
Abstract
Background:
Enhanced recovery after surgery (ERAS) became a widely adapted and introduced concept of multimodal pain control. However, this idea was not standardized and left room for exploration of a variety of different analgesic modalities. One such modality is the bilateral quadratus lumborum (QL) catheter block that was introduced in 2018 but is not yet been fully studied in the gynecological oncology population.
Objective:
Authors hypothesized that use of these catheters would help with pain management and decrease opioid consumption in the postoperative period.
Methods:
A retrospective chart review was conducted from 2018 to 2020 looking at patients with known gynecological malignancy who underwent an exploratory laparotomy. Groups who had the QL block were compared with those without the block. Primary outcome was opioid consumption measured in morphine milligram equivalents (MME). Secondary outcomes looked at opioid consumption analyzed by adjuvants used in the block, length until ambulation, and length of stay in the hospital.
Results:
Authors found that the results showed no difference on MME used on postoperative day (POD) 1 (p = 0.704), POD2 (p = 0.562), and POD3 (p =0.749, or combined over the 3 days (p = 0.597). Secondary outcomes also showed no difference: length to ambulation (p = 0.704), length of stay (p = 0.912), and QL adjuvant epinephrine (p = 1.0) and dexamethasone (p = 1.0). Results suggest that a variety of confounders may have influenced statistical significance when providers notice a clinical difference in pain control in patients who have a QL block.
Conclusions:
This study provides the first step in understanding pain control with blocks and paves the way for a future trial.
Introduction
Enhanced recovery after surgery (ERAS) is an evidence-based, multimodal pathway designed to optimize postoperative management by decreasing morbidity associated with surgery and reducing the length of hospital stay.1,2 The ERAS pathway includes preoperative measures (patient education, elimination of prolonged fasting period, nausea/vomiting prophylaxis, etc.), intraoperative measures (maintenance of normothermia, multimodal pain management, regional anesthesia, etc.), and postoperative measures (early mobilization, early Foley catheter removal, etc.).1,2
The ERAS pathway has been adapted for gynecological oncology patients and many studies have confirmed its promising effect on length of stay (LOS), postoperative pain, and postoperative opioid use.3–5 Despite this, components of the ERAS are yet to be standardly implemented, both nationally and institutionally. One important component that does not yet have standardized implementation is regional anesthesia and multimodal pain management as part of the intraoperative and postoperative pain control cascade.
The 2019 ERAS Society Recommendations note that a variety of regional analgesic techniques could be used, such as neuraxial (e.g., epidural, spinal) blocks, peripheral nerve blocks, and wound infiltration, particularly in combination with nonopioid analgesics (e.g., non-steroidal anti-inflammatory drugs, acetaminophen). Such multimodal pain management regimens allow for more rapid recovery and reduction of opioid administration, the latter of which poses increasing concern considering the growing opioid epidemic. 6 However, the report did not provide specific evidence to distinguish efficacy of different anesthetic techniques. More robust research is needed to better understand combinations and doses of different multimodal pain management methods and agents. 7
Generally, in laparotomy, thoracic epidural anesthesia (TEA) has been considered standard of care by most enhanced recovery pathways (ERPs). 1 However, complications caused by TEA can often disrupt other components of the ERPs. Over the last 10 years, fascial plane blocks such as transversus abdominis plane (TAP) blocks and, more recently, quadratus lumborum (QL) block catheters have gained popularity due to their more favorable safety profile compared with neuraxial techniques. 8 Very little data exist studying such techniques in open laparotomy for gynecological surgery.
Given the limited information and evidence in using QL block catheters among gynecological oncology patients and the clinical evidence that potentially QL blocks led to better pain control, we hypothesized that QL blocks would also lead to decreased opioid consumption in the immediate postoperative period.
Methods
Institutional review board approval was initially obtained. A retrospective study of gynecological oncology patients undergoing exploratory laparotomy during 2018–2020 was performed at an academic medical center. Any patient who was younger than 18 years, did not have a gynecological malignancy, did not undergo exploratory laparotomy, or had neuraxial anesthesia or a different type of pain block other than QL was excluded. Of note, all QL blocks placed were bilateral and an anterolateral (QL1) approach was used for placement. A Research Electronic Data Capture (REDCap) tool was created assessing demographics, postoperative pain scores, frequency and duration of narcotic use in the hospital, LOS in the hospital, and readmission rates for pain management. These parameters were compared with a historical patient cohort. Primary outcome measure was the amount of opioid used measured in morphine milligram equivalents (MME). Secondary outcomes included length to ambulation, length of hospitalization, and differences in MME use based on QL block adjuvants.
Statistical analysis
Analyses were reported as frequencies and percentages for categorical data, and means and standard deviations for continuous data. Differences between groups were reported using independent t-tests for continuous data, and chi-square or Fisher’s exact test for categorical data. Subset analyses were conducted using univariate and multivariable linear regression models. Analyses were conducted using R version 4.2.1; all tests were two-tailed and p < 0.05 was considered significant.
Results
Initially, 565 charts were pulled for analysis based on Current Procedural Terminology codes for review. Of these, 259 charts met the inclusion criteria. With regard to demographics, average age of participants was 60 years (range: 19–93), majority of the participants were Caucasian (86%), and the most common diagnosis was both metastatic uterine and ovarian cancer (20% each).
There were two groups that were compared: patients who received the bilateral QL block and those who did not receive the block. Of the total participants, bilateral QL block was administered to 116 patients (45%). Of note, the study did attempt to establish if this block was administered preoperatively or postoperatively. In this cohort analysis, 100 patients (86%) received the block preoperatively and 16 patients received it postoperatively (14%). Furthermore, adjuvants that were placed into the block such as epinephrine and dexamethasone were also analyzed to assess if there was an effect on pain by proxy of opioid use. See Table 1 for demographic data.
Patient Demographics
Represents significant p value.
With regard to the primary outcome, results showed no difference on MME used on post-operative day (POD) 1 (p = 0.704), POD2 (p = 0.562), POD3 (p = 0.749, or combined over the 3 days (p = 0.597). See Figure 1. Secondary outcomes also showed no difference: length to ambulation (p = 0.704), LOS (p = 0.912), and QL adjuvant epinephrine (p = 1.0) and dexamethasone (p = 1.0). See Figure 2.
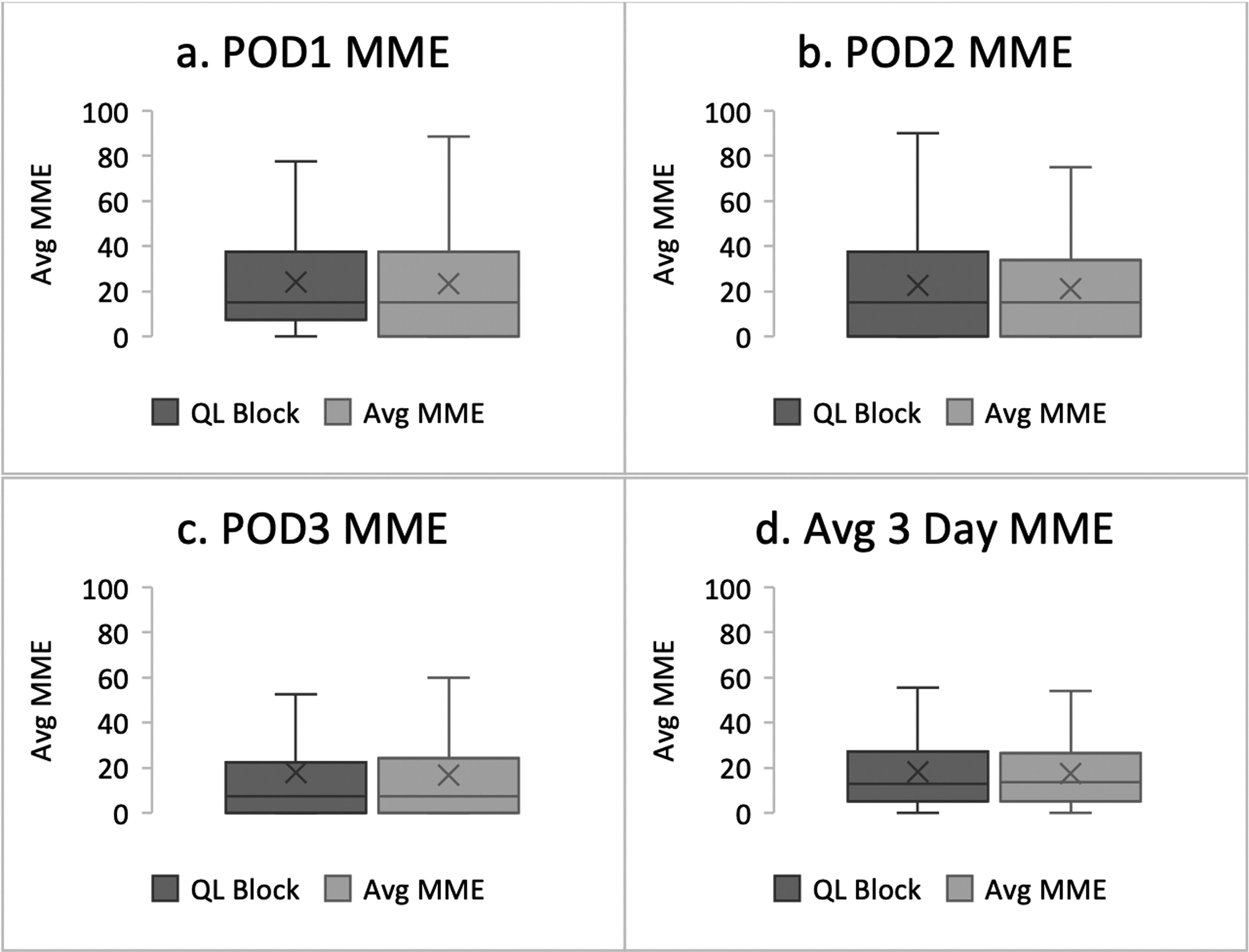
MME use on postoperative days 1–3.
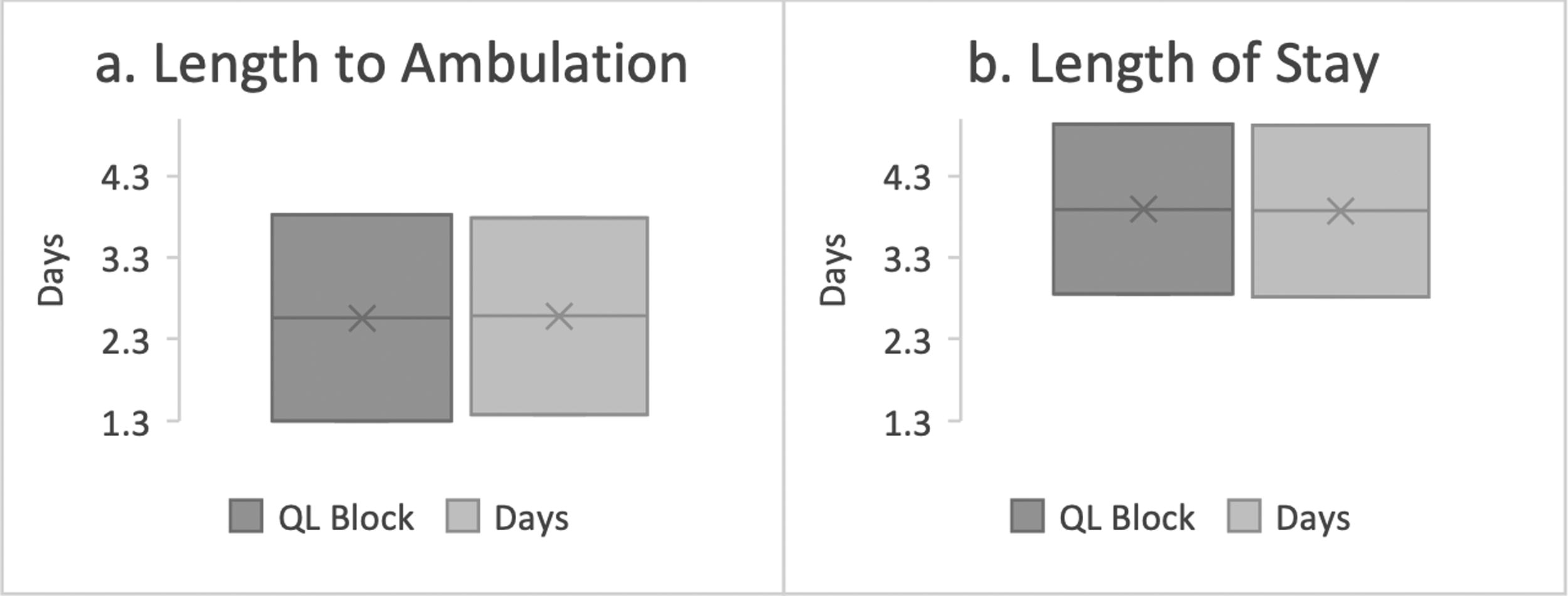
Secondary outcomes affected by QL block versus no block.
These results were further stratified by cancer type. However, due to a small number of patients for certain cancers such as cervical, metastatic cervical, fallopian tube, peritoneal, metastatic peritoneal, or vulvar/vaginal cancer, subtype analysis could not be run. For all others, results showed no difference in MME. See Table 2.
QL Block Outcomes by Cancer Type
Post hoc power analysis showed the following: POD1 at 6%, POD2 at 8%, POD3 at 6%, and POD average at 8%.
Discussion
This retrospective analysis was the first to explicitly analyze the effects of bilateral QL blocks on opioid use in a cancer population undergoing laparotomy. Given that the primary outcome of postoperative opioid use as measured in MME showed no difference across all postoperative days, we reject our hypothesis that there may be reduction in amount of opioid due to bilateral QL block. Nonetheless, there are many caveats that should be taken into account as an explanation of these results.
First, these results suggest that we should explore how opioids are administered in the hospital setting. Presumably, there is a bias in opioid administration as order sets often place these medications as pro re nata or PRN, suggesting that these are not scheduled medications, requiring patients to rate their pain scores in a certain way or to request them explicitly. Patients could subconsciously feel that because they have cancer and underwent a large surgery, they feel the need to ask for opioids. Furthermore, because of patients having to ask for medications, their pain could also be less controlled by the time the medication is administered, thereby requiring even more narcotics for additional pain control throughout the day. This could be alleviated if pain medications were on a more scheduled regimen and if patients felt their pain was adequately controlled, they could reject administration of medication and use less narcotics overall.
With regard to the QL catheters themselves, due to limitations in documentation, it was unable to be assessed when the catheters were removed. Hypothetically, there may have been patients who had the block removed due to it becoming dislodged or another error causing the catheters to not work properly. If these catheters were removed early in the postoperative course, POD1 for example, it can also explain why the catheter group showed no difference in opioids consumed overall. In this light, no data were tracked regarding if re-bolusing of the medications in the QL catheter was needed. These limitations could also explain the no difference in opioid use seen as the primary outcome as investigators were unable to account for how many of the QL catheters were actually working appropriately, how often patients were pressing their infusion buttons, and if re-bolusing was needed and unrecognized, causing patients to consume more opioids than otherwise may have been needed.
Furthermore, there is no established local anesthetic dose that infuses from the QL catheter itself. These doses are based on body weight of the patient and have established upper limits of safety beyond which dosing could be toxic. Majority of the patients (65) in this study were dosed 30 cc 0.5% ropivacaine. The most common body mass index (BMI) range was 26–30 for all groups (both block and no block). Nonetheless, 111 patients fell into the overweight category with a BMI of >30. All BMI groups were divided into range increments of 5, and therefore, this subset collectively represents a larger number of patients who were obese. It should be noted that the higher dose of local anesthetic 31–45cc 0.5% ropivacaine was used only in 12 patients, or 11.2% of the population. Presumably, this could too lead to pain-related issues requiring more narcotic use with the QL block group, leading to the results of this study.
Looking at the secondary outcomes showing no difference, one interesting aspect of this study is that it elicited which QL block adjuvants were used and how often. Authors found that epinephrine was used as an adjuvant in 21 blocks and dexamethasone was used in 36 pain blocks. These adjuvants are typically used to extend the effects of the local anesthetics and are not standardized for routine use for catheters but are routinely used for single shot blocks.9,10 As such, it could be thought that the catheters may become dislodged or had a chance to be misplaced as to why the block team added on these adjuvants preemptively such that if nothing else, the patient at least received a shot block. Given that investigators were unable to assess which catheter blocks may have failed, this is another area that sheds light on the efficacy of the blocks in this study population.
Yet another caveat that should be taken into consideration is intraoperative pain medication administration. Currently there is no standardized method of establishing pain intraoperatively. Anesthesiologists rely primarily on vital sign changes and their interpretation of changes as it relates to pain or other intraoperative events. It is thought that intraoperative pain control works as presumptive analgesia and can prevent an inflammatory response that may further exacerbate pain postoperatively. 11 In our study, we did trend intraoperative pain medications and found that hydromorphone ≤ 1 mg, hydromorphone > 1 mg, and ketorolac 30 mg were significantly used overall but did not assess how these medications may have influenced opiate use given that our primary outcome was not significant. Theoretically, given that these medications are not given in a standardized method, it would be challenging to study, but authors recognize that giving these medications at our academic center routinely may influence the study results showing no difference in opioid consumption between the two groups.
We believe each of these factors could have influenced acceptance of the null hypothesis, especially with the study design being retrospective, limiting us to use an Electronic Medical Record (EMR) that was difficult to extract data from due to limited availability of data. Post hoc analysis revealed that the study was underpowered but if there was a difference, then the analysis of 259 patients should be able to reveal this difference. As such, we are not convinced from the results of this study.
Clinically, providers have seen an effect on pain control secondary to bilateral QL catheters that seems significant from a pain management perspective. As such, authors believe due to these confounders limiting the retrospective analysis, results of this study should be followed up with a prospective cohort study or a randomized controlled trial looking specifically at QL catheters versus no blocks and conducting an analysis that focuses on opioid use, duration of QL catheters remaining in place, re-bolusing rates, how often bilateral QL catheters became dislodged or were otherwise faulty, adjuvants used due to presumptive single-shot block in case catheters fail, and also intraoperative pain medications. Having a prospective cohort will help with data extraction in areas that may have confounded the study results presented here.
In addition, bilateral QL block catheters versus TAP blocks could also be compared in the future along with QL block and neuraxial analgesia effects on opioid consumption. This study paves the way for many future directions and though the results here were not statistically significant, we feel this was due to limitations in the study design, and as always, the gold standard for investigating whether bilateral QL blocks offer a clinical benefit in this patient population would be a prospective, double-blind, placebo-controlled trial.
There is much center to understand about pain and opioid consumption. The strengths of this study are that it is first of its kind to attempt to understand if this type of block has a meaningful effect on opioid use in light of the opioid pandemic. Furthermore, it is an initial analysis that could shed light on varying clinical practices of pain management with how the block is administered, intraoperative narcotic use, etc. that can influence how we think about opioid consumption in the postoperative setting. Finally, this study uses a large sample size and an interesting population—cancer patients—that often requires more opioid prescriptions than others due to cancer-related pain. Nonetheless, the results of the study are not what were anticipated, and this study revealed there are many more questions that are center to be answered.
Footnotes
Acknowledgments
The authors would like to thank Mr. Colin Das and Dr. David Bennett for their contribution to this research endeavor.
Precis
This is a retrospective study studying the effects of quadratus lumborum blocks on opioid consumption and suggests a need for a prospective clinical trial.
Author Contribution
Drs. Sadhvi Batra, Christa Nagel, and Jeffrey Hopcian were responsible for the study design, IRB approval, and REDCap tool creation. Dr. Batra and Ms. Ashley Cantu-Weinstein did the data collection and wrote the article. Dr. Sarah Delozier did the data analysis.
Author Disclosure Statement
There are no conflicts of interests among the authors. This publication was made possible through the support of the Clinical Research Center of University Hospitals Cleveland Medical Center (UHCMC) and the Case Western Reserve University Clinical and Translational Science Collaborative (CTSC) 4UL1TR000439. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of UHCMC or NIH.
Funding Information
There was no funding for this project.
Statement of Originality
This article is original and has not been presented at any conference or submitted to any other journal for publication.