
Abstract
Vaginal hysterectomy is considered the preferred approach for benign hysterectomy due to its cost-effectiveness, safety, and low morbidity. Efforts to increase vaginal hysterectomy utilization, including endorsement by the American College of Obstetricians and Gynecologists and the American Association of Gynecologic Laparoscopists, has had limited impact on national trends. Marketing from companies and shifts in practice patterns along with lack of resident education have exacerbated the problem. Deeply engrained, though unfounded, perceived contraindications to a vaginal approach (e.g., prior surgery, nulliparity, uterine size, and risk factors for extrauterine disease) limits consideration of this approach further. This review presents evidence against these commonly perceived contraindications and provides a peer-reviewed algorithm that can be implemented to increase vaginal hysterectomy utilization safely. As minimally invasive technologies continue to evolve, surgeons have the responsibility to seek candidates that would benefit from the original—and most minimally invasive—approach to benign hysterectomy.
Introduction
The American College of Obstetricians and Gynecologists (ACOG) and American Association of Gynecologic Laparoscopists (AAGL) recommend the vaginal route as the preferred approach to hysterectomy for benign indications owing to its low morbidity and costs.1,2 Nevertheless, national trends for the vaginal approach continue in a steady decline, with the most recent data showing that only 11.5% of commercially insured patients underwent vaginal hysterectomy between 2010 and 2013. 3 The reasons for decreasing vaginal hysterectomy rates are multifactorial. Whereas trainees at the turn of the century had to master vaginal and abdominal hysterectomy, residents today need to learn vaginal, abdominal, laparoscopic, robotic, and single-incision hysterectomy. What compounds the issue is that the number of yearly hysterectomy procedures declined steadily from a peak of 681,234 in 2002 to 433,621 yearly procedures in 2010. 4 Finally, although adnexal pathology, severe endometriosis, adhesions, and pelvic malignancy are unequivocal contraindications to vaginal surgery, 1 for the majority of patients, the overarching limitation to using this approach remains ingrained perceptions of “contraindications.” This article reviews the data refuting these assumptions, offers data comparing the various approaches, and provides an algorithm to increase vaginal hysterectomy utilization safely.
Evidence Based Comparison Among Approaches
Vaginal compared to open
In one study, the mean return to normal activities (9.5 days shorter), operative time (mean difference [MD]: −11.01minutes; 95% confidence interval [CI]: −35.09, 13.08), and hospital stay (MD: −1.07 days; 95% CI: −1.22, −0.92) were significantly shorter following vaginal compared to abdominal hysterectomy. 5 Women undergoing vaginal hysterectomy were more likely to be satisfied with their functional capacity and quality of life (odds ratio [OR]: 2.69; 95% CI: 0.50, 14.42). There were no differences in intraoperative complications or blood loss between these 2 approaches. 5
Vaginal compared to laparoscopic
The laparoscopic approach peaked at 15.5% in 2006 and decreased thereafter to account for 8.6% of cases in 2010. 1 A 2015 Cochrane review found no benefit to laparoscopic-assisted vaginal hysterectomy over vaginal hysterectomy, with vaginal hysterectomy only being associated with shorter operative time (mean difference: 33.69 minutes; 95% Cl: 20.13, 47.07). 5 There were no differences in intraoperative visceral injuries, bleeding complications, conversion rates, return to normal activities, or major short-term (hematomas, infections, or thromboembolic events) or long-term complications (fistulas or urinary dysfunctions) between the 2 approaches.4,5 Although the overall rate of vaginal cuff dehiscence for all routes is low (with an estimated incidence of 0.24–0.39%), 6 it is highest following total laparoscopic hysterectomy (1.35%). 6 The risk of this complication is significantly higher following laparoscopic compared to both abdominal (0.15%; OR: 9.1; CI: 4.1, 20.3) and vaginal hysterectomy (0.08%; OR: 17.2; CI: 3.5, 75.9). 6 Interestingly, a large retrospective cohort showed similar cuff dehiscence rates between laparoscopic and vaginal hysterectomies when the cuff was closed vaginally. 4 This finding suggests that surgical technique, rather than thermal damage during laparoscopic colpotomy, might be the key risk factor for this complication.
Vaginal compared to robotic
Robotic-assisted hysterectomy now accounts for up to 40% of hysterectomies performed for benign indications due to direct-to-consumer marketing, improved ergonomics, and relative ease of suturing, compared to conventional laparoscopy. 4 There are no randomized controlled trials comparing vaginal and robotic hysterectomy. 4 In a retrospective cohort study of women undergoing hysterectomy for benign indications, the robotic approach was associated with higher postoperative complication rates (15.1% versus 8%; p = 0.02), longer operative times (1.2 versus 0.7 hours; p ≤ 0.001), and increased costs, compared to vaginal hysterectomy ($13,619 versus $11,366; p < 0.001).4,7
Approaches to Improve Vaginal Hysterectomy Utilization
Increasing vaginal hysterectomy utilization based on clinical guidelines has been evaluated. Kovac et al. applied a simple algorithm to alter the rate of abdominal to vaginal hysterectomy from 3:1 to 1:11.
8
Patients requiring hysterectomy for benign indications were offered a vaginal procedure if:
Vaginal caliber was more than 2 finger breadths at the apex (no-one was excluded for this indication). There was ≥ grade 1 apical prolapse. For women who had limited uterine descensus in the clinic, the final route was chosen based on descent during examination under anesthesia in the operating room. For patients with suspected extrauterine disease (e.g., history of endometriosis, ruptured appendicitis, or ectopic pregnancy etc.), a diagnostic laparoscopy was performed with a 5-mm scope at the beginning of the case. If uterine enlargement was suspected, an examination under anesthesia was utilized to assess vaginal access.
Application of this simple algorithm allowed for successful completion of vaginal hysterectomy in 91.8% of the patients. 8 Importantly, only 19/407 (4.6%) patients had limited vaginal access and underwent abdominal hysterectomies (note, this was a study from the late 1990s, although it was published in 2002, prior to widespread endoscopic approaches). Among patients with suspected extrauterine disease, no disease or minor disease was found in 90.9% (80/88). There was no need for laparoscopic procedures, and the surgeons simply proceeded with vaginal hysterectomies. Laparoscopic procedures were required in only 6.8% (6/88) of women, who had extrauterine adhesive disease. Finally, in women with estimated uterine weights >280 g (∼ 12 weeks), vaginal hysterectomy was successful in 82.2% (37/45) of these patients following examinations under anesthesia.
Schmitt et al. recently validated a similar, simpler algorithm to improve utilization (Fig. 1). 3 For women presenting with uterine size ≤12 weeks of gestation (280 g), history of ≤1 cesarean delivery or laparotomy, adequate vaginal caliber, and uterine descent greater than half of total vaginal length during outpatient evaluation, vaginal hysterectomy was chosen automatically. If patients had ≥2 cesarean deliveries, limited uterine mobility on clinical examination, or uterine size 13–16 weeks of gestation, an examination under anesthesia was utilized to assess for feasibility for the vaginal route. Finally, women with uterine size ≥17 weeks of gestation were offered abdominal approaches (open, laparoscopic, or robotic). The algorithm's accuracy was assessed retrospectively and validated prospectively. Using presenting patient characteristics, the algorithm predicted that a total of 259 of 365 women studied (71%) would be eligible for vaginal hysterectomy—202 directly and 57 after examinations under anesthesia. Although the algorithm was only followed in 170 (84.2%) of the eligible patients, vaginal hysterectomy was successful in 99% of patients in which it was attempted. Importantly, 95% of these women were discharged within 24 hours of surgery and only 2 intraoperative conversions occurred. 3
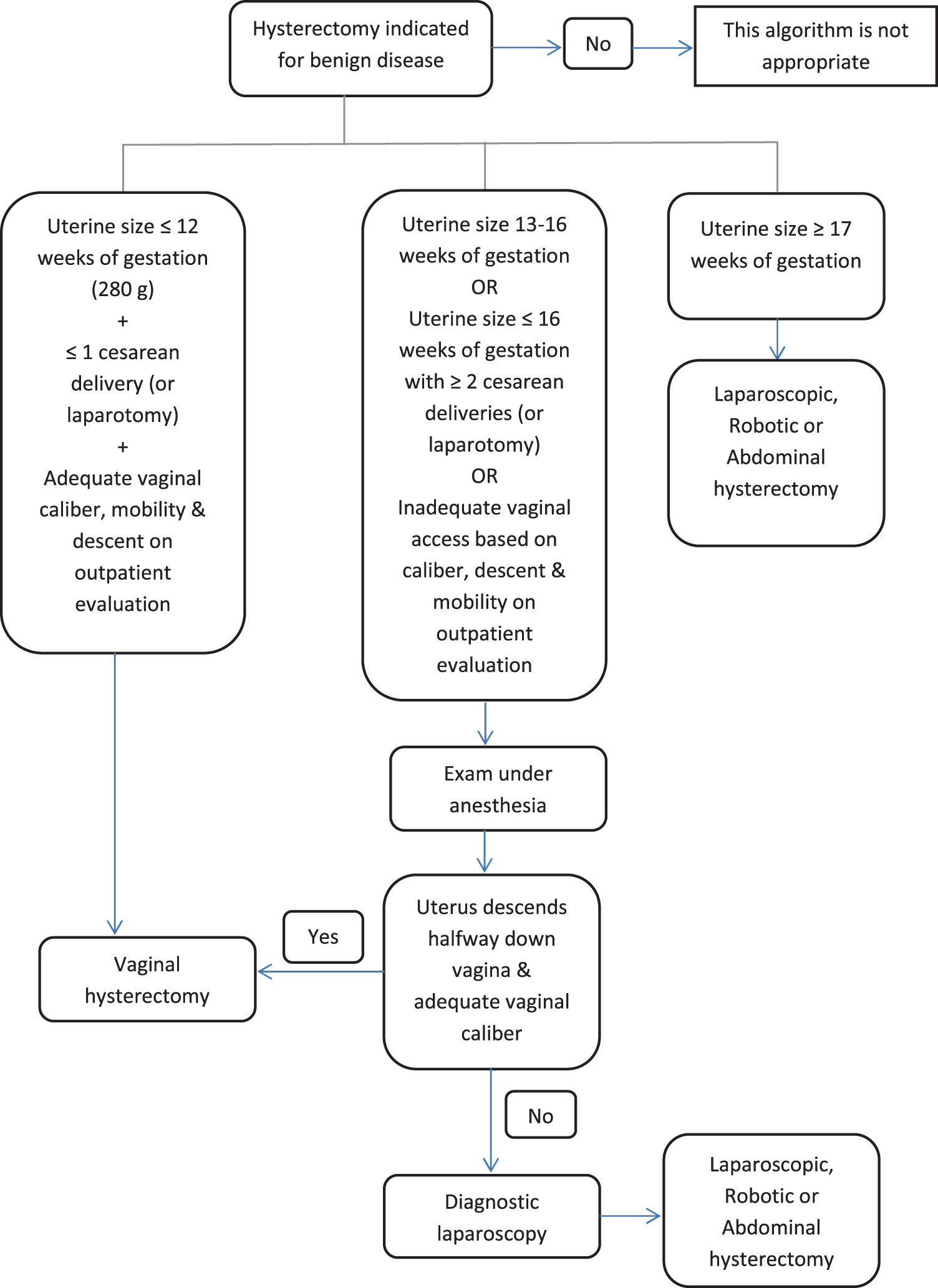
Algorithm to identify candidates eligible for vaginal hysterectomy.
The cited studies above suggest that vaginal hysterectomy can be accomplished safely in most patients presenting with benign indications and provides an evidence-based call for practice realignment, given the steady decline in vaginal hysterectomy utilization nationally. Moreover, these studies highlighted the importance of an examination under anesthesia to determine the route of surgery.3,8 Assessment of descensus should always include a pelvic examination in the lithotomy and standing positions. When descensus remains a concern despite these maneuvers, an examination under anesthesia, with its associated decrease in pelvic-floor tone, allows the surgeon to evaluate the feasibility of a vaginal approach best. 3 If uterus enlargement extends to the pelvic side-walls or if there is persistent limited uterine descensus, abdominal approaches are utilized. In the Mayo Clinic, all patients undergoing vaginal surgery are counseled on the small risk of requiring conversion to other approaches, thereby allowing optimization and individualization of treatment.
Perceived contraindications to vaginal surgery
There are numerous perceived “contraindications” to vaginal hysterectomy, including nulliparity, history of prior laparotomy (primarily cesarean delivery), historical factors associated with extrauterine disease (e.g., endometriosis, ruptured ectopic pregnancy, etc.), obesity, narrow pubic arch, and uterine enlargement. These factors are presumed to limit uterine descensus, making anterior or posterior entry difficult, or preclude vaginal delivery of an enlarged uterus. However, none of these factors have been shown to limit successful vaginal hysterectomy or that this approach is associated with increased morbidity in these patient populations. 9 In fact, a systematic review and meta-analysis of 79 studies showed that vaginal hysterectomy has the lowest rate of bladder and ureteral injuries compared to other approaches. 10 Similarly, the observation that incidental cystotomy rates in women undergoing vaginal hysterectomy with and without previous cesarean deliveries are similar, argues against the concern for increased bladder injuries in this population of women. 11 Finally, numerous surgical series have consistently demonstrated more than 90% success rates for vaginal hysterectomies attempted in nulliparous women, those with enlarged fibroids, or with histories of prior cesarean deliveries. 8
Technical Considerations
Proper positioning can help with visualization and avoidance of nerve injury. 11 The patient's buttocks should be at the edge of the table with the thighs flexed and abducted and the knees flexed with minimal external rotation. 11 Careful attention to padding minimizes the risk of nerve injury further. The initial cervicovaginal incision is made circumferentially and deep. This allows for proper identification of the surgical dissection plane and safe anterior and posterior entries. In certain patients (e.g., history of prior cesarean deliveries, large anterior fibroids or cervical elongation), anterior entry can be delayed. In these cases, the bladder is mobilized off the cervix and lower uterine segment, allowing for safe transection of the uterosacral and cardinal pedicles with the bladder deflected with a Deaver retractor. 11 Moreover, these maneuvers allow for the “creation” of descensus and identification of the peritoneal reflection. With smaller uteri, digital palpation around the fundus helps the surgeon identify a safe plane for entry. Finally, one can backfill the bladder to delineate the surgical planes better and avoid bladder injury.
There is no evidence that women undergoing vaginal hysterectomy for fibroids are at increased risk of visceral injury, requiring blood transfusions or needing prolonged hospital stays. Typically, however, women with uterine sizes >10 weeks will require debulking to deliver the enlarged uterus safely. In order to debulk the uterus safely, it is imperative to secure the uterine blood supply before starting to morcellate. Once the uterine vessels are secured, the cervix is bivalved and a wedge is resected from the anterior and posterior myometrium to expose the fibroids (Fig. 2). Keeping instruments within the serosa, the fibroids are sequentially excised until vaginal delivery and securing of the utero-ovarian pedicles can be achieved. Although this is safe, patients undergoing uncontained morcellation should be counseled about the risk of undiagnosed malignancy and potential inadvertent spread during morcellation (estimated range from 1:360 to 1:7400). 12 It is important to emphasize that morcellation in the setting of undiagnosed malignancy does not appear to alter prognosis or morbidity. 13 Patients who are unwilling to incur these risks should be offered abdominal or laparoscopic/robotic hysterectomies (with contained morcellation in a bag) to avoid potential intraperitoneal dissemination.
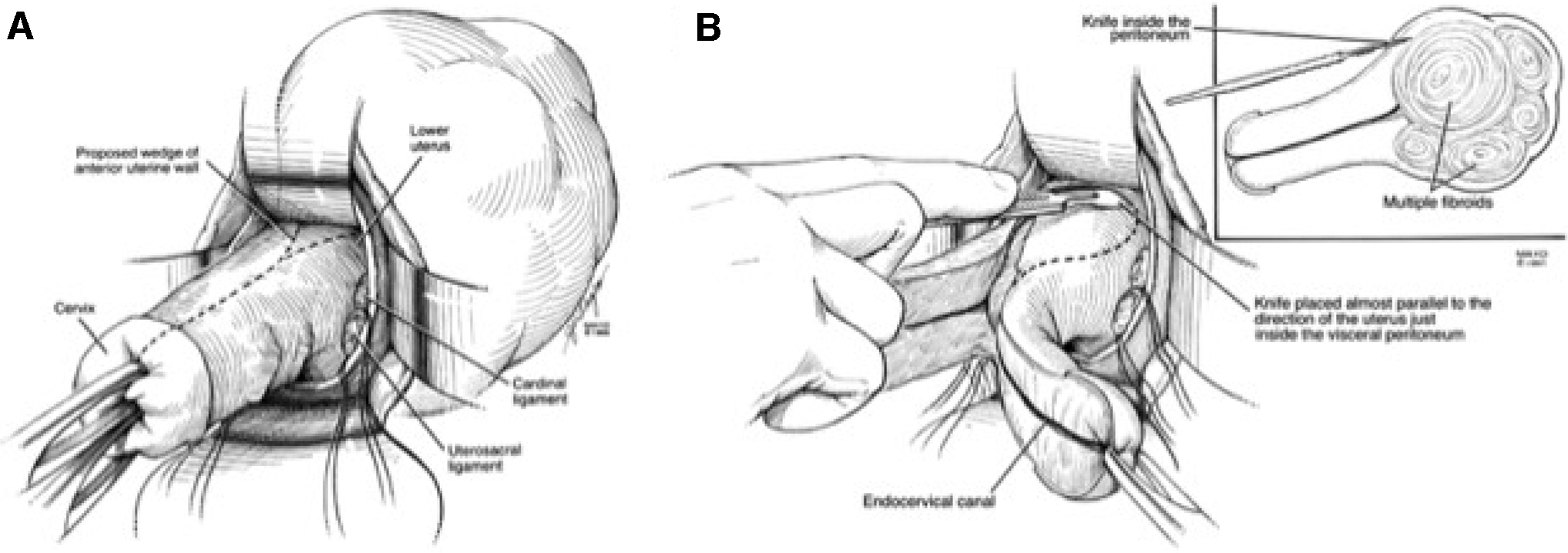
Uterine morcellation technique.
Adnexectomy can also be performed safely via the vaginal route. A 2015 study demonstrated that opportunistic salpingectomy at the time of vaginal hysterectomy was successful in 88% of cases. 14 In the Mayo Clinic, the utero-ovarian pedicles are tagged to facilitate identification of the adnexa for opportunistic salpingectomy or for oophorectomy; similar success has occurred with adnexectomy. These data suggest that laparoscopic assistance is typically not required for adnexal surgery at the time of vaginal hysterectomy. Advanced bipolar devices can also be used during vaginal hysterectomy, as they have demonstrated shorter operative times and lower blood loss compared to conventional suturing. 15 However, these advantages should be weighed against device costs because systematic reviews have found no net benefit for bipolar devices compared to suturing. 15 One can consider using these devices in cases when increased blood loss or prolonged operative time is expected (e.g., class 3 obesity or enlarged fibroids).
Risk of prolapse
Another commonly accepted—though erroneous—misconception, is that vaginal hysterectomy predisposes a patient to a future apical prolapse. A review of the literature shows unequivocal evidence that preexisting prolapse, rather than mode of hysterectomy, is the key determinant of a future prolapse. A large population-based cohort was used to evaluate the incidence of subsequent pelvic-floor repairs among women who had a hysterectomy with and without combined prolapse repairs between 1965 and 2002. 16 In patients with no preexisting prolapses, the cumulative incidence of subsequent pelvic-floor repairs at 20 years follow-up was similar—and extremely low—between patients who had abdominal or vaginal hysterectomy (2.1% versus 1.9%, respectively). 16 However, the incidence of subsequent pelvic-floor repairs increased to 9.5% in women who had baseline prolapse and underwent isolated vaginal hysterectomy. 16 In contrast, in those who had concomitant prolapse repairs at the time of vaginal hysterectomy, the incidence subsequent pelvic floor-repairs decreased to 4.4%. Other researchers have similarly reported that the risk of subsequent repairs increases with increasing grade of prolapse beyond grade 2, of any compartment, at baseline. Prophylactic apical suspension should be considered at the time of benign hysterectomy to decrease the risk of posthysterectomy prolapse (Fig. 3).
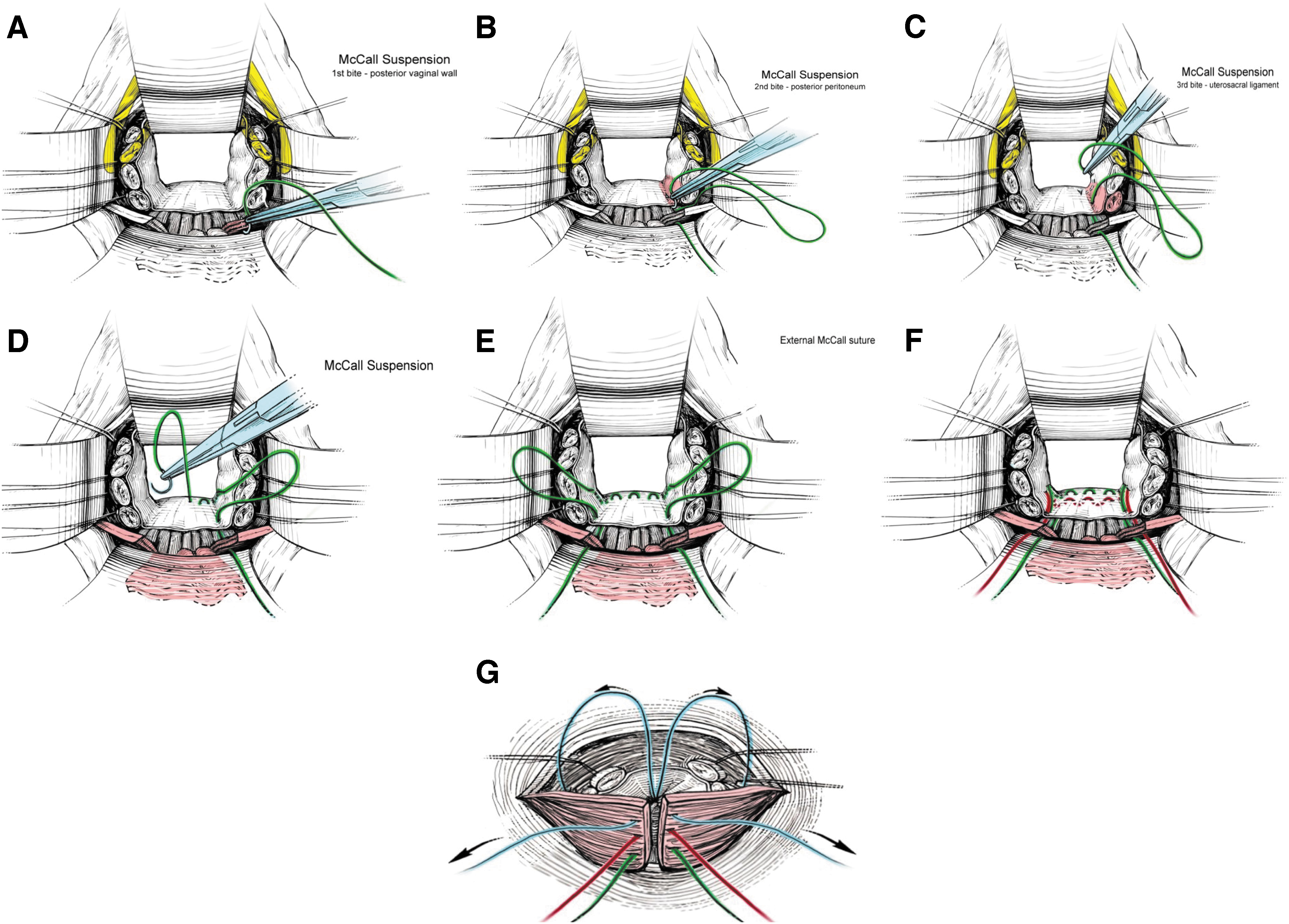
Mayo Clinic's McCall's culdoplasty technique for apical suspension.
Feasibility of outpatient surgery
Not only can vaginal hysterectomy be accomplished safely in patients with perceived contraindications, these procedures can be performed in an outpatient setting. Over the last decade there has been an emphasis on same-day discharge following hysterectomy. 17 In a large cohort of 1071 vaginal hysterectomy cases, Zakaria and Levy described successful same-day discharge of 96% of these patients. 18 Successful protocols were established, including extensive preoperative counseling, preemptive medical management of nausea, continuous nonsteroidal anti-inflammatory drugs with opioids for breakthrough pain, early ambulation, return to regular diet, and daily telephone contact postoperatively. Intraoperatively, these researchers described local infiltration of a paracervical block along with injection into the round ligament and utero-ovarian ligaments. Of this cohort, 46% had additional procedures, including adnexectomy, anti-incontinence procedures, and vaginal repairs. 18 Another misperception is that patients with prolapse repair require overnight stays. However, in a cohort of patients with vaginal reconstructive surgery, successful early adoption of same-day discharge occurred in 64% of patients. 17 The Mayo Clinic has now converted to increasing same-day discharge for most patients who undergo vaginal reconstructive surgery.
Impact on trainees
Changing national hysterectomy trends, with fewer hysterectomies and more approaches, have had a significant impact on gynecologic practice and surgical training. Seventy-four percent of residents report a negative impact of robotic surgery on their training, and only 28% of graduating residents report that they are “completely prepared” to perform vaginal hysterectomy. 4 To address this problem among new graduates, the ACOG has created simulation programs geared to improve vaginal surgical skills. Alternatively, pursuing mentorship with a skilled vaginal surgeon may provide another vehicle for new graduates to hone their post-training vaginal surgical skills. There is a clear and urgent need to increase residents' exposure to vaginal surgery. The current authors believe that implementation of the vetted algorithm described above can be a mechanism to begin to improve resident training and change national trends in vaginal hysterectomy utilization.
Conclusions
Vaginal hysterectomy should be considered the primary route for patients requiring surgery for benign disease, as this approach has been shown to be the safest and most cost-effective surgical one. Application of a simple algorithm (Fig. 1) revealed that nearly three-quarters of women are eligible for a vaginal approach. What is equally important is that these hysterectomies were completed vaginally when attempted 99% of the time. 3 Examination under anesthesia and diagnostic laparoscopy are underutilized tools that have been shown to assess the feasibility of a vaginal approach effectively and should be encouraged. Concerted efforts by national societies, mentors, and by residency programs will be required to train vaginal surgeons adequately to begin to change national trends in vaginal hysterectomy.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was provided for this study.