
Abstract
Abstract
Shrestha, Promish, Buddha Basnyat, Thomas Kupper, Simone van der Giet. Cerebral venous sinus thrombosis at high altitude. High Alt. Med. Biol. 13:60–62.—Cerebral venous sinus thrombosis (CVST) is a rare but potentially life-threatening medical condition. We describe a case of a 47-year-old woman who presented with headache, speech defects, and visual disturbances, and was later diagnosed with cerebral venous sinus thrombosis. The article describes a possible risk of such thrombotic events with exposure to high altitude environment in patients with coagulation defects such as Factor V Leiden mutation. Besides, such neurological conditions can occur independent of altitude illness and need to be recognized as their management differs.
Introduction
Case Report
A 46-year-old German woman came to Nepal International Clinic in Kathmandu (elevation 1400 m) with complaints of loss of vision on the right side of her visual field for 3 days. She was returning from her trek up to an altitude of 5600 m in Kalapathar. When she descended to Namche (3400 m), she developed sudden headache, followed by inability to see things on her right side and difficulty speaking. Her symptoms of headache and speech impairment improved as she descended further to Lukla (2400 m), but the visual defect persisted. When she presented to the clinic, she had mild headache and visual impairment. She had not had any symptoms of acute mountain sickness such as headache, fatigue, nausea, or dizziness during her ascent. She was not taking any medications. She had no history of chronic disease such as diabetes or hypertension.
Her blood pressure was 110/80 mmHg; pulse 66/min and regular, oxygen saturation by pulse oximeter was 97% in room air at rest. She was well oriented to time, place, and person. Her pupils were bilaterally normal in size and reacted equally to light; extraocular movements were normal. Confrontation testing revealed right visual field narrowing. The remainder of her neurological evaluation was unremarkable.
An ophthalmological evaluation reported she had right upper quadrantanopia; magnetic resonance imaging (MRI) scan of the brain showed features consistent with hemorrhage in the left temporo-parieto-occipital region. Further blood work-up including prothrombin time/International Normalized Ratio, complete blood count, and liver function test were within normal limits. She was advised to be admitted to hospital for observation but she elected to fly back to her country for further investigation and management. She underwent further computed tomography (CT) scans, angiography, and coagulation studies. Initial CT scan in Germany also showed left temporo-parieto-occipital hemorrhage with surrounding edema (Fig. 1). A repeat CT scan after 2 weeks showed that the lesion was resolving (Fig. 2). She was diagnosed with cerebral venous sinus thrombosis with thrombophilia with heterozygous mutation of Factor V and decreased protein S levels. She was initially treated with subcutaneous injection of Enoxaparin (low molecular weight heparin) during her 15-day stay at the hospital. During the treatment period she showed gradual improvement of the field of vision and repeat CT scan showed resorption of the lesion. She was then advised to take oral phenprocoumon for up to a year.
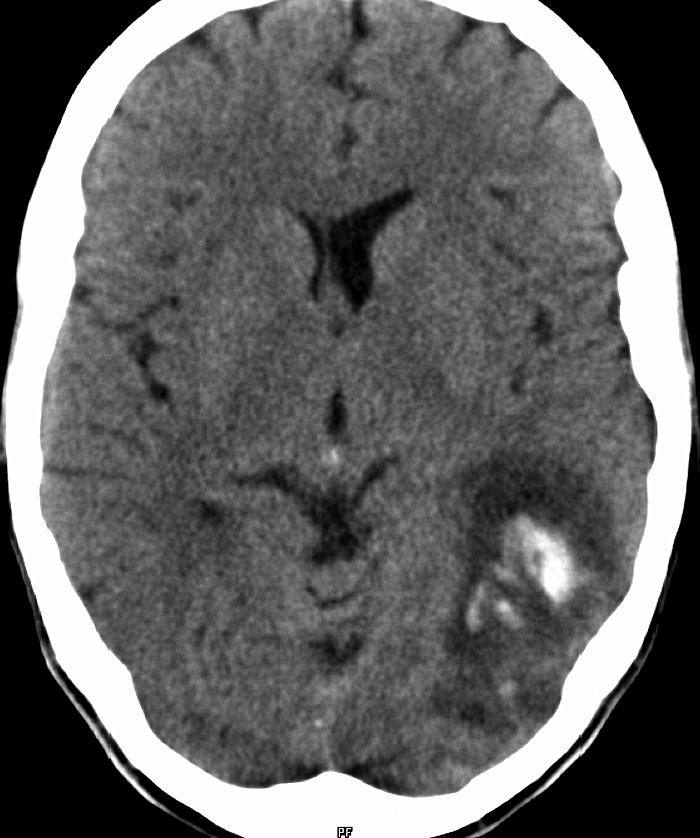
Left temporo-parieto-occipital hemorrhage with surrounding edema. 47×56 mm.
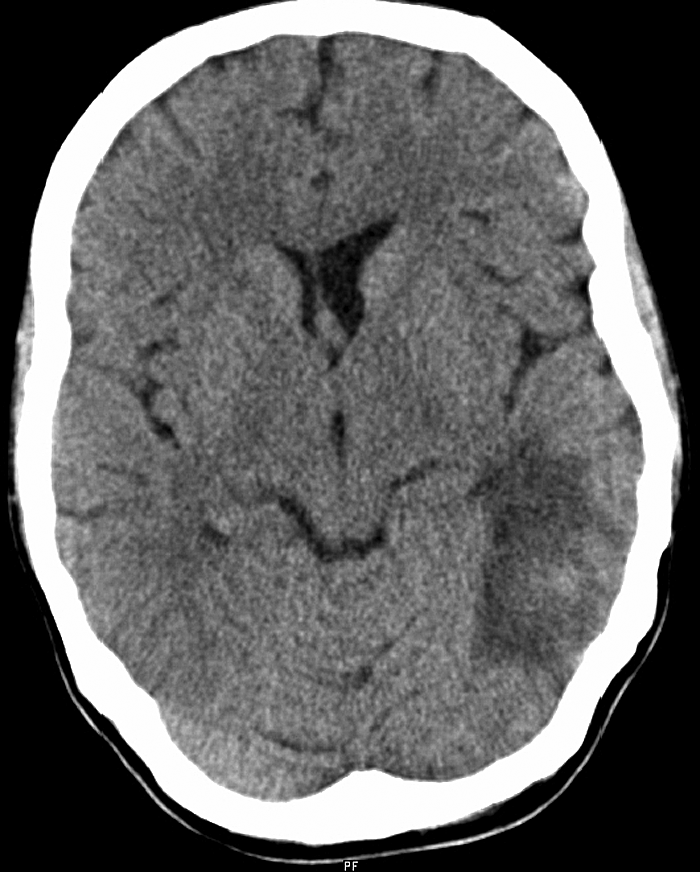
Resolution of the lesion compared to initial CT. 44×55 mm.
Discussion
CVST is an uncommon disease marked by clotting of blood in cerebral venous or dural sinuses, and in rare cases, cortical veins. Infection, neoplasm, pregnancy, puerperium, systemic diseases, intracranial tumors, oral contraceptive pills with concomitant tobacco use, and intrinsic coagulopathies are the risk factors to which CVST are often attributed (Saddatnia et al., 2009). In addition, dehydration, high altitude, and polycythemia in the absence of other factors, have also led to CVST (Chen et al., 2009; Fujimaki et al., 1986). Sagittal sinus thrombosis in a high altitude sojourner associated with protein C deficiency has been documented in the past (Boulos et al., 1999). A case of hereditary protein S deficiency presenting with CVST has also been reported (Nair et al., 2008). Our patient had a heterozygous mutation (G1691A) of Factor V, also known as Leiden mutation, and decreased level of protein S. Activated protein C along with protein S prevent clotting by inhibiting Factor V, Factor VIII, and tissue plasminogen activator (t-PA), hence, regulating fibrinolysis. A deficiency of protein C and/or protein S, thus, can lead to thrombosis. Also mutation in the gene for Factor V can prevent activated protein C from inactivating its respective factors and predisposing to thrombosis. Factor V Leiden mutation causing resistance to activated protein C is the most frequent cause of thromboembolism in Europe (Saddatnia et al., 2009). In the German population, heterozygous allele frequencies of 2.0%–3.6% have been reported (Saddatnia et al., 2009). CVST in individuals with heterozygous mutation of Factor V traveling to high altitude has not been previously documented. The acquired risk of thrombophilia at high altitude combined with congenital thrombophilic state of this patient possibly resulted in CVST. Other thrombotic events such as mesenteric, pulmonary, and retinal thrombosis have been documented from high altitude (Basnyat et al., 2001).
This case featured sudden onset of headache, speech disturbance, and right side visual defect. Her symptoms occurred at an altitude of about 3400 m when she was descending from altitude of about 5600 m. Altitude spectrum illnesses such as acute mountain sickness (AMS) and high altitude cerebral edema (HACE) present with a gradually progressive headache and global neurological signs rather than a focal deficit (Basnyat et al., 2004). Moreover, they occur during ascent, after some time at high altitude, not several days later when the patient has descended 2200 m. It was, therefore, highly unlikely that she had AMS or HACE.
A brain MRI of the patient done in Nepal showed a hemorrhage in the left temporo-parieto-occipital region (Fig. 3) which was the probable cause of the right-sided superior quadrantanopia. Further investigations in Germany diagnosed her with cerebral venous sinus thrombosis. CVST can present with focal neurological deficits due to cerebral venous infarcts which are frequently hemorrhagic (Ehtisham and Stern, 2006).
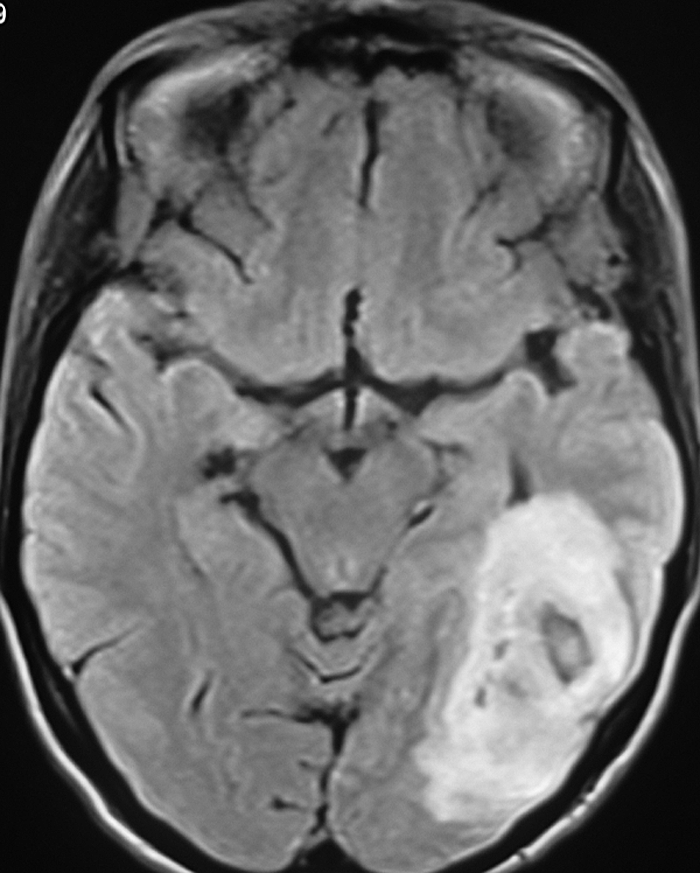
MRI showing left temporo-parieto-occipital hemorrhage. 50×63 mm.
It would be difficult to identify persons who can have thromboembolic events before they travel to high altitude. It is advisable that patients with such events in the past such as our case should not return to high altitude. Maintaining adequate hydration status is a preventive measure. Travelers to high altitude such as Kalapathar (5600 m) can get dehydrated because of lack of adequate water intake, as well as due to loss of fluid from vomiting caused by altitude illness. It can be worsened if the traveler has diarrhea. Patients with Factor V Leiden, if compounded by dehydration, may suffer from thrombosis. Hence, it is important to maintain adequate water intake and try to prevent and if necessary properly treat diarrhea at high altitude (Küpper et al., 2010). With the relative abundance of the Factor V Leiden mutation on one hand and the obviously extreme rareness of incidences like the one described above on the other hand, it is hard to make general recommendations for travel to high altitude. In general, it may be best to tell travelers to high altitude with known predisposing factors to thrombosis to take all the precautions to avoid altitude sickness and especially to drink adequate amounts of fluids (2 to 3 L of water per day); importantly, there are no evidence-based guidelines to make firm recommendations.
Conclusion
Neurological conditions such as CVST that fall outside the setting of routine altitude illness can occur independently without AMS or HACE (Basnyat et al., 2004). A diagnosis of CVST should be considered in patients with sudden headache and focal neurological defects at high altitude. A thorough history and physical exam is very important to differentiate these conditions. With this enhanced clinical awareness and the help of radiological techniques such as CT, MRI, and CT or MR angiography, CVST can be reliably diagnosed and properly managed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.