
Abstract
Abstract
Paal, Peter, Mario Milani, Douglas Brown, Jeff Boyd, and John Ellerton. Termination of Cardiopulmonary Resuscitation in Mountain Rescue. High Alt Med Biol. 13, 200–208, 2012.—The aim was to establish scientifically supported recommendations for termination of cardiopulmonary resuscitation (CPR) in mountain rescue, which can be applied by physicians and nonphysicians. A literature search was performed; the results and recommendations were discussed among the authors, and finally approved by the International Commission for Mountain Emergency Medicine (ICAR MEDCOM) in October 2011. 4166 abstracts were reviewed; of these, 96 were relevant for this article and are included in this literature review. In mountain rescue, CPR may be withheld or terminated in a patient with absent vital signs when the risk is unacceptable to the rescuer, the rescuer is exhausted or in extreme environments where CPR is not possible or any of the following apply: decapitation; truncal transection; whole body incinerated, decomposed, or frozen solid; avalanche victim in asystole with obstructed airway and burial time >35 min. Also, CPR may be terminated when all of the following criteria apply: unwitnessed loss of vital signs, no return of spontaneous circulation during 20 min of CPR, no shock advised at any time by AED or only asystole on ECG, and no hypothermia or other special circumstances warranting extended CPR. In situations where transport is not possible, mitigation of special circumstances is not possible, and further resuscitation is futile, CPR should be terminated. Medical directors of rescue teams should interpret these recommendations in the context of local conditions and laws, and create team-specific training and protocols for determining when to withhold and terminate CPR in a patient with absent vital signs.
Introduction
Methods
In 2009 the International Commission for Mountain Emergency Medicine (ICAR MEDCOM) established a working group for this topic. A literature search was performed in Medline by an investigator (PP) and restricted to research in humans. Articles were sought with the keywords “termination cardiopulmonary resuscitation” (114 articles), “primary cardiac arrest survival” (1379 articles), “trauma cardiac arrest survival” (799 articles), “hypothermia cardiac arrest survival” (1041 articles), “drowning cardiac arrest survival” (70 articles), “avalanche survival” (78 articles), “lightning survival” (93 articles), “electrocution survival” (77 articles), “burns cardiac arrest survival” (56 articles), “poisoning cardiac arrest survival” (132 articles), “auto resuscitation” (90 articles), and “resuscitation ethics survival” (247 articles); 4166 pertinent articles were found, excluding duplicates; the last access date was February 11, 2012. Abstracts of all articles were filtered for relevance; for relevant abstracts the whole article was retrieved for further reading. Additionally, reference lists of retrieved articles were hand searched for additional articles. 96 relevant articles were included in this review. Evidence and recommendations were reviewed at ICAR MEDCOM meetings during the fall of 2009 in Zermatt, Switzerland, the spring of 2010 in Laterns, Austria, the fall of 2010 in Stary Smocovec, Slovakia, and the spring of 2011 in Longyearben, Svalbard, Norway. Consensus was obtained, and the final manuscript was approved by the ICAR MEDCOM at the fall meeting 2011 in Are, Sweden.
General Aspects and Ethical Considerations
Resuscitation attempts in patients with sudden cardiac arrest are unsuccessful in 70%–98% of all in- and out-of-hospital cases and death will result (Lippert et al., 2010). Decisions regarding initiation and termination of CPR are challenging in individual cases (Lippert et al., 2010). Termination of CPR efforts may depend on several factors such as laws, policies and protocols, patient's age and medical history, mechanism and site of incident, and likelihood that resuscitation will be futile (Lockey, 2002; Farber et al., 2006; Rydvall et al., 2007; Rydvall et al., 2008; Grudzen et al., 2010; Millin et al., 2011). These factors may complement, but sometimes conflict with physician advice (Hall et al., 2004). In some situations where pre-hospital criteria for termination of CPR are inadequate, rescue personnel may need to use their judgement to determine whether CPR is reasonable or not (Ewy, 2006).
Death may be defined as the irreversible cessation of vital functions, including absence of circulation, spontaneous breathing, and whole-brain death when no confounding factors are present (Powner et al., 1996; Schlotzhauer et al., 2002). Nevertheless, diagnosing death's irreversibility in the field is not necessarily simple. A rescuer may declare a victim dead in the presence of some widely accepted conditions of death, or decide not to start CPR if the situation is unsafe (Table 1) (Boyd et al., 2010; Morrison et al., 2010a).
Historically, once CPR was started in a normothermic patient, many advocated that CPR should be performed for at least 20 minutes, and that CPR termination may be considered if asystole persists for longer than 20 minutes (Lockey, 2002; Baskett et al., 2005). More recently, clinical prediction rules for pre-hospital termination of basic life support (BLS) (Morrison et al., 2006; Ong et al., 2006) and advanced life support (ALS) (Morrison et al., 2009) for urban, nontraumatic, primary cardiac arrest have been validated. The BLS (Morrison et al., 2006) and ALS rules (Morrison et al., 2009) were re-validated for patients in urban centers by two separate research groups (Richman et al., 2008; Sasson et al., 2008). Recently, BLS and ALS rules (Morrison et al., 2006; Morrison et al., 2009) were also validated in patients with noncardiac causes of arrest, although patients with drowning or trauma were not included (Skrifvars et al., 2010). In the 2010 American Heart Association Resuscitation Guidelines, it is recommended that CPR should be continued until i) return of spontaneous circulation, ii) care is transferred to an ALS team, iii) rescuers are exhausted or CPR would jeopardize rescuers or others, or iv) reliable criteria of death are met, or v) criteria for termination of resuscitation are met (Morrison et al., 2010b).
These termination-of-resuscitation rules are promising, but they should be applied cautiously in mountain rescue since they have only been validated in urban areas. In mountainous and other wilderness areas the population, cardiac arrest circumstances, and survival may be different, creating the possibility for unexpected survivors (Gilbert et al., 2000; Oberhammer et al., 2008; Strapazzon et al., 2012). For example, mountain rescuers may encounter cardiac arrest caused by special circumstances such as avalanche, burns, drowning, hypothermia, poisoning or trauma, and these are discussed later in the article. Hence, any termination-of-resuscitation rule should be validated by mountain rescue services before widespread implementation.
With this caveat, we propose use of a modified BLS termination-of-resuscitation guideline to limit inappropriate CPR in mountain rescue. In a person with any unwitnessed loss of vital signs, all criteria have to be met to terminate CPR (Table 2). The termination of resuscitation in mountain rescue recommendations are more detailed than the urban ones, as they reflect CPR scenarios which may be associated with higher rates of special circumstances (e.g., hypothermia and avalanches) than in an urban environment. We have incorporated these components in a structured algorithm (Fig. 1) and propose this evidence-based framework principally to reduce unnecessary prolonged CPR while, however, promoting CPR where appropriate. This algorithm would be very useful for the large proportion of mountain rescue responders who are trained at least to BLS level and are adequately equipped (Brugger et al., 2005; Elsensohn et al., 2006; Barcella et al., 2010; Hohlrieder et al., 2010; McIntosh et al., 2010; Brugger et al., 2011).
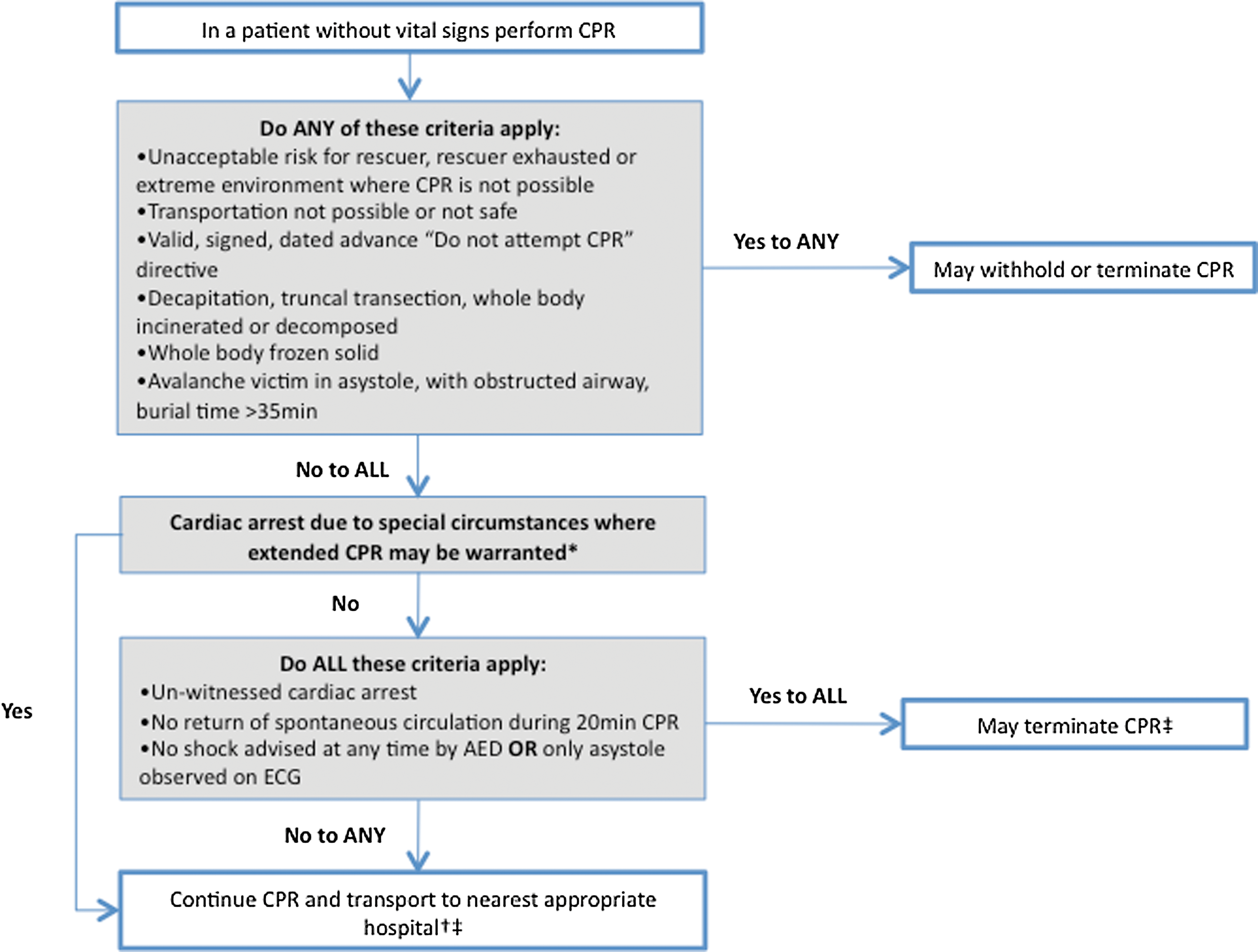
Algorithm for termination of CPR in mountain rescue.
AED denotes automated external defibrillator, CPR cardiopulmonary resuscitation, ECG electrocardiogram. 1 Clinical evidence of hypothermia, possibly confirmed by an esophageal temperature of less than 35°C if available.
Witnessed cardiac arrest, compared to unwitnessed arrest, has been shown to be significantly associated with greater return of spontaneous circulation in an urban pre-hospital study (OR 8.8; 95%CI=2.9–26.9) and therefore does not lend itself to a structured termination-of-resuscitation guideline (Verbeek et al., 2002). Therefore, with any witnessed cardiac arrest or, if one criterion is absent from the termination-of-resuscitation guideline (Table 2 and Fig. 1), CPR would best be continued unless a suitably qualified medical control provides a clinical assessment of the situation, patient, CPR, and transportation factors and determines that further CPR is futile. In contrast to the validated BLS rule, which stipulates that cardiac arrests witnessed by EMS be resuscitated (Morrison et al., 2006), this proposal for mountain rescue requires that CPR continues for arrests witnessed by bystanders also.
Prolonged CPR is not indicated when a patient is not expected to survive, consistent with the principle of medical futility (Morrison et al., 2010b; Soar et al., 2010), such as when rendered futile by patient condition as well as inadequate rescue resources or excessively long transports.
Primary Cardiac Arrest
About 50% of all hiking fatalities in the mountains suffer a sudden primary cardiac arrest (Burtscher et al., 2000; Burtscher et al., 2007), and sedentary men >40 years of age are at greatest risk (Ponchia et al., 2006). Survival declines at an average of 3% per minute after collapse (Gold, 2010). Mountain rescue teams should consider carrying an automated external defibrillator (AED) to improve outcome from primary cardiac arrest (Elsensohn et al., 2006; Barcella et al., 2010).
Environmental Limitations and Special Circumstances
In mountain rescue, outcomes from CPR may be worse than in an urban area due to limited personnel, equipment, environmental stresses, and longer extrication and transportation times. This trend towards worse outcome may be tempered by a somewhat healthier patient population compared with urban CPR studies. In addition, many instances of cardiac arrest occurring in the mountains may be classified as “cardiac arrest in special circumstances” (e.g., hypothermia), requiring modified criteria for termination of CPR (Soar et al., 2010; Vanden Hoek et al., 2010). For example, with hypothermia, drowning, lightning, and poisoning, prolonged CPR may be associated with a good outcome but in trauma or burns the prognosis very likely will be poor (Hopson et al., 2003; Mollberg et al., 2011).
Trauma
In one study from the mountain rescue service of Scotland, trauma accounted for ∼10% of all fatalities (Hearns, 2003). Trauma is also a frequent medical emergency in mountains in the United States (McIntosh et al., 2010; Rodway et al., 2011) and after avalanches (Hohlrieder et al., 2007) and crevasse accidents (Hohlrieder et al., 2010). Additionally, trauma in mountain areas is associated with a higher mortality rate when compared to urban areas because of longer transportation times associated with a higher risk of traumatic shock (Sumann et al., 2009). Severely traumatized patients should be assessed for lethal injuries, and if these injuries are absent, CPR should be commenced (Koster et al., 2010). In traumatic cardiac arrest, CPR in many cases is unsuccessful (Martin et al., 2002); however, when trauma is associated either with hypoxia, hypothermia, or electrical injury, survival rates increase (Pickens et al., 2005; Lockey et al., 2006; Willis et al., 2006). Cardiopulmonary resuscitation should be initiated in patients with clinical conditions, suggesting a nontraumatic initial cause of cardiac arrest (Hopson et al., 2003). Some suggest continuing CPR for at least 20 minutes in blunt trauma (Moriwaki et al., 2011), although it is not clear how those recommendations pertain to pre-hospital traumatic cardiopulmonary arrest. In the end, mountain rescuers should consider that one set of current guidelines for resuscitation of out-of-hospital traumatic cardiopulmonary arrest (Hopson et al., 2003) recommend termination of CPR after 15 minutes of unsuccessful resuscitation, and these guidelines have been supported by one large retrospective review (Mollberg et al., 2011).
Medical directors of mountain rescue teams should consider creating local protocols for termination of CPR in traumatic cardiac arrest bearing in mind that current guidelines also consider terminating CPR if the transport time is greater than 15 minutes (Hopson et al., 2003).
Hypothermia
Isolated hypothermia accounted for 4% of mountain deaths in one study from Scotland (Hearns, 2003). Diagnosis should be based on clinical and environmental presentation, classified according to the Swiss Classification (Durrer et al., 2003; Paal et al., 2006) and confirmed with core temperature measurement when available (Putzer et al., 2010). Even in cases of prolonged cardiopulmonary arrest, survival without neurological deficit may be possible if the patient was sufficiently cold before the onset of cardiac arrest (Gilbert et al., 2000; Oberhammer et al., 2008). In deeply hypothermic patients, survival with a good neurological outcome has been reported after as much as 6 hours and 30 minutes of CPR (Lexow, 1991). Patients have also been successfully resuscitated when part of their body is frozen (Moser et al., 2005). If, however, the whole body is frozen, the patient can be considered dead (Lloyd, 1996). For hypothermic patients in cardiac arrest or with cardiac instability, improved survival has been demonstrated with extracorporeal rewarming (ECR) (Walpoth et al., 1997; Gilbert et al., 2000; Ruttmann et al., 2007). In the absence of alternate causes of death, all nonfrozen, hypothermic patients without vital signs should be considered for CPR (Soar et al., 2010), and ideally transport should be to a center capable of ECR. In cases where time to ECR will be greater than 3 hours and 10 minutes (Husby 1990), no evidence exists to help choose between shorter transport to center without ECR or longer transport to an ECR center. Cardiopulmonary resuscitation should be continued until the patient is in the hospital and rewarmed to normothermia (Larach, 1995). Mechanical chest compression devices may be helpful with prolonged CPR (Lim et al., 2010).
Drowning
Worldwide every year, 150,000 die of drowning, making it the second leading cause of unintentional death (WHO, 2002a; Layon et al., 2009). Hypothermia, following cold water submersion, may be neuroprotective, thus survival even after prolonged submersion is possible (Harries, 2003). Several case reports have documented good outcomes in children receiving CPR (Ibsen et al., 2002), especially in those with cold water immersion (i.e., head out of the water) before submersion (i.e., head below the water); the documented record stands at 66 minutes submersion without neurological deficit (Bolte et al., 1988; Ibsen et al., 2002). Factors that are predictive for survival include witnessed short-lasting submersion and early resuscitation (Youn et al., 2009).
In many cases, drowning may be the result of another primary event, for instance arrhythmia, intoxication, seizure, stroke, or trauma (Modell, 1993). Thus, besides drowning, it is important to consider other potential reasons for cardiac arrest when making the decision to terminate CPR (Layon et al., 2009). A review has stated that if the water temperature is >6°C, survival is extremely unlikely if the patient is submerged for >30 minutes; if the water is <6°C, survival is extremely unlikely after >90 minutes of submersion (Tipton et al., 2011). Despite concerns over producing guidelines using minimal data, there is some support for using the above noted temperature and timing of submersion for termination of resuscitation decisions. The issue is further complicated because the time of immersion is usually known, but the time of submersion often is not. For these reasons it may be premature to use water temperature and timing to guide decisions regarding search and rescue effort or resuscitation (Perkins, 2011).
Avalanche
In North America and Europe, avalanches account for an average of ∼150 deaths per year (Brugger et al., 2001; Brugger et al., 2011). In a complete burial (at least the head and chest covered by snow) with an obstructed airway (e.g., packed with snow, no air pocket), asphyxia leads to death within 35 minutes. In the absence of life-threatening trauma, a buried patient with a patent airway will develop hypothermia, hypoxia, and hypercapnia, the so-called triple H-syndrome (Brugger et al., 2003). Hypoxia is the most common cause of death, followed by trauma (McIntosh et al., 2007). Trauma mortality was reported to be 24% overall in a study of 204 avalanche fatalities, although this rate varied considerably between activity groups (Boyd et al., 2009). Two other studies from different regions, of 56 and 36 fatalities, respectively, have demonstrated lower rates of trauma mortality (McIntosh et al., 2007; Hohlrieder et al., 2007). Hypothermia may be neuroprotective and survival with a good neurological outcome after prolonged burial and even cardiac arrest is possible (Oberhammer et al., 2008; Putzer et al., 2010).
In the absence of trauma incompatible with life, all avalanche patients buried for less than 35 minutes should be resuscitated according to current BLS and ALS guidelines (Berg et al., 2010; Deakin et al., 2010; Koster et al., 2010; Morrison et al., 2010a; Neumar et al., 2010). With burial time exceeding 35 minutes, absent vital signs and a patent airway, CPR should be performed and the patient should be transported to an ECR center as per the hypothermia guideline noted above. With burial time exceeding 35 minutes, asystolic cardiac arrest and an obstructed airway, CPR may be terminated (Brugger et al., 2001; Boyd et al., 2010; Vanden Hoek et al., 2010).
Lightning
In the United States of America, ∼100 persons a year die from lightning (Koumbourlis, 2002). Lightning has a mortality rate 5 to 10 times higher than other forms of electrical injuries. For example, in the Italian mountains 0.2% of persons rescued were hit by lightning and the mortality rate was 24% (CNSAS, 2002–2008). Unconscious patients with linear or feathering burns should be considered as lightning victims (Zafren et al., 2005). Explosive force may result in blunt trauma (Cherington, 1995), and burns or trauma may be life-threatening (Cooper, 1980; Koumbourlis, 2002; Ritenour et al., 2008), requiring rapid evacuation. A patient with a lightning injury should be assessed and, if indicated, CPR performed for at least 20 minutes (Zafren et al., 2005; Nelson et al., 2007). Death from lightning may result from primary respiratory arrest, followed by hypoxia and secondary cardiac arrest (Zafren et al., 2005). Thus, rescuers should be aware that with lightning, some patients may be nonbreathing but may have cardiac activity and thus only require artificial ventilation. Lengthy periods of ventilation may be required before spontaneous respiration returns. In cases of persistent cardiac arrest despite 20 minutes of CPR, terminating CPR should be in accordance with Tables 1 and 2 and Figure 1.
Burns
Worldwide, fire-related burns are responsible for over 300,000 deaths annually (WHO, 2002b). A significant portion of these deaths are related to open flame cooking that is common in many mountain communities. Case reports have shown good outcomes in burn patients who required short durations of in-hospital CPR (Jeschke et al., 2000). Unfortunately, out-of-hospital cardiac arrest in burn patients is unlikely to result in survival to discharge or meaningful neurologic function. However, withholding or terminating CPR should be in accordance with Tables 1 and 2 and Figure 1.
Poisoning
Poisoning in the mountains may result from causes such as alcohol, carbon monoxide, herbicides, plant ingestion, or envenomation (Hampson et al., 2001; Boyd et al., 2007). When managing a potentially contaminated patient, special personal protective measures are of utmost importance to protect the rescuer from toxic exposure until the patient has been adequately decontaminated. Case reports exist of patients with cardiac toxins surviving to good outcome after prolonged (i.e., >20 min) CPR (Durward et al., 2003). Therefore, be prepared to continue CPR for a prolonged period, particularly in young patients, as poison may be metabolized during life support measures (Soar et al., 2010). In poisoned patients, consultation with a poison control center should be considered before discontinuing CPR.
Further Considerations
Dangerous terrain necessitating delayed assessment
In some instances, assessing the victim on site is too dangerous (Samuel, 2008). In such circumstances, consider first evacuating and then assessing the patient when the environment is deemed safe. Declaring a victim dead on site without a complete assessment may be premature (Adhiyaman et al., 2007; Krarup et al., 2010; Braun et al., 2011).
Prolonged transport scenarios
If the risk of performing CPR is acceptable but a rescuer is in doubt about the likely outcome of a patient, then CPR should be performed continuously until arrival at an appropriate hospital, care is transferred to a higher level provider, or instruction to terminate CPR is given by a suitably qualified medical control. Mechanical chest compression devices can maintain good quality CPR and may assist in difficult evacuations or long transports (Nolan et al., 2010), although a systematic review found insufficient evidence of benefit or harm to recommend their widespread use (Brooks et al., 2011).
Legal issues
Medical leaders of rescue teams should interpret these guidelines in the context of their own local conditions and create team-specific training and guidelines for determining when to withhold and when to terminate CPR. The appropriate type of physician oversight will also vary and may include onsite, online (telephone or radio), and/or offline (protocols or guidelines along with training and quality assurance programs). Separate from the decision to start or stop CPR is the need for informing the responsible authorities (e.g., police) and the certification of death in accordance with laws and EMS protocols (Bailey et al., 2000; Richman et al., 2008; Stratton et al., 2008; Morrison et al., 2009; Ruygrok et al., 2009). Customized CPR protocols and standard operating procedures may help assisting EMS in making the difficult decision to withhold and terminate CPR in mountainous and other wilderness environments.
Limitations
These recommendations are based in part on studies performed in urban areas and, due to paucitiy of pre-hospital data, some in-hospital studies. These recommendations should be applied cautiously and reviewed prospectively, as there may be unexpected survivors in mountain populations. These recommendations should not preclude performing or terminating CPR in individual circumstances. Also, these recommendations specifically do not address pediatric patients.
Conclusions
In mountain rescue, CPR may be withheld or terminated in a patient with absent vital signs when the risk is unacceptable to the rescuer, the rescuer is exhausted, or in extreme environments where CPR is not possible or any of the following apply: decapitation; truncal transection; whole body incinerated, decomposed or frozen solid; avalanche victim in asystolic cardiac arrest with obstructed airway and burial time >35 minutes. Also, CPR may be terminated when all of the following criteria apply: unwitnessed loss of vital signs, no return of spontaneous circulation during 20 min of CPR; no shock advised at any time by AED or only asystole confirmed on ECG, and no hypothermia or other special circumstances warranting extended CPR. In special circumstances where extended CPR is warranted, if transport to hospital is not possible, then the rescuer will ideally mitigate the special circumstance prior to terminating CPR. In situations where transport is not possible, mitigation of special circumstances is not possible and further resuscitation is futile, CPR should be terminated. Medical directors of rescue teams should interpret these recommendations in the context of their local conditions and create team-specific training and protocols for determining when to withhold and terminate CPR in a patient with absent vital signs. This process is separate from the possible need for medical certification of death in accordance with regional and national laws and compliance with requirements of investigatory legal agencies.
Footnotes
Acknowledgments
These recommendations have been discussed and approved by Gege Agazzi (Italy), Borislav Aleraj (Croatia), Marc Blancher (France), Jeff Boyd (Canada), Bruce Brink (Canada), Doug Brown (Canada), Hermann Brugger (Italy), Perolof Eduinsson (Sweden), John Ellerton (England), Fidel Elsensohn (Austria), Herbert Forster (Germany), Nicole Gantner-Vogt (Liechtenstein), Andrzod Gorka (Poland), Martin Ivanov (Bulgaria), Alex Kottmann (Switzerland), Volker Lischke (Germany), Mario Milani (Italy), Maria Mizuskovic (Montenegro), Jose R. Morandeira (Spain), Wokiech Moskal (Poland), Maria A. Nerin (Spain), Marie Nordgren (Sweden), Noriyoshi Ohashi (Japan), Einar Ornarnarsson (Iceland), Kazue Oshiro (Japan), Oliver Reisten (Switzerland), Erik Sandetrom (Sweden), Fredrik Sederkuist (Sweden), Sven Christjar Skiaa (Norway), Inigo Soteras (Spain), Giacomo Strapazzon (Italy), Oleg Tcholakov (Bulgaria), David Tingay (Australia), Iztok Tomazin (Slovenia), David Watson (Canada), Ken Zafren (USA), and Greg Zen-Ruffinen (Switzerland).
We are indebted to Steve Teale who initiated this review by introducing the draft manuscript “Diagnosis of death in the mountains.”
Author Disclosure Statement
No manufacturer supported this study financially or materially. The authors have no financial or personal interest nor obtain any grants nor hold any patents concerning the described devices.