complications, such as pneumonia and sepsis. Interestingly, steroid use was not associated with increased surgical complications, a category that includes SSIs.
After multivariable analysis, longer operative time was found to be independently associated with overall complications, medical complications, and blood transfusion. This is consistent with trends noted by Sizzi and colleagues, who found an association between longer operative time and complications on bivariate but not on multivariable analysis. 10
The strengths of the current study included the large number of patients as well as data gathered from many institutions nationwide, allowing for a high degree of generalizability.
The current study had several limitations pertaining to study design and information bias. First, it was not possible to determine surgeon experience; surgeon volume; and exact myoma weight, location, or size—all of which may contribute to longer operative time and to perioperative complications. In order to account for surgeon experience, resident physician involvement was included in bivariate analyses; however, this variable was excluded from regression modeling, as it was not recorded for the majority of the study population. NSQIP cannot determine the extent of trainee involvement in a given surgical procedure or the experience or surgical volume of the primary surgeon.
Furthermore, NSQIP does not specifically track visceral injuries, such as bladder, bowel, ureteral, or major vascular injury, which would likely increase both operative time and complications. By excluding concomitant procedures, several patients with CPT codes indicating visceral injury were eliminated from analysis; however, exclusion of all such patients relies on consistent CPT coding of intraoperative injuries. It was not possible to determine the type or indication of procedures performed at the time of return to the operating room. We also were not able to identify complications or returns to the operating occurring >30 days after the index myomectomy.
As mentioned previously, NSQIP cannot distinguish conventional from robotic-assisted laparoscopic myomectomy in order to analyze complications separately. Although the NSQIP database has been validated and found to have high rates of accuracy and reliability, the current study depended on correct CPT code recording and complication tracking.
Finally, given that NSQIP data are collected from many institutions, it is possible that postoperative care and surgical techniques may vary by institution; these variables are difficult to quantify and could not be controlled for in the current study.
Despite these limitations, our data provided important information from a nationwide database regarding the impact of prolonged operative time on 30-day perioperative complications after laparoscopic myomectomy.
Many studies have analyzed the learning curve associated with minimally invasive gynecologic surgery, with a particular focus in recent literature on robotic-assisted hysterectomy. Lin et al. described significantly decreased operative time in robotic hysterectomy (RH) performed by a single surgeon after the first 20 to 30 cases. 25 Sandadi and colleagues found that gynecologic oncology fellows overcame their learning curve in RH after an average of 33 cases, beyond which operative time decreased. 26 Woelk et al. evaluated the RH learning curves of two surgeons and found that operative time and patient length of stay both decreased over a study period of 36 months. 27 Given decreasing operative time as surgeons overcome initial learning curves and the current study finding that longer operative time is directly associated with complications, there may be a role for increased proctoring and simulation training to help surgeons improve efficiency and decrease operative time as they adopt and maintain minimally invasive myomectomy techniques.
Although laparoscopic myomectomy can be associated with longer operative time than abdominal myomectomy, this approach confers benefits including lower blood loss, decreased postoperative pain, and shorter recovery time.3–8 In a large meta-analysis, overall complication rates were lower for laparoscopic myomectomy, compared to abdominal myomectomy, but major complication rates were similar. 7 Given the current study finding that increased operative time was associated with increased complications after laparoscopic myomectomy, an important future research question will be if there exists an operative time threshold above which a lengthy laparoscopic myomectomy may, in fact, be more morbid compared to a significantly shorter, efficiently performed abdominal myomectomy. Surgeons should be cognizant of the impact of prolonged operative time on postoperative complications in selecting appropriate candidates for minimally invasive myomectomy and in striving to maximize intraoperative efficiency during laparoscopic and robotic myomectomy.
Conclusions
The current study demonstrated an independent association between longer operative time during laparoscopic myomectomy and increased rates of 30-day overall complications, medical complications, and blood transfusion. Based on multivariable regression modeling, for each additional hour of operative time, odds of medical complications would be expected to increase by a factor of 1.65, blood transfusion by 1.66, and overall complications by 1.52. Future research should aim to delineate risk factors further for prolonged operative time in laparoscopic myomectomy, including surgeon experience and volume, patient characteristics, and size and location of uterine leiomyomata. An improved understanding of these risk factors will be valuable in guiding future investigations regarding differential morbidity of abdominal and laparoscopic myomectomy, with the goal of helping surgeons maximize preoperative planning and optimize patient selection for minimally invasive myomectomy procedures.
Footnotes
Disclosure Statement
The authors declare that they have no conflicts of interest and have not received any financial support in relation to this study.