
Abstract
Abstract
Chronic postoperative pain (also known as chronic postsurgical pain) is pain that occurs post-surgery and extends beyond the tissue-healing process, lasting for at least 3 months. Risk factors for the development of chronic postoperative pain include demographic/lifestyle, genetic, psychologic, and clinical factors (comorbidities, surgical factors, anesthesia/analgesia factors), as well as perioperative pain (preoperative and postoperative pain). In addition, there are several conditions that occur postoperatively leading to propagation of chronic postoperative pain, such as anterior cutaneous nerve entrapment, incisional neuromas, pudendal neuralgia, and ilioinguinal neuralgia. Clinicians should focus on identifying risk factors and mitigating them to decrease the incidence of chronic postoperative pain. (J GYNECOL SURG 39:262)
Introduction
Chronic postoperative pain (also known as chronic postsurgical pain) is pain that occurs post-surgery and extends beyond the tissue-healing process, lasting at least 3 months. 1 Chronic postsurgical pain was not formally defined until the current International Classification of Diseases, 11th Revision (ICD-11) was developed.1–3 Given this more-recent classification, a literature search reveals variations in how chronic postoperative pain is defined in terms of time course, with a range of 2–12 months.
Incidence
There is also a huge variation in the incidence of chronic postoperative pain that is reflective of the many risk factors that exist for the development of chronic postoperative pain. 1 A narrative review by Steyaert et al. quantified the frequency of subacute pain (defined as up to 3 months) after gynecologic surgery to be 17% and the frequency of chronic pain (defined as up to 12 months) after gynecologic surgery to be 15%–40%. 2 For gynecologic surgery, hysterectomy is the one of the most-common gynecologic operations; with annual rates of ∼5.6/1000 in the United States. 4 Given the prevalence of hysterectomy, it is one of the most-studied surgeries in gynecology and is the source of a significant amount of data on chronic postoperative pain post gynecologic surgery.
Risk Factors
Risk factors for the development of chronic postoperative pain are shown in Figure 1 and include demographic/lifestyle factors, genetic factors, psychologic factors, clinical factors (comorbidities, surgical factors, anesthesia/analgesia factors), and perioperative pain (preoperative and postoperative pain). 1
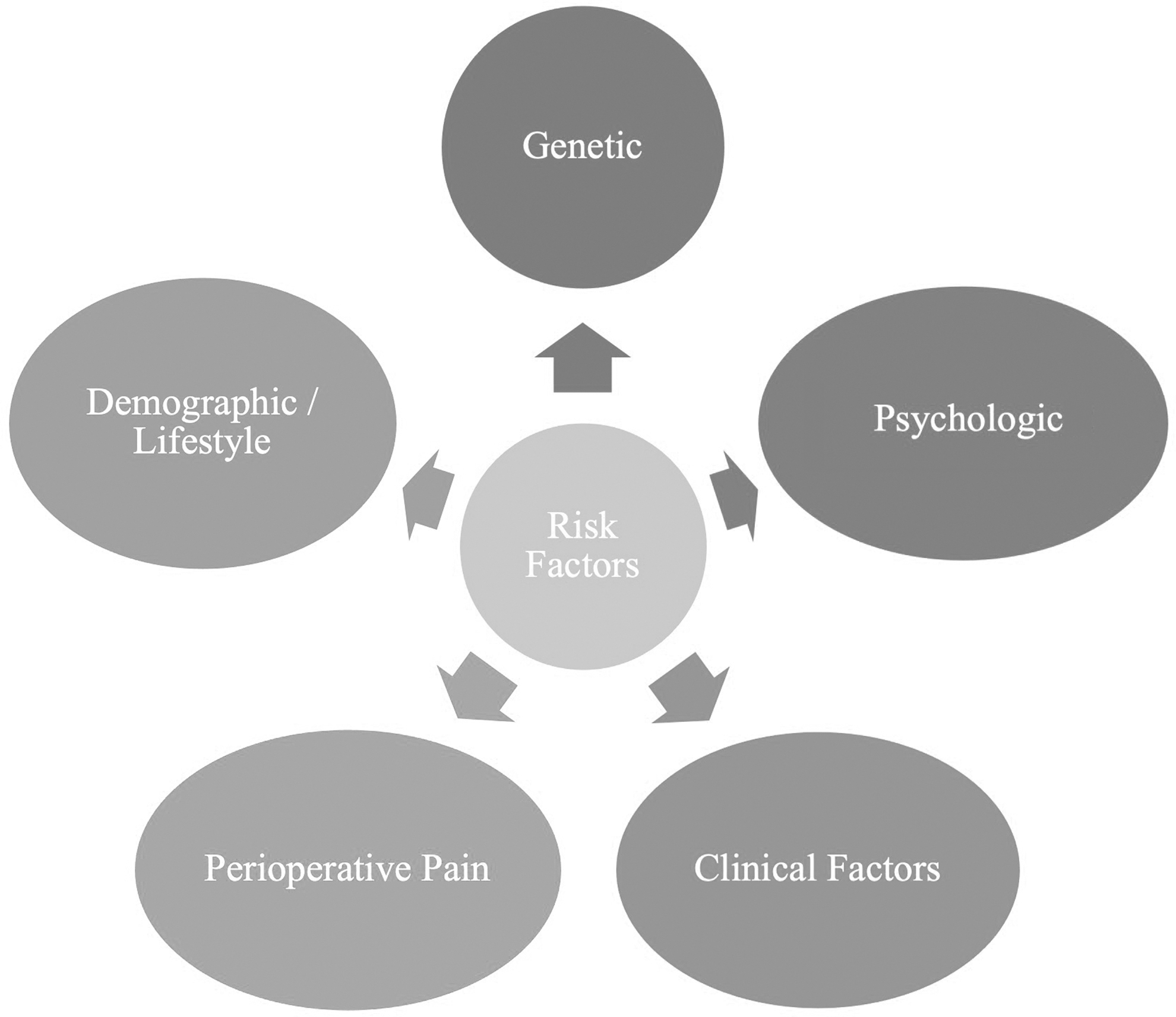
Risk factors for chronic postoperative pain.
Demographic and lifestyle factors include female sex, young adult age, low education level, low socioeconomic status, and smoking.1,5
Genetic predisposition has been an increasing field of research, pursued to identify which genetic factors play roles in chronic pain. 5 Genetic factors include genetic mutations and polymorphisms affecting various receptors, enzymes, and channels such as catechol-ortho-methyl transferase and precursor of μ-protein receptor. 1
Factors affecting psychologic vulnerability include catastrophizing, anxiety, depression, and post-traumatic stress.1,5 In addition, the nocebo effect (a negative effect due to negative expectations) has become an increasingly frequent phenomenon. 5 Patients with negative expectations of pain had increased postoperative pain scores on questionnaires. 5
Types of clinical factors
Clinical factors are subdivided into comorbidities, surgical factors, and anesthesia/analgesia factors.1,5
Comorbidities
These include conditions such as fibromyalgia, irritable bowel syndrome, rheumatoid arthritis, and peripheral neuropathy among others.1,5
Surgical factors
These include surgical technique (laparoscopic versus open), duration of procedure, extent of nerve/tissue injury, and surgical complications. 1 A higher occurrence of persistent pain 4 months after surgery was seen with hysterectomy via Pfannenstiel or vertical incision than with hysterectomy via laparoscopic or vaginal route. 5 It is important to note that this prior statement compared abdominal hysterectomy to vaginal hysterectomy not specifically correlating between the incision types used for abdominal hysterectomy. 6 The incidence of neuropathic pain after abdominal and pelvic procedures varies between 13.5% and 30%. 5 Most neuropathies are mild and self-limited; however, some are severe or long lasting, requiring intervention.7,8
A single-center retrospective case series of patients undergoing benign gynecologic surgery (N = 2449) found that 3.2% of the patients developed postoperative neuropathy. 7 Most neuropathies were sensory only (80.8%) and most resolved over time (complete resolution was noted in 75.6% of the study patients and persistent, but reduced, neuropathy was noted in 16.7% of these patients). 7 Of the 3.2% of the patients who experienced postoperative neuropathy, 35.9% developed chronic postoperative neuropathic pain (symptoms >3 months). 7 Most cases of postoperative neuropathy after gynecologic surgery are unspecified but other frequently seen neuropathies are femoral, common peroneal, lateral femoral cutaneous, ilioinguinal/iliohypogastric, and genitofemoral. 8
Anesthesia and analgesia-related factors
These include use of general versus regional techniques and specific adjunct medication usage. 1 The type of analgesic strategy used changes the transmission of pain, ideally causing beneficial changes in central pain processing. 5
A randomized, placebo-controlled double-blinded study was published in 2022. 9 The study compared dexmedetomidine or lidocaine infusion to placebo for preventing chronic postoperative pain and neuropathic pain after open gynecologic surgery. Dexmedetomidine reduced pain scores significantly, compared to placebo at three months, and lidocaine was superior to placebo for preventing development of neuropathic pain at six months after gynecologic surgery. 9
An equally interesting topic centers around epidural analgesia and if it improves rates of chronic postoperative pain. Although many reports note the benefit of regional anesthesia, such as epidurals, specifically in the acute postoperative time, epidural analgesia has not been shown to reduce the prevalence of chronic postsurgical pain in gynecologic surgery.5,6
Types of perioperative pain
Perioperative pain factors include preexisting preoperative, intensity of pain, and acute postoperative pain. 1
Preexisting preoperative pain
Preoperative pain can be at the surgical site or any other part of the body and has the highest correlation with chronic postoperative pain, based on length of presence and intensity.1,5 Preoperative abdominopelvic pain tripled the odds of persistent pain in patients undergoing hysterectomy. 5 Interestingly, pain itself can be an indication for a hysterectomy. 4 The subset of patients with preoperative pain as an indication for surgery are at a higher risk of developing chronic postoperative pain. 4
Pain intensity
With increasing levels of pain, the probability of preoperative opioid use increases, which, in turn, is related to a higher risk of chronic postsurgical pain after gynecologic surgery. 5
Acute postoperative pain
Among the many risk factors for the development of chronic postoperative pain, one of the most-studied modifiable risk factors is acute postoperative pain.6,10 The severity of acute postoperative pain, particularly during the first 5 postoperative days (and possibly even within the first 48 hours) is highly predictive of chronic postoperative pain. 1 Given the importance of controlling acute pain, many enhanced recovery after surgery protocols have been developed. 10 These protocols are designed to prevent acute postoperative pain and its progression to chronic postoperative pain by using preemptive and multimodal analgesia. 6 Preemptive analgesia helps blunt the excitability of dorsal-horn neurons that occurs from surgical stimuli, thereby reducing postoperative hyperalgesia. 6
Interventional Pain Management
Several conditions are known to occur postoperatively, leading to the development of chronic postoperative pain. Pain management physicians who are aware of these conditions can help patients relieve their pain, and improve their quality of life (QoL). Some of these conditions include anterior cutaneous-nerve entrapment (ACNES), incisional neuromas , pudendal neuralgia, and ilioinguinal neuralgia etc. In a retrospective chart review of 1210 patients undergoing major pelvic surgery, the incidence of postoperative neuropathy was ∼1.9%. 11
ACNES
This is a phenomenon in which neuropathic pain is sensed due to impingement along the anterior cutaneous nerves, branches of the intercostal nerves, typically as they perforate the rectus fascia and run along the lateral border.12,13 Patients present with abdominal pain, with a point of maximal tenderness along the lateral rectus sheath border, typically unilateral in presentation. 12 Diagnosis is made based on history and a physical examination while ruling out other causes of abdominal pain. Physical examination findings include a positive Carnett's sign—when a physician presses on the point of maximal tenderness and the patient is asked to raise the head/lift the shoulders, which increases the pain sensed. 12 Treatment includes local anesthetic nerve blocks (used for diagnoses and for therapy); radiofrequency ablations, if there is a need to extend relief; and neurectomy, if the condition is refractory. 13
Pudendal neuralgia
Pudendal neuralgia is defined as neuropathic pain along the pudendal nerve territory; in women, this includes the vulva, vagina, clitoris, perineum, and rectum; in men, it includes the glans penis, scrotum, perineum, and rectum.14,15 Pain is usually worsened by sitting and can be associated with sexual and bladder symptoms. 15 There are many causes of pudendal neuralgia, including mechanical, infectious, and immunologic. 14 Most causes of postsurgical-related pudendal neuralgia are mechanical in nature, related to scar tissue, pelvic-floor muscle spasm, or pressure from surrounding structures. 14 Treatment includes medications, physical therapy, pudendal nerve blocks, sacral neuromodulation, and surgical decompression.14,15
Ilioinguinal neuralgia
This is a cause of neuropathic pain along the lower abdomen, upper thigh, and pelvis (labia majora and mons pubis in women and penis root and anterior scrotum in males).16,17 The nerve originates from the anterior rami of T12 and L1 but runs a long course that makes it susceptible to injury. 17 Surgical trauma has been documented in inguinal-hernia repair, hysterectomy, appendectomy, laparoscopic abdominal surgery with traumatic trocar placements, abdominoplasty, and orchiectomy. 16 Treatment includes medications, rehabilitation (myofascial release, acupuncture, or transcutaneous nerve stimulation), nerve blocks, radiofrequency ablations, or surgical neurectomy. 16
Conclusions
Chronic postoperative pain is an important clinical problem that affects function and QoL. 9 Despite having information related to the etiology and risk factors for chronic postoperative pain, there is no concrete way to stop the development of this kind of pain. Clinicians should focus on identifying risk factors and mitigating them to decrease the incidence of chronic postoperative pain. In addition, if a patient develops certain postoperative pain conditions, such as ilioinguinal neuralgia, once a proper diagnosis has been made a comprehensive treatment plan can be developed.
Footnotes
Authors' Contributions
Drs. Ackerman and Ibañez conceptualized, wrote, reviewed, and edited this article.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this article.