
Abstract

A38
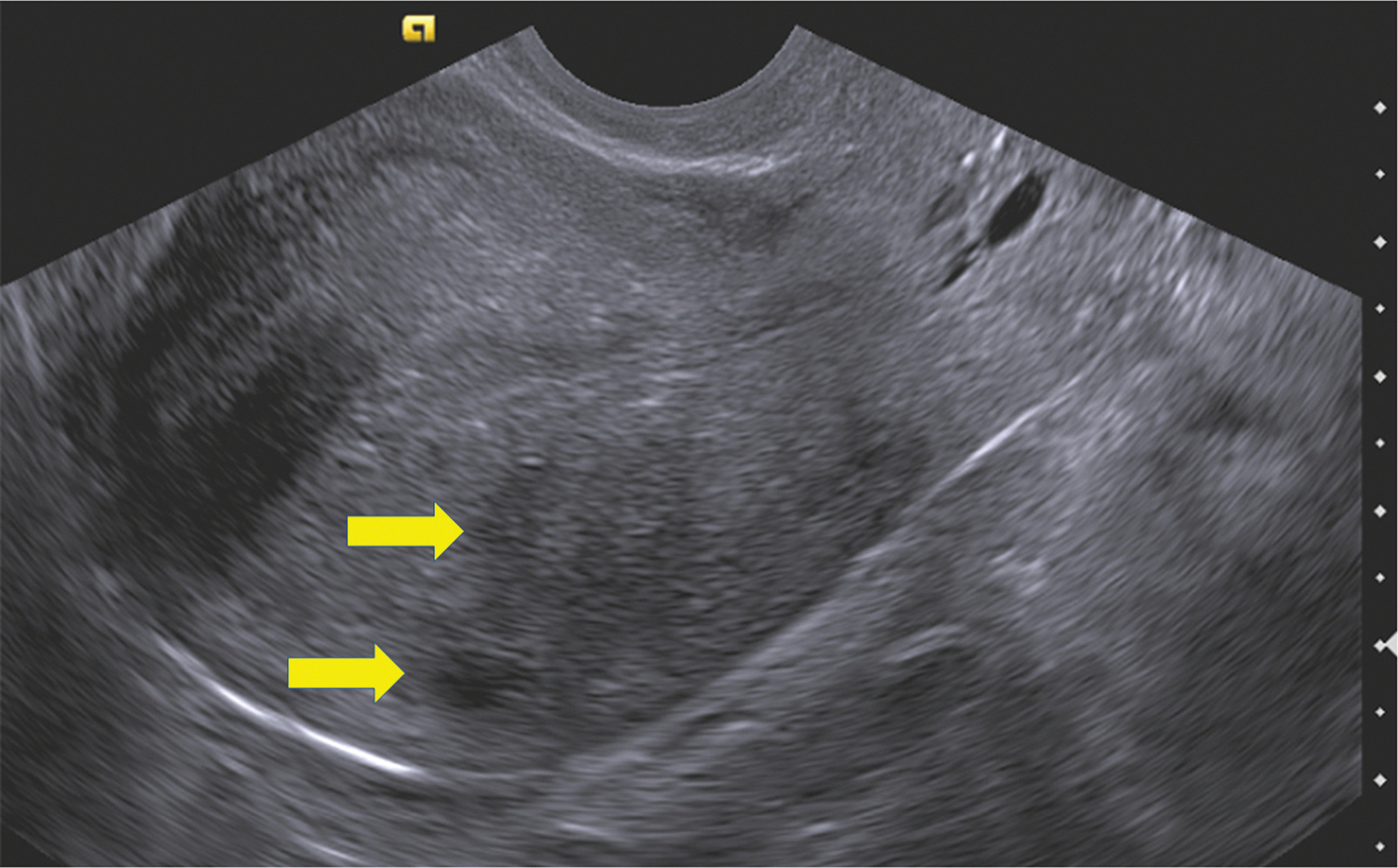
Transvaginal ultrasound. Note diffuse heterologous myometrium, indistinct endometrial-myometrial junction, and cystic areas in the myometrium (arrows). These ultrasonic findings are suggestive of adenomyosis.
At total laparoscopic hysterectomy, the uterus was bulky in appearance, but superficial and deep infiltrating endometriosis were not identified grossly. Cystic adenomyosis was identified on histologic sections of the uterus. The proximal fallopian tubes were thickened and contained multiple gray interlacing nodules contiguous with the uterus (Fig. 2). Histologically, the proximal fallopian-tube nodules had diffuse endometrial islands of variable sizes within hypertrophic tubal muscularis consistent with nodular adenomyosis (Fig. 3).
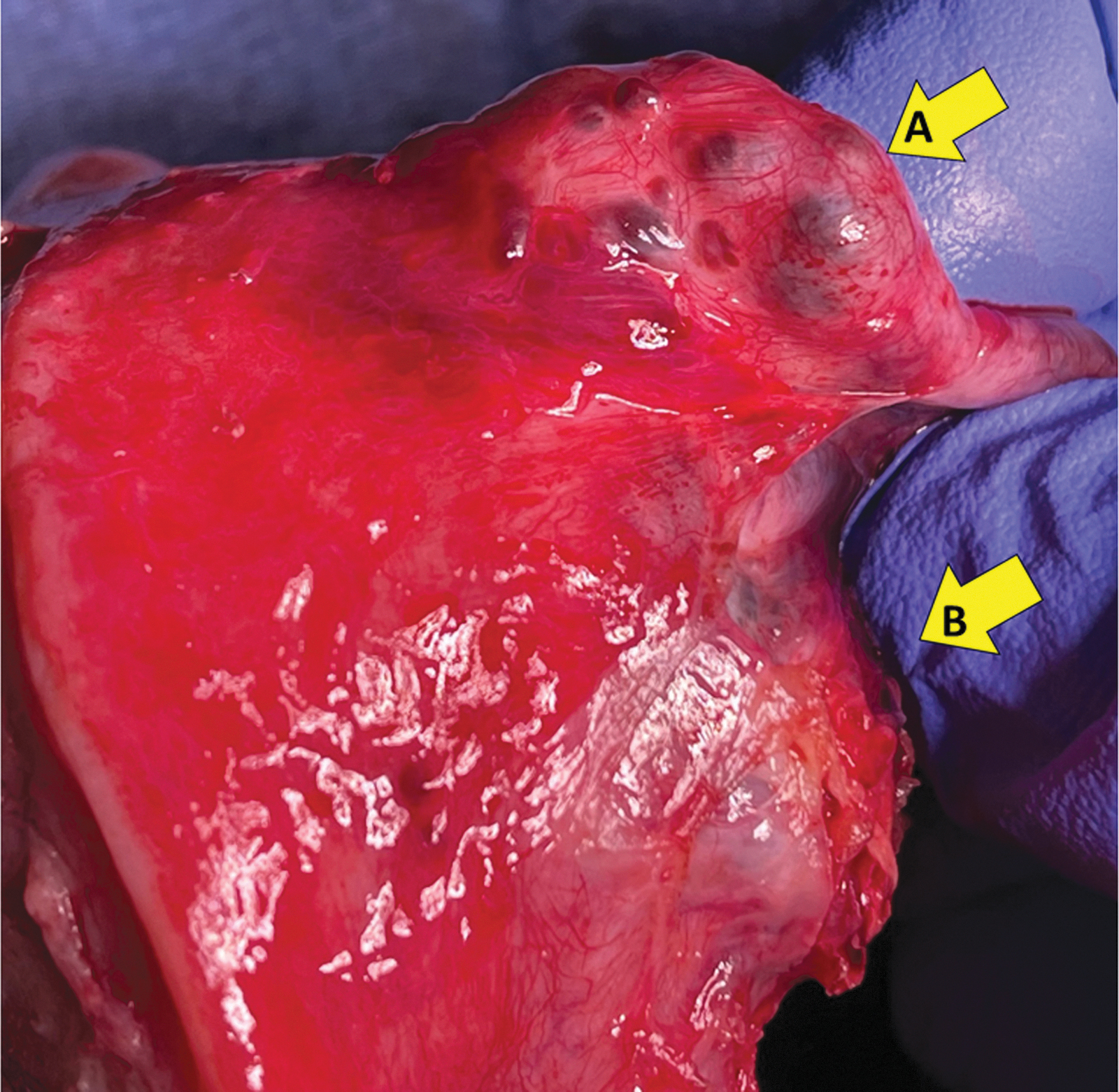
Gross surgical specimen with nodular adenomyosis of the right cornual and isthmic fallopian tube (arrow A) and cystic adenomyoma within the myometrium (arrow B).
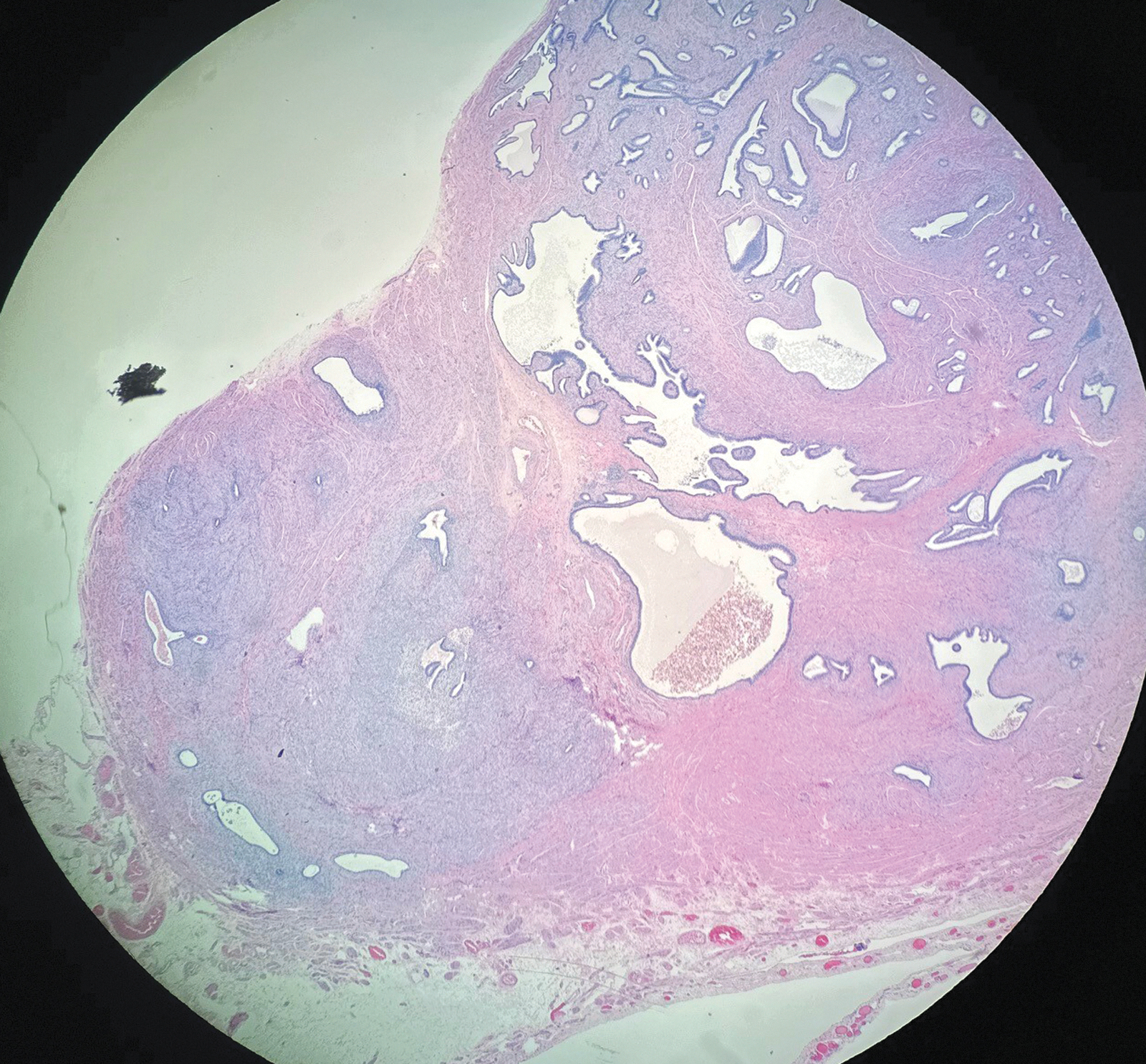
Histopathology of the proximal right fallopian tubal nodule showing multiple irregular islands of endometrial tissue and stroma within smooth muscle, consistent with a nodular adenomyoma.
Adenomyosis is a benign gynecologic condition characterized pathologically by islands of endometrial glands and stroma present within the myometrium. Clinically, adenomyosis is associated with pelvic pain, dysmenorrhea, dyspareunia, abnormal uterine bleeding, adverse pregnancy outcomes, gastrointestinal distress, dysuria, and infertility. Ultrasonography and magnetic resonance imaging have increased diagnostic acumen in establishing the diagnosis particularly for patients who desire conservative management.
Uterine smooth muscle is contiguous anatomically with the muscularis portion of the fallopian tube. Not uncommonly, scattered superficial endometriosis may be encountered on the fallopian tubes, but descriptions of adenomyosis present in the fallopian tubes are rare.1–3
As the proximal fallopian tube smooth-muscle component is contiguous to the myometrium anatomically, migration of endometrial glands into proximal tubal smooth muscle is biologically plausible. The precise mechanism of migration of endometrial glands into myometrium in adenomyosis is understood incompletely, and several hypotheses have been suggested. 4 One hypothesis is that adenomyosis originates from focal extension of clonally unique endometrial glands that migrate into myometrium forming a labyrinthine network of invasion. Stromal cells may also migrate. 5 Via this mechanism, endometrial glands in the interstitial area of the uterus could migrate laterally into the contiguous proximal fallopian tube.
Dr. Kauffman performed the surgery and wrote the original draft of this article. Mr. Alfaro performed background research and reviewed and edited the article.