
Abstract
Objective:
The aim of this study was to establish the effective and prognostic value of the log of odds (LODDS) of positive lymph nodes for predicting the survival of patients undergoing surgical staging for endometrial cancer (EC).
Materials and Methods:
This retrospective cohort study used the Surveillance, Epidemiology, and End Results (SEER) database of EC cases diagnosed from 2010 to 2015. The LODDS was calculated using the equation:
when pLN = number of positive lymph nodes and nLN = number of negative lymph nodes. LODDS and FIGO staging were compared, using a Kaplan–Meier (K–M) analysis and univariate Cox regression modeling to analyze the risk factors for survival. The independent prognostic effect of univariate Cox model variables was evaluated with a multivariate Cox regression model.
Results:
The analyses included 3230 EC cases from the SEER database (International Federation of Gynecology and Obstetrics [FIGO] stage IIIC1 = 1546, FIGO stage IIIC2 = 958, and FIGO stage IV = 726). Among these cases, 58.0% had high-grade histology (FIGO grade 3–4) and 59.0% were classified as type II EC. There were 925 EC-specific deaths. Cases were categorized into 2 groups: (1) LODDS < −0.12707 and (2) LODDS ≥ −0.12707. K–M curve analyses showed 1-, 3-, and 5-year disease-specific survival (DSS) rates of 93.9, 75.9, and 67.5% for LODDS < −0.12707; and 78.6, 49.6, and 38.1% for LODDS ≥ −0.12707, respectively. Cumulative 1-, 3-, and 5-year DSS were 91.0, 71.1, and 62.2%, respectively. In multivariate analysis, LODDS is an independent prognostic factor for EC mortality (hazard ratio = 2.14; 95% confidence interval: 1.85–2.47; p < 0.0001).
Conclusions:
LODDS classification has significant prognostic value for survival among patients with EC. (J GYNECOL SURG 38:278)
Introduction
Endometrial cancer (EC) is the most-common gynecologic malignancy in the United States; 65,620 new cases and 12,590 deaths were expected in 2020. 1 EC is dichotomized into 2 types: (1) type I ECs have predominately well-differentiated (grade 1) and moderately differentiated (grade 2) endometrioid histologies, are associated with unopposed estrogen, have superficial myometrial invasion, and favorable prognoses; and (2) type 2 ECs have more-aggressive tumor types, deep myometrial invasion, a high frequency of lymph-node metastases, and poor prognoses. 2 The mainstay of treatment is primarily surgery comprising extrafascial hysterectomy, removal of the adnexa, and evaluation of lymph-node status by lymphadenectomy, lymph-node sampling (LNS), or sentinel lymph-node (SLN) biopsies.
Lutman et al. demonstrated that removal of >11 pelvic lymph nodes was associated with improved overall survival (OS) and progression-free survival (PFS) in patients with poorly differentiated EC. 3 This association of improved outcomes after lymphadenectomy has been shown in numerous studies specifically for intermediate- and high-risk ECs.3,4 The presence of lymph-node metastases portends a poor 5-year disease-specific survival (DSS), compared to localized disease.5,6
Currently, lymph-node status is based on the presence of lymph-node metastases regardless of the number of resected lymph nodes. However, this may not reflect the true nodal burden of disease accurately. Several multicenter retrospective studies of EC found the lymph-node ratio (LNR) to be associated with worse PFS and OS. 7 Over the last few years, the log odds (LODDS) of positive lymph nodes (pLNs) has been emerging as an alternative predictive factor of outcomes in ovarian, 8 cervical, 9 and colorectal cancers.10–12 LODDS' utility for EC is unknown.
The primary aim of this study was to examine the relationship between LODDS and DSS in patients at advanced stages of EC.
Materials and Methods
Patient selection
This was a retrospective study for which data were obtained from the Surveillance, Epidemiology, and End Results (SEER) database consisting of 18 population-based cancer registries. This population-based cancer registry is sponsored by the National Cancer Institute and comprises ∼48% of the U.S. population. Cases of EC from January 1, 2010, to December 31, 2015, were extracted, using the International Classification of Diseases (ICD) code, C54.1. The inclusion criteria for selected cases were: (1) primary adenocarcinoma of the endometrium without multiple primary cancers elsewhere; (2) age 20 years or older; (3) International Federation of Gynecology and Obstetrics (FIGO) stages IIIC and IV; and (4) at least 1 lymph node submitted for pathologic examination.
International Classification of Disease for Oncology, Third Edition (ICD-O-3)* codes used were 8380-8383 (endometrioid adenocarcinoma), 8140 (adenocarcinoma, not otherwise specified), 8560,8570 (adenocarcinoma with squamous differentiation), 8441, 8460, 8461 (serous), 8323 (mixed-cell), 8310 (clear-cell), and 8480-8482 (mucinous). ECs are categorized into type 1 and type 2 cancers. Type 1 EC includes adenocarcinoma, adenocarcinoma with squamous differentiation, grade 1 endometroid adenocarcinoma, and grade 2 endometrioid adenocarcinoma. Type 2 EC includes serous carcinoma, mixed-cell, clear-cell, grade 3 endometrioid adenocarcinoma, and grade 4 (undifferentiated/dedifferentiated) endometrioid adenocarcinoma.2,13
Cases were excluded if the following information was unknown: race; tumor grade; stage; tumor size; nodal status; and survival information. In all, 22 patients were excluded from this study.
Given that the SEER database is public-use data, the University of Kentucky, Lexington, KY, USA, deemed that an institutional review was not required.
Study variables and clinical factors
Demographic, clinicopathologic, and treatment factors were extracted from the SEER database. Data were extracted for the following variables: age at diagnosis; year of diagnosis; race; histologic type; histologic grade; tumor location; stage; tumor size; number of resected lymph nodes (rLNs); number of pLNs; survival time; and cause of death. Tumor staging was in accordance to the FIGO staging system from the American Joint Committee on Cancer (AJCC) 7th Edition TNM Staging System.** Stage IIIC EC is subdivided into stage IIIC1 (T1-3, N1/N1mi/N1a, M0) and stage IIIC2 (T1-3, N2/N2mi/N2a, M0). Histologic grade was subdivided according to current FIGO definitions: well-differentiated (grade 1); moderately differentiated (grade 2); poorly differentiated (grade 3); and undifferentiated/dedifferentiated (grade 4).
DSS was the primary endpoint for the study. DSS was calculated as the time from the date of diagnosis to the date of EC-specific death. Cases of patients who died from other causes or were alive at the time of the last follow-up were censored.
Statistical analyses
LNR was defined as the ratio between the number of metastatic lymph nodes and the total number of negative lymph nodes (nLNs). The LODDS was defined as the logarithm of the ratio of the probability (odds) of a lymph node to contain metastasis and the probability of being an nLN. It was estimated as:
when pLN is the number of positive lymph nodes, nLN is the number of negative lymph nodes, and 0.5 is added to both pLN and nLN to eliminate the possible production of a singularity (i.e., an infinite value). 14
To identify the best predictor for outcome measures, C-statistics and receiver operating characteristic (ROC) curves were compared for: (1) number of nodes examined; (2) number of pLNs; (3) LNR; (4) LODDS; and (5) index of pLNs, defined as patients who had pLNs identified from surgery.
Using the Harrell's C-index statistic, we were able to compare the prognostic performance of each lymph-node classification. The value of the Harrell's C-index statistic ranges from 0.5 (no discrimination) to 1 (perfect discrimination), and the largest value was chosen as the best prognostic prediction model. LODDS performed the best, compared to the other lymph-node classifications even when accounting for covariates (Supplementary Figs. S1–S4; supplementary data are available online at www.liebertonline.com/gyn). Additionally, when using Uno's concordance statistical method, 15 LODDS had a consistently statistically significantly better performance, compared to other lymph-node classification methods (Supplementary Tables S1 and S2).
Cutoff values for LODDS were selected from ROC curves for 3- and 5-years, based on maximum values from the sum of sensitivity and specificity. The 3- and 5-year cutoff values for LODDS were −0.12707 and −0.25889, respectively. The cutoff values selected in this study were based on the Youden Index (J)—a maximum potential of effectiveness of the diagnostic test. It has been widely used as an optimal cutoff selection method for ROC curves and is calculated as:
For the primary analysis, the 3-year LODDS value was, used as most deaths (65%) occurred by 36 months. By 5 years, death occurred in nearly 95% of patients; thus, the 5-year LODDS value was utilized for a sensitivity analysis.
The prognostic effects of LODDS were evaluated using a log-rank test. Kaplan–Meier (K–M)curves were used to compare the performances of LODDS and FIGO stage. A univariate Cox regression model was used to analyze the risk factors for survival outcome. A multivariate Cox regression model was used to evaluate the independent prognostic effect of the significant variables identified from the univariate Cox model. LODDS was utilized as a continuous variable in the Cox regression model.
Data were analyzed using SAS (version 9.4, SAS Institute, Cary, NC, USA), and all statistical tests were 2-sided with a significance level of 0.05.
Results
Patients' characteristics in the SEER Database
A total of 3230 patients with EC drawn from the SEER database were included in the analyses. There were 925 EC-specific deaths.
The clinical and histopathologic characteristics of the patients are shown in Table 1. The data indicated that patients were mainly Caucasian (75.6%), followed by African American (12.0%). Of the total patients with EC, 1307 (40.6%) were classified as type 1 EC while 1906 (59.0%) were classified as type 2. Pathologically, 58.0% (1874) patients were diagnosed with grade 3–4 disease, while the remaining patients had well-to-moderately differentiated disease. There were 2504 (77.5%) stage III and 726 (22.5%) stage IV cases. With regard to the various lymph-node classifications, the average number of lymph nodes examined was 17.66 (standard deviation [SD] = 13.05), number of pLNs was 3.44 (SD = 5.32), the LNR was 1.05 (SD = 4.53), and the LODDS was −1.314094 (SD = 1.424115), as shown in Table 1.
Clinical and Demographic Characteristics of Study Cohort
yrs, years; LODDS, log of odds; pLNs, positive lymph nodes; LNR, lymph-node ratio.
The cumulative 1-, 3-, and 5-year DSS rates for all patients were 91.0%, 71.1%, and 62.2%, respectively. The median follow-up time for the entire cohort was 29 months (range = 0–83). This cohort did not reach the median survival time and, therefore, this was not calculated.
Prognostic value of LODDS in advanced EC
The K–M survival analysis stratified by FIGO stage is presented in Supplementary Fig. S5. The analysis demonstrated decreasing DSS with increasing FIGO stage (p < 0.0001), and the 5-year DSS was 71.4%, 63.4%, 63.1%, and 37.8%, for FIGO stage IIIC1, stage IIIC2, stage IVA, and stage IVB, respectively (Supplementary Fig. S5; p < 0.05). The log-rank test demonstrated that LODDS was statistically significantly associated with DSS. Using the 3-year LODDS cutoff value of −0.12707, the 1-, 3-, and 5-year DSS rates were 78.6%, 49.6%, and 38.1%, respectively (Fig. 1; p < 0.05). When examining the effects of LODDS by FIGO stage, all stages (except for FIGO stage IVA) demonstrated worse DSS with increasing LODDS (Fig. 2 and Supplementary Fig. S6; p < 0.05 for FIGO stages IIIC1, IIIC2, IVB; p > 0.05 for FIGO stage IVB).
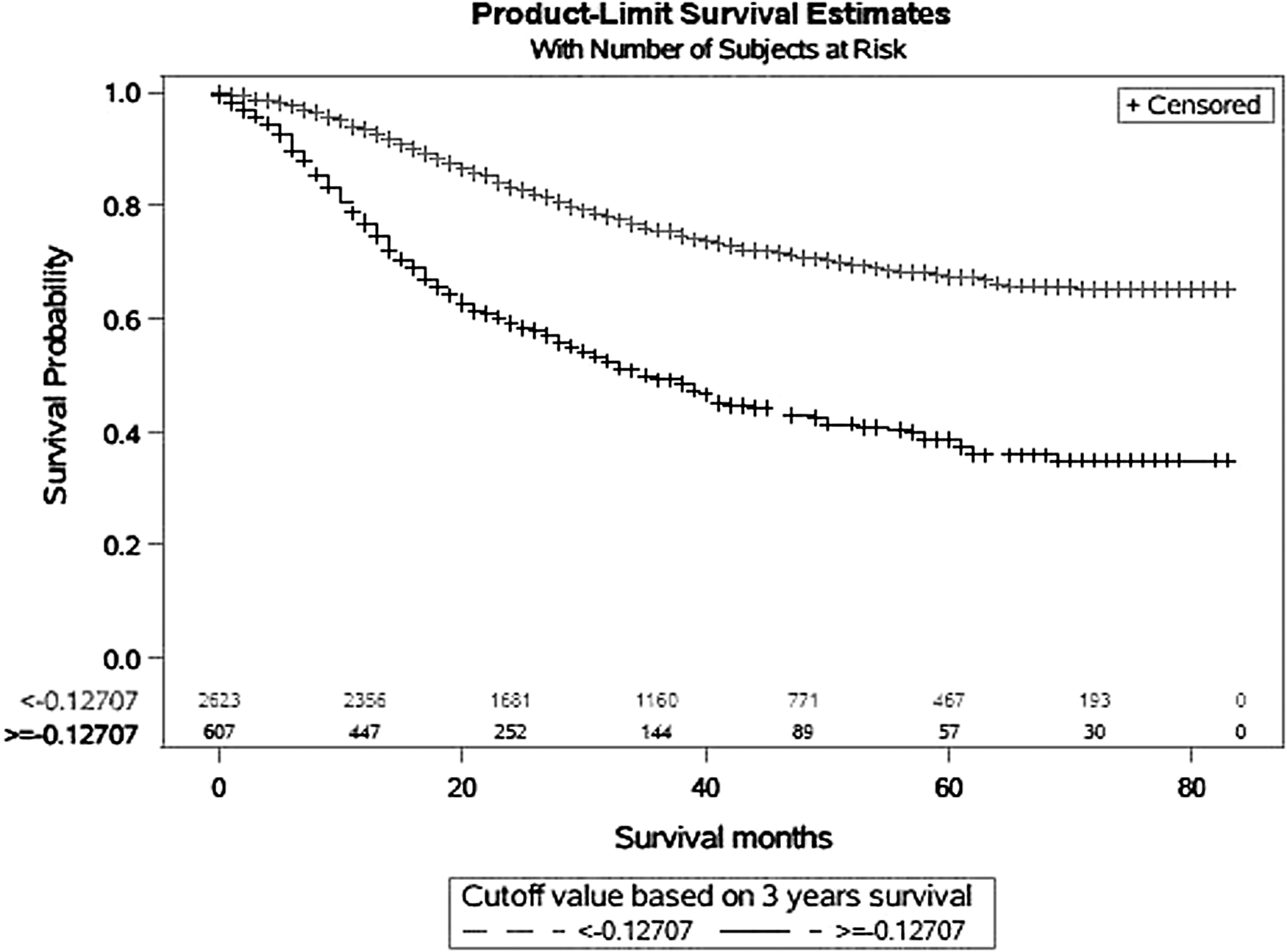
Cumulative disease-specific survival analysis of study cohort stratified by 3-year LODDS [log of odds] cutoff value.
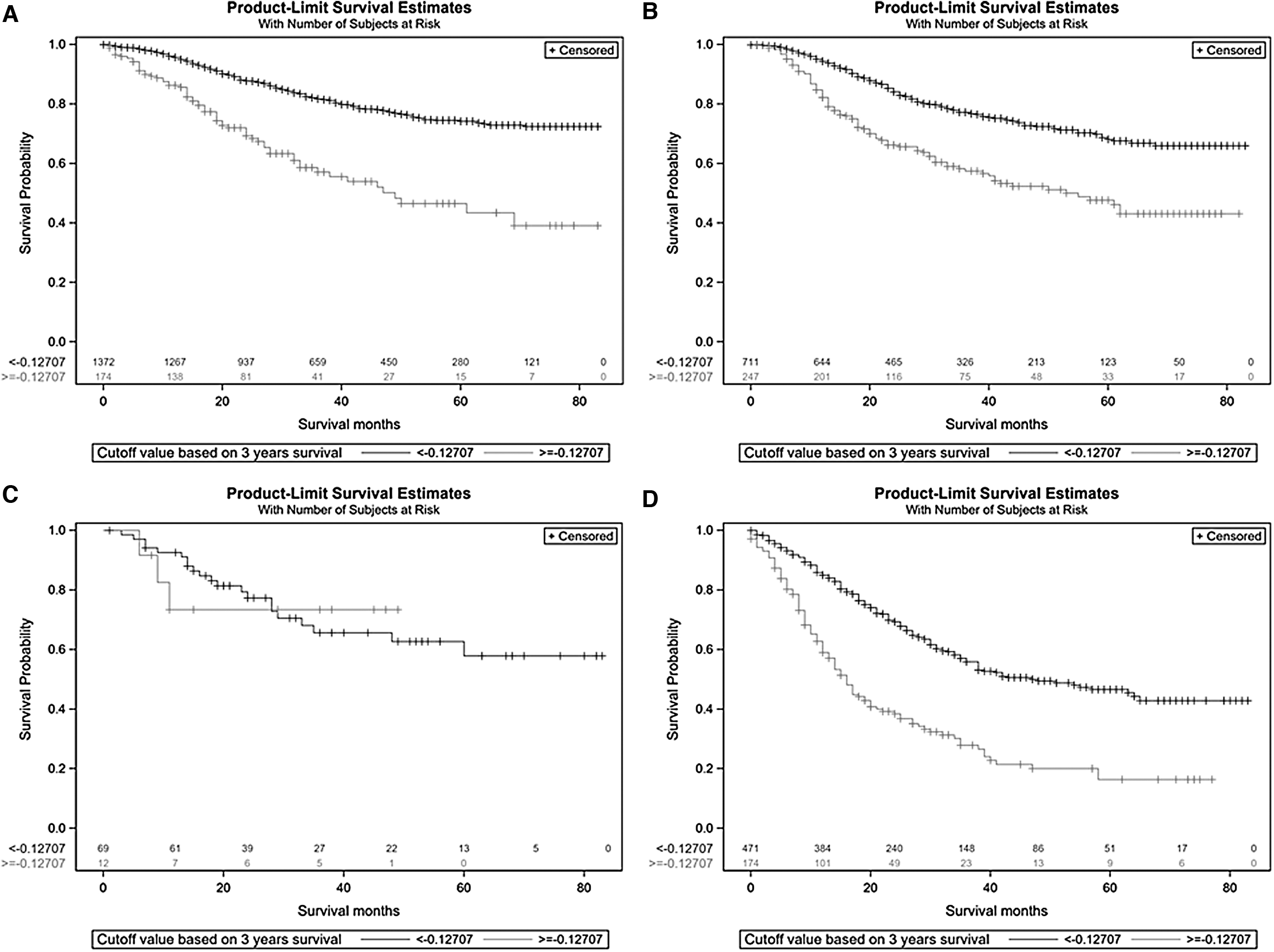
Disease-specific survival analysis of study cohort stratified by 3-year LODDS [log of odds] cutoff values and International Federation of Gynecology and Obstetrics (FIGO) stage
A similar decrease in OS was found with 1-, 3-, and 5-year OS rates of 75.7%, 43.3%, and 30.5%, respectively (Supplementary Fig. S7; p < 0.05). As with DSS, when analyzing the effects of LODDS by FIGO stage, patients with LODDS ≥ −0.12707 had poorer OS (Supplementary Figs. S8 and S9). When performing the sensitivity analysis using the 5-year LODDS cutoff value of −0.25889, a decrease in DSS and OS were observed (Supplementary Figs. S10 and S11; p < 0.05).
To determine if LODDS was an independent factor associated with DSS in patients with advanced EC, univariate and multivariate descriptive analyses were performed, analyzing LODDS as a continuous value. Univariate and multivariate analyses showed that a higher LODDS was significantly and independently associated with a poorer DSS (hazard ratio [HR] = 2.14; 95% confidence interval [CI]: 1.849–2.473; p < 0.0001). See Table 2. These analyses also indicated that age, race, FIGO grade, FIGO stage, and tumor size were significant prognostic factors. Similar results were obtained in the Cox regression model for overall survival (Supplementary Table S3).
Cox Regression Model for Disease-Specific Survival Using 3-Year LODDS Cutoff Value
LODDS, log of odds; HR, hazard ratio; CI, confidence interval; yrs, years; Ref., referent (group).
Sensitivity analysis using the 5-year LODDS cutoff value of −0.25889 revealed an independent association with poorer DSS (HR = 2.10; 95% CI: 1.82–2.42; p < 0.0001) and OS (HR = 1.98; 95% CI: 1.74–2.26; p < 0.0001; Supplementary Tables S4 and S5).
Discussion
The primary aim of this study was to examine the relationship between LODDS and DSS in patients who had advanced-stage EC. Compared to other lymph-node classification systems, LODDS was found to be a superior method (Supplementary Figs. S1 and S2 and Supplementary Table 1). Using a LODDS cutoff value of LODDS −0.12707, 1-, 3-, and 5-year DSS rates were statistically significantly lower when LODDS ≥ −0.12707. When stratified by FIGO stages, 1-, 3-, and 5-year DSS rates were statistically significantly lower when LODDS ≥ −0.12707 for FIGO stages IIIC1, IIIC2, and IVB (p < 0.05). This effect was not seen for FIGO stage IVA (p > 0.05). Similar decreases in OS were found with increased LODDS even when stratifying by FIGO stages.
A sensitivity analysis using the 5-year LODDS cutoff value of −0.25889 confirmed these findings. This study demonstrated that, although FIGO stage is associated with survival, LODDS adds a significant and unique influence upon survival prediction for women with advanced EC.
Lymph nodes and EC survival
Lymphadenectomy and lymph-node status have significant effects on prognosis for patients with EC. Researchers from Duke University (Durham, NC, USA) determined that removal of ≥12 pelvic lymph nodes influenced survival in patients with high-risk EC. Lutman et al. found that patients with high-risk EC histology with removal of ≥12 pelvic lymph nodes had significantly greater 5-year OS (90% versus 64%; p < 0.001) and PFS (87% versus 55%; p < 0.001), compared to patients with similar histology and <12 pelvic lymph nodes removed. 3 A lymph-node count ≥12 was an independent factor for OS (HR = 0.28; p < 0.05) and PFS (HR = 0.29; p < 0.05). 3
It is also known that having metastatic disease to lymph nodes affects 5-year DSS negatively, compared to localized disease. The Molecular Markers in Treatment in Endometrial Cancer (MoMaTEC) study group reported that patients with nodal metastasis had poorer 5-year DSS (FIGO stage IIIC1 = 60% and FIGO stage IIIC2 = 53%), compared to disease locally confined to the uterus and/or cervix (FIGO stage IA = 96%, FIGO stage IB = 87%, and FIGO stage II = 80%). 5
Using the SEER database, Lewin et al. demonstrated similar findings with decreasing OS in the presence of pLN disease (FIGO stage IIIC 1 = 57% [95% CI 54%–60%], FIGO stage IIIC2 = 49.4% [95% CI: 46%–53%] versus FIGO stage IA = 89.6% [95% CI: 89%–90%] and FIGO stage IB = 77.6% [95% CI: 76%–79%]). 6 The current study produced similar results using contemporary SEER data (FIGO stage IIIC1 = 71.4% and FIGO IIIC2 = 63.4%; p < 0.0001).
However, research shows that current methods of assessing nodal disease burden may not be completely accurate. Various multicenter studies have found that the LNR (ratio of number of pLNs to nLNs) was associated with worse PFS and OS. This parameter helps evaluate the burden of nodal disease and cancer spread, as well as the extent and quality of comprehensive lymphadenectomy. Researchers from Memorial Sloan–Kettering (New York, NY, USA) reported that patients with a tumor nodal burden of >10% had worse 5-year OS than patients with a ≤10% tumor nodal burden (LNR ≤10% = 79% OS versus LNR of 10%–50% = 60.6% versus LNR >50% = 35.8%; p < 0.001). 17
Similarly, MD Anderson (Houston, TX, USA) researchers found that patients receiving care at that center with at least 10 lymph nodes removed and with LNR >50% had PFS of 25.2 months, compared to LNR <50% (135.6 months; HR = 3.87; 95% CI: 1.15–13.04; p = 0.03). 7
Under the current FIGO staging system, pLN status is used for determining treatment plans. The number of pLNs is dependent on the number of rLNs. Therefore, it is prudent to consider the number of rLNs and nLNs when discussing adjuvant treatment planning and prognosis with patients. LODDS is a measure that reflects both rLNs and nLNs. LODDS has been utilized as an assessment tool for predicting prognoses in ovarian, cervical, and colorectal cancers,8–12 but its usefulness for EC had not been reported.
The present study investigated the prognostic value of LODDS in patients with FIGO stages IIIC and IV EC. The results demonstrated that a LODDS value ≥ −0.12707 was significantly and independently associated with poorer DSS (93.9, 75.9, and 67.5% [LODDS <0.12707] versus 78.6, 49.6, and 38.1% [LODDS ≥ −0.12707]; HR = 2.14; 95% CI: 1.85–2.47). Findings for OS were similar (Supplementary Table S3).
Although LODDS is a measure that requires complex calculations and is not as intuitive as LNR, LODDS strength lies in the ability to discriminate patients with equivalent LNRs. Sun et al., demonstrated the heterogeneity of LODDS even when the LNR was 0 or 1. 18 Additionally, when comparing various measures of lymph-node status (number of lymph nodes examined, number of pLNs, LNR, index of positive odds, and LODDS), LODDS was the strongest at predicting survival (Supplementary Figs. S1–S4, Supplementary Tables S1 and S2).
Utility of nodal disease-burden assessment
Assessing lymph node status for women with EC has been a controversial topic since the publication of GOG-33 [Gynecologic Oncology Group#33]. 19 Many researchers are hesitant to perform pelvic and para-aortic lymphadenectomies due to surgical complexity, 20 patient habitus and medical complexities, the inherent indolent biologic behavior of EC, and the potential for undue long-term morbidity. 21
To determine which patients would benefit from comprehensive surgical staging involving lymphadenectomy, the Mayo Clinic (Rochester, MN, USA) developed a triage protocol utilizing intraoperative frozen-section analysis of the uterus identifying intrauterine risk factors. 22 Although it is widely adopted, various studies have demonstrated that the methodology is inaccurate and nonreproducible; to keep the false–negative rate low, “a large number of patients with negative lymph nodes have to undergo a full lymphadenectomy.” 21
Adding to the complexity of the issue are the results of the CONSORT [Consolidated Standards of Reporting Trials] and ASTEC [A Study in the Treatment of Endometrial Cancer] randomized controlled trials. The trials revealed that surgical staging did not provide any survival benefits.23,24 These studies have also been criticized in the gynecologic oncology community about their experimental designs, study powering, baseline characteristic differences in study arms, and inadequacies of lymph-node dissections. 25 Additionally, patients who do not have lymphadenectomy lack pathologic information on lymph-nodes status. This deficiency leads to many patients requiring external beam radiation to conventional fields, areas of unknown disease extent, leading further to many patients subjected to undue radiation therapy and its sequelae.26–29
Use of LODDS with current LNS techniques
SLN sampling (SLNS) has been proposed as a middle ground between comprehensive lymphadenectomy and no lymphadenectomy, and is considered an acceptable method of staging by the National Comprehensive Cancer Network. 30 Evidence from the FIRES [Fluorescence Imaging for Robotic Endometrial SLN biopsy] trial, a multicenter prospective cohort study involving 18 clinical sites and 340 patients, revealed a SLN mapping technique that had a sensitivity for detecting metastatic disease of 97.2% (95% CI: 85.0–100) and a negative predictive value of 99.6% (95% CI: 97.9–100). These findings support the use of SLNS strongly for surgically staging patients with EC. 31 From a perioperative standpoint, SLNS has been shown to have other benefits, including lower incidences of leg lymphedema, 32 less surgical complexity, and shorter operative times compared to conventional lymphadenectomy.20,33
Although prospective data are lacking on survival outcomes for SLNS, there are reported data from retrospective studies. In a study of the National Cancer Database, Nasioudis et al. reported a non–statistically different 3-year OS rate of 83.0% versus 87.4% when comparing SLNS-only and conventional lymphadenectomy. They reported no difference in survival between conventional lymphadenectomy– and SLNS-only groups (HR = 1.39; 95% CI: 0.77–2.52). 34 Researchers from the Mayo Clinic confirmed these findings with a similar analysis. 35
Similarly, a study of two patient series from two United States academic centers compared a conventional systematic pelvic and para-aortic lymphadenectomy to a contemporary series of patients undergoing SLNS. The results showed no statistical differences in risk of disease progression (HR = 1.45; 95% CI: 0.74–2.85; p = 0.28) or death due to disease (HR = 2.18; 95% CI: 0.87–5.47; p = 0.10). 36 These findings support the utility of SLNS as part of surgical staging of EC with comparable outcomes to conventional lymphadenectomy. The utility of LODDS for women undergoing staging surgery for EC with use of SLNS is unknown.
Strengths and limitations
The current study had several strengths. The SEER database collects and publishes cancer incidence and survival data from 18 population-based cancer registries covering ∼48% of the U.S. population. SEER is also the only comprehensive database that includes stage of cancer at time of diagnosis and patient-survival data. The current study reported the findings of a large EC cohort. The data are generalizable, and representative of the U.S. population, because the data are is collected from cancer registries across United States.
Limitations of the study were attributable to the source data. Limitations include incompleteness and inaccuracies of individual-level data collected from source registries. Accuracy of lymph-node information may not be confirmed for each case, and missing lymph-node data may introduce biases. However, the impact is negligible.
Survival outcomes cannot be evaluated fully because the data do not distinguish the intention of therapy as either curative or palliative. Details on the types, doses, and durations of chemo- and radiation therapies, and the use of other treatments are not collected. When stratifying by FIGO stage, there was a relatively small sample size for patients with FIGO stage IVA disease. The last event for patients with high LODDS occurred at ∼10 months, and the curve remained flat as no further events occurred. This led to a statistically insignificant difference in outcomes between comparative groups. However, this result must be interpreted cautiously as the small sample size did not provide stable estimates. Finally, as with all retrospective studies, information and selection biases may affect comparisons.
Conclusions
When assessing lymph-node status, LODDS is a superior classification method for predicting survival DSS in patients with EC.
Footnotes
Acknowledgments
This article was previously published as a poster presentation: Smith C, Quan C, McDowell A, et al. The log odds of positive lymph nodes predicts survival of advanced stage endometrial cancer: A retrospective analysis of 3230 patients in the SEER database. Gynecol Oncol 2021;162 (suppl1):S301. †
Authors' Contributions
Dr. Smith was responsible for conceptualizing the study and writing the original draft of this article. Drs. Chen and Huang curated the data curation and performed formal analyses. Dr. Baldwin-Branch supervised the study, and all of the other authors wrote, reviewed, and edited, the final article.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
The authors did not receive financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.