
Abstract
Abstract
Boos, Christopher John, Adrian Mellor, John Paul O'Hara, Costas Tsakirides, and David Richard Woods. The effects of sex on cardiopulmonary responses to acute normobaric hypoxia. High Alt Med Biol. 17:108–115, 2016.—
Methods:
Fourteen young healthy adult Caucasian subjects were studied at sea-level rest and then after >150-minute exposure to acute normobaric hypoxia (NH) equivalent to 4800 m and again at sea-level rest at 2 hours post-NH exposure. Cardiac function, using transthoracic echocardiography, physiological variables, and Lake Louise Scores for acute mountain sickness (AMS) were collected.
Results:
All subjects completed the study, and there was an equal balance of men (n = 7) and women (n = 7) who were well matched for age (25.9 ± 3.2 vs. 27.3 ± 4.4; p = 0.51). NH exposure led to a significant increase in AMS scores and heart rate, as well as a fall in oxygen saturation, systolic blood pressure, and stroke volume. Stroke volumes and cardiac output were overall significantly higher in men than in women, and acute NH heart rate was higher in women (80.3 ± 10.2 vs. 69.7 ± 10.7/min; p < 0.05). NH led to a significant fall in the estimated left ventricular filling pressure (E/E′), an increase in the septal A′ and S′ and septal and lateral isovolumic contractile velocities (ICVs), and a fall in the E′A′S′ ratio. The mitral E, lateral ICV, and E′ velocities were all higher in men. Acute NH led to a significant increase in right ventricular systolic pressure and pulmonary vascular resistance. There was no interaction between NH exposure and sex for any parameters measured.
Conclusion:
Despite several baseline differences between men and women, the cardiopulmonary effects of acute NH are consistent between men and women.
Introduction
A
An area that has been barely explored is that of the effects of sex on cardiopulmonary adaptations to HA. It is already well known that men have larger cardiac chamber sizes, higher resting stroke volume, and cardiac output than women (Okura et al., 2009; Dalen et al., 2010; Daimon et al., 2011). There are some, although very limited, data to suggest that there may be sex-related differences in autonomic, vasodilatory, and physiological responses to hypoxia (Mortola et al., 1996; Ricart et al., 2008; Wadhwa et al., 2008; Lombardi et al., 2013; Casey et al., 2014; Patel et al., 2014).
To overcome some of the challenges of studying subjects at genuine terrestrial HA, a number of methods of HA simulation have been used, and these include hypobaric (reducing the partial pressure of oxygen in a depressurized chamber) and normobaric hypoxia (using either a low FiO2 chamber or mask) (Boos et al., 2013; Coppel et al., 2015). These simulation methods can accurately replicate the degree of hypoxia for a given altitude, while allowing for a more controlled environment for medical research than that afforded with studies at terrestrial HA (Coppel et al., 2015).
In this study, we aimed to explore the cardiopulmonary responses of men and women to acute normobaric hypoxia (NH) in humans to determine whether any sex-related differences occur.
Methods
Study population
This was a prospective observational study of 14 fit and healthy British military servicemen aged 22–35 years. This cohort consisted of seven men and seven women who were matched for age and ethnicity. All subjects were required to abstain from caffeine, alcohol, nonsteroidal anti-inflammatory drugs, and smoking for >12 hours before the study and from strenuous physical activity for 48 hours before the experiment. Health status was confirmed following a detailed health questionnaire, and all subjects were required to have a normal baseline echocardiogram to confirm suitability for inclusion. All the included women had not had a previous pregnancy.
Ethics
The study was approved by the Ministry of Defence Research and Medical Ethics Committee and conducted according to the standards of the Declaration of Helsinki. All subjects were required to provide written informed consent.
Study protocol
The detailed study flow is shown in Figure 1. All subjects were examined at rest under normal atmospheric oxygen conditions at near sea level (absolute altitude ∼113 m; Leeds Beckett University, Centre for Sports Performance, Leeds, UK), followed by a 3-hour continuous exposure in an NH chamber (TISS, Alton, United Kingdom, and Sporting Edge, Sherfield on Loddon, United Kingdom).
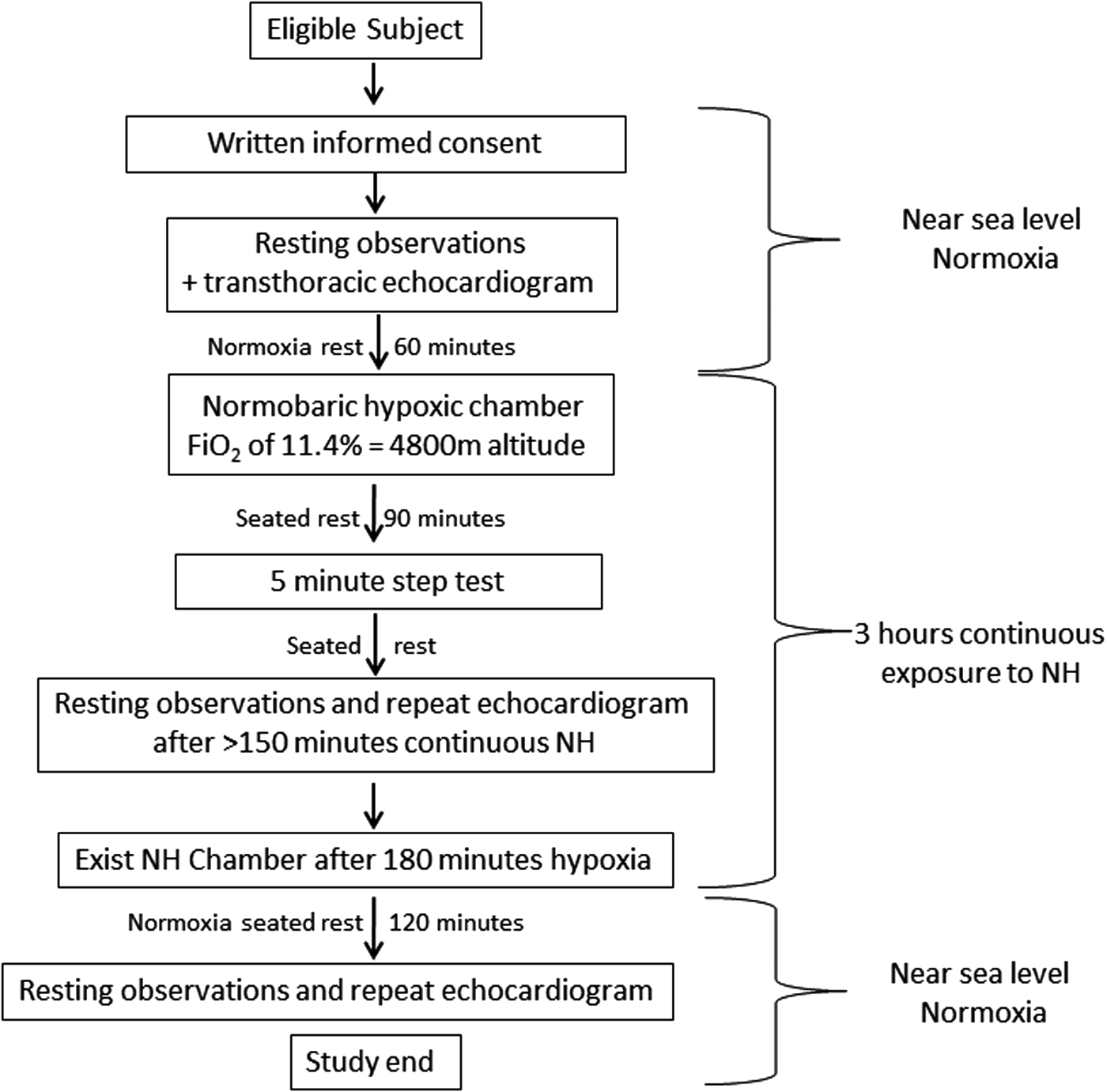
Experimental design flow diagram.
For NH exposure, the chamber was set to an FiO2 of 11.4%, approximating an altitude of 4800 m (Fig. 1). Participants were then required to complete physiological assessments (heart rate, blood pressure, and SpO2), a detailed transthoracic echocardiogram, and assessment of symptoms of acute mountain sickness (AMS). This was performed at rest 60 minutes before NH and then after 150 minutes to a 3-hour exposure to acute NH. All subjects underwent a 5-minute step test at 90 minutes. The chamber temperature was controlled at 21°C throughout the study. An additional echocardiogram was performed at rest in normoxia at 120 minutes post-NH exposure in all subjects.
Physiological measurements
Resting recordings of oxygen saturation (SpO2) were performed using a Nellcor N-20P Pulse Oximeter (Nellcor Puritan Bennett, Coventry, United Kingdom). Blood pressure was measured using an automated blood pressure cuff M6 (Omron Healthcare, Milton Keynes, United Kingdom), with the subject sat upright for >10 minutes at rest. Heart rate was obtained from a single-lead ECG obtained during the echocardiogram.
AMS scores
HA-related symptoms were assessed using the Lake Louise Score (LLS) twice (Hackett and Oelz, 1992; Roach et al., 1993). The LLS allocates a score of 0–3 (symptom not present to severe) for symptoms of AMS (headache, gastrointestinal symptoms, fatigue/weakness, dizzy/light-headedness, and difficulty sleeping). A total score of ≥3 in the presence of a headache is consistent with AMS and ≥6 with severe AMS.
Echocardiographic assessment
All echocardiographic assessments were undertaken using a portable Vivid Q echocardiogram machine (GE Healthcare™; Amersham, Bucks, United Kingdom) with a 1.5- to 3.6-MHz S4 transducer. All scans were performed by a single consultant cardiologist, with significant experience in echocardiography, and the data were exported for offline viewing and analysis using Xcelera package (Philips Healthcare, DA Best, The Netherlands). All subjects were scanned semisupine in the left lateral position at 30° head-up tilt. Pulsed-wave and two-dimensional color images were acquired in the parasternal short-axis and apical four-chamber view during a short end-expiration pause.
Stroke volume and cardiac output were calculated using the aortic systolic flow velocity integral, pulsed-wave profile of aortic blood flow from the apical five-chamber view, and the cross-sectional area of the left ventricular outflow tract (Boos et al., 2012, 2013, 2014; Huez et al., 2005). The cardiac index and the stroke volume index were calculated by dividing the cardiac output and stroke volume, respectively, by the surface area. Ejection fraction was calculated using the Simpson biplane method.
The pulsed-wave sample volume of the conventional Doppler was placed at the tips of the mitral and tricuspid valve leaflets to measure the peak early transvalvular flow velocity (E), the peak flow velocity (A) of late diastolic filling, and the E/A ratios (Paulus et al., 2007). Pulsed-wave TDI volume samples were recorded at the septal and lateral mitral annulus and used to calculate isovolumic contractile velocities (ICVs) and early (E′) and late diastolic (A′) and peak systolic (S′) long-axis velocities (Pavelescu et al., 2012; Boos et al., 2014).
The left ventricular EAS index, which is a measure of global cardiac function (E′/[A′ × S′]), was calculated using the TDI at the septal annulus as previously described (Boos et al., 2013). Estimation of LV filling pressure was undertaken from the ratio (E/E′) using the mitral valve E velocity divided by TDI-derived early annular filling E′ velocity at the averaged (septal and lateral) mitral annulus (Paulus et al., 2007). The left ventricular myocardial performance (Tei) index, another measure of global left ventricular function (IRT [isovolumic relaxation time] + ICT [isovolumic contractile time]/ejection time), was performed using TDI as previously described (Boos et al., 2013).
Right ventricular systolic pressure (RVSP) was estimated from the maximum velocity of the transtricuspid gradient using continuous-wave Doppler imaging. Pulsed-wave volume sampling at the level of the pulmonary valves was used to assess the pulmonary artery acceleration time.
The tricuspid annular plane systolic excursion, which is a marker of right ventricular long-axis systolic function, was recorded using M-mode echocardiography as previously described (Boos et al., 2013). The pulmonary artery vascular resistance (PVR) was calculated using the following equation: PVR = 80 × TRV/VTI RVOT, where TRV is the maximal tricuspid regurgitation velocity and VTI is the velocity time integral of the right ventricular outflow tract (RVOT) velocity measured using pulsed-wave Doppler at the level of the pulmonary valve in the parasternal short-axis view (Abbas et al., 2003).
Statistical methods and power calculations
Data were analyzed using SPSS® statistics version 22 (SPSS, Inc., Somers, NY). The Shapiro–Wilk test and inspection of the data were undertaken to assess normality of all continuous data. All data are presented as mean ± standard deviation. Unpaired two-group comparisons of continuous baseline data for men and women were performed using an unpaired T test and the Mann–Whitney test for parametric and nonparametric data, respectively. For categorical data, the Fisher's exact test was used.
The effects of sex on the time-dependent variables (effects of hypoxic exposure) were evaluated by two-way factorial repeated measures ANOVA. Time at baseline, ≥150 minutes of NH, and 120 minutes post-NH were included as levels of within-subjects factor (time effects of hypoxia) and sex (male or female) as between-subjects factors. The Bonferroni multiple comparison test was used when significant differences were found as well as interactions between the effects. A significance level of p < 0.05 was adopted.
There are no previously published studies that have assessed sex-related differences in cardiac function with acute hypoxia. Our sample size of 14 subjects was based on previously published work, which demonstrated significant changes in cardiac function and hemodynamic indices with acute hypobaric hypoxia with a sample size of 10–14 subjects (Boos et al., 2012, 2013).
Results
All subjects completed the study. Image quality was rated as good to excellent for all the echocardiographic scans. The average age of the 14 included subjects was 26.6 ± 3.8 (range: 21–33) years, with an equal balance of men (n = 7; 50%) and women (n = 7; 50%; Table 1). They weighed 72.5 ± 12.3 kg and were 171. ± 10.5 cm tall, with an average body mass index 24.6 ± 2.4 kg/m2. The men and women were well matched for age (p = 0.51) and were all Caucasians (Table 1). Four of the women were on oral contraceptive pill, which was a combined pill in three and progestogen only in one of the subjects.
Physiological and hemodynamic variables
The main effect of time and NH exposure was a significant increase in LLS and heart rate, as well as a fall in systolic blood pressure and stroke volume (Table 2). The main effect of sex was that stroke volumes and cardiac output were higher in men despite notably higher heart rates in women (80.3 ± 10.2 vs. 69.7 ± 10.7/min; p < 0.05) during NH. There was no observed interaction of time (altitude exposure) and sex. Hence, there was no sex-dependent effect of NH on measured variables. There was, however, a nonsignificant trend to higher SpO2 levels among women compared with men during hypoxia (p = 0.09; Table 2).
Significant (p < 0.05) differences between men and women.
Results of post hoc test: baseline versus 2.5 hours NH.
Results of post hoc test: NH versus 2 hours post-NH.
Changes in left ventricular function
NH led to a significant fall in mitral E velocity (main effect of time [hypoxic exposure], F = 10.1; p = 0.001) and the estimated left ventricular filling pressure (E/E′), an increase in the septal A′ and S′ and septal (main effect of hypoxic exposure, F = 11.9; p = 0.002) and lateral (main effect of hypoxic exposure, F = 9.2; p = 0.0007) ICVs, and a fall in the EAS ratio (Table 3). Mitral E velocity (main effect of sex, F = 8.1; p = 0.02) and lateral ICVs (main effect of sex, F = 5.3; p = 0.04) were overall significantly higher in women (Figs. 2 and 3), and lateral E′ velocities were higher in men (Table 3). There were no significant interactions with NH exposure and sex on any left ventricular functional parameters (p > 0.05; Table 3).
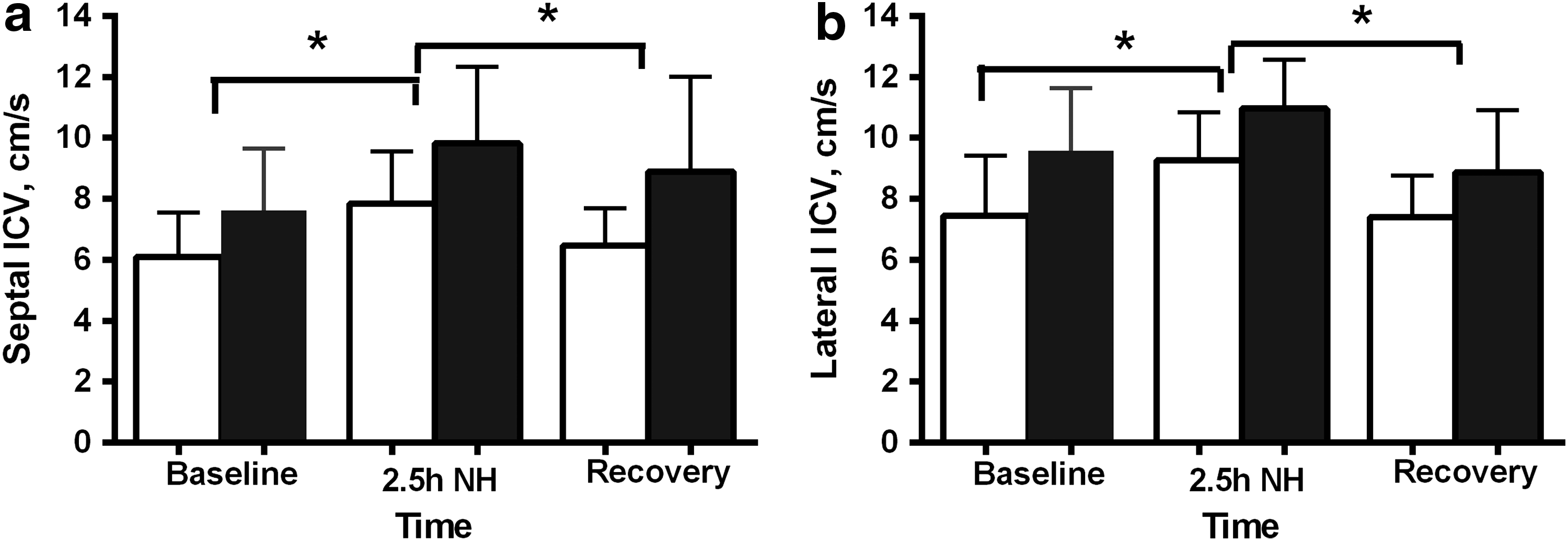
Changes in the left ventricular septal
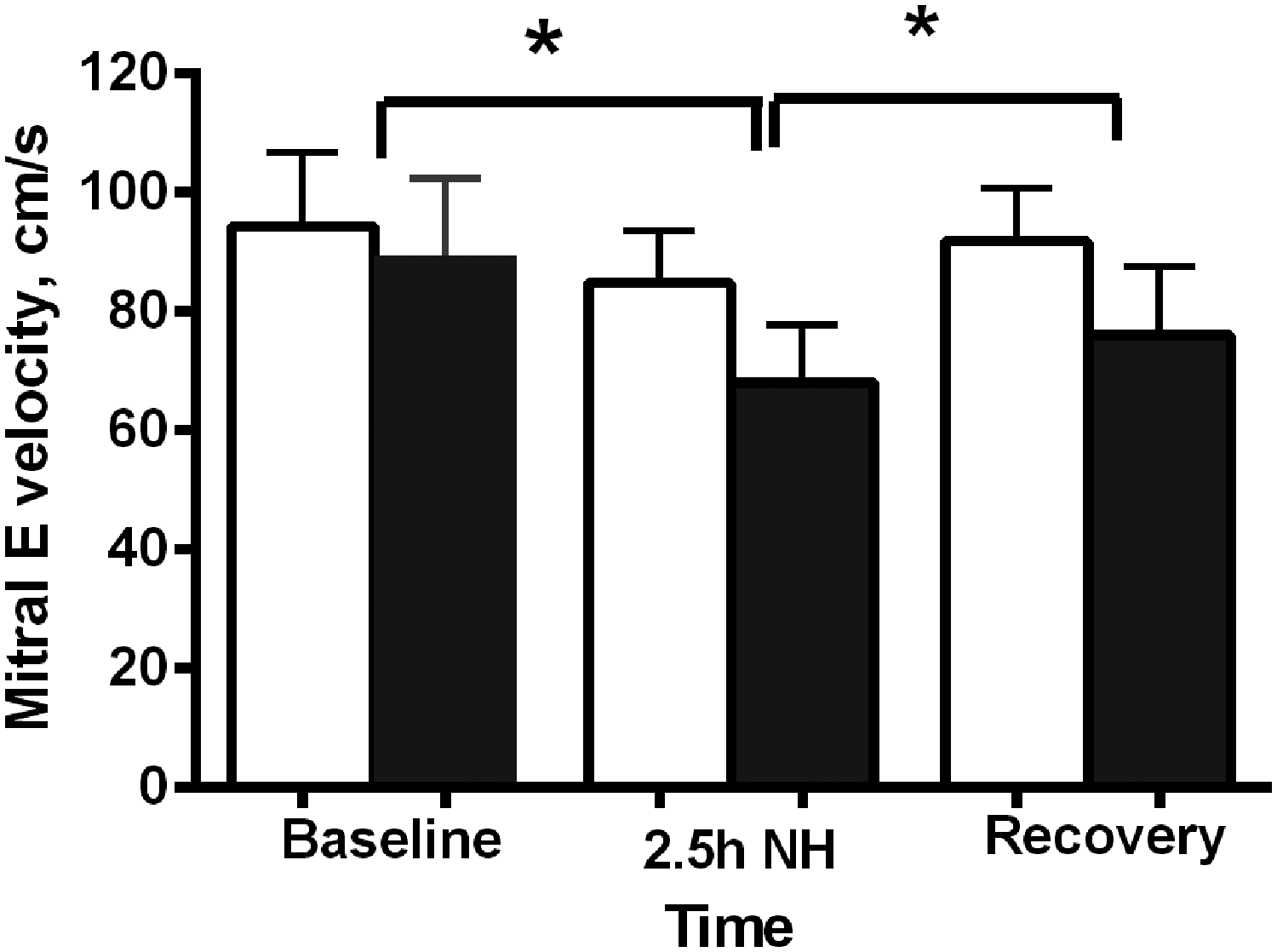
Changes in mitral E velocity with exposure to NH between women (white shade) and men (dark shade). *Significant on post-test.
Significant (p < 0.05) differences between men and women.
Results of post hoc test: baseline versus 2.5 hours NH.
Results of post hoc test: baseline versus 2 hours post-NH.
Results of post hoc test: NH versus 2 hours post-NH.
Right ventricular function and RVSP
Acute NH led to a significant fall in pulmonary artery acceleration time and an increase in RVSP and pulmonary vascular resistance without any main effects of sex or interactions of time and sex (Table 4).
Results of post hoc test: baseline versus 2.5 hours post-NH.
Results of post hoc test: baseline versus 2 hours post-NH.
Results of post hoc test: NH versus 2 hours post-NH.
TAPSE, transannular plane systolic excursion.
Discussion
To the authors' knowledge, this is the first study to assess the sex-related changes in biventricular cardiac function following acute hypoxia. The main finding of this study was that while cross-comparative differences in cardiac function exist between men and women at rest during normoxia, their responses to acute NH were consistent with the main effect of hypoxia. Hence, the cardiac functional responses to hypoxia are similar between men and women despite their recognized baseline differences.
Acute hypoxia leads to a number of well-recognized acute physiological and cardiac responses (Boos et al., 2012, 2013, 2014; Naeije, 2013). This study aimed to determine whether the additional stimulus of acute hypoxia leads to any specific sex-related differences. This is an important issue as HA exposure, whether as part of recreation or sport, is an interest shared by both men and women and as such could succumb to the complications of including AMS and high-altitude pulmonary edema (HAPE).
Differences in the incidence of AMS between men and women have been variably reported. There are published data to suggest that women may be more prone to AMS than men (McDevitt et al., 2014; Santantonio et al., 2014), but there are also contrary data to support the exact opposite (Beidleman et al., 2013). The data are similarly conflicting for HAPE, where variable sexual predominance has been reported (Sophocles et al., 1986; Hultgren et al., 1996). These reported differences may be explained in part by deficiencies in study design (unequal matching of men and women in numbers and age, etc.) and failure to adjust for important confounding factors known to influence AMS, such as the use of AMS prevention medicines, including acetazolamide, and sex-related differences in the altitude achieved.
We did notice that AMS scores were nonsignificantly yet nearly 50% higher during acute NH in men compared with women in our study, although this did not reach significance, lending some support to previously published work (Beidleman et al., 2013; Table 2).
Beyond the issue of AMS, there is evidence that cardiac adaptations may also be different between men and women. It is well established that cardiac chamber sizes, wall thickness, and mass are greater in men than in women and are influenced by age, degree of cardiovascular conditioning, ethnicity, and body habitus (e.g., height) (Okura et al., 2009; Dalen et al., 2010; Daimon et al., 2011). Observational studies have highlighted several sex-related differences in left ventricular systolic and diastolic function. These include higher resting mitral E and left ventricular E′ velocities in women (Daimon et al., 2011). Our baseline resting data are largely consistent with these published studies. Our data would suggest that the ICV is a very sensitive marker to both the effects of hypoxia, which led to a marked increase in ICV, and to sex, with notably higher lateral ICV and a trend to higher septal peak ICV in men over the time course of the study. It has been previously shown by our group and others (Huez et al., 2005; Boos et al., 2013) that in healthy young adults, the ICV increases with acute hypoxia, suggesting augmentation of systolic function, and that the ICV is higher at rest in men than in women with normoxia (Lind et al., 2006). This is, to the authors' knowledge, the first study to assess sex-related changes with acute NH. The left ventricular ICV has been shown to be a robust and validated noninvasive marker of global cardiac contractility and has the advantage over several other functional markers of being less load dependent (Lindqvist et al., 2007).
There are preliminary data to suggest that cardiopulmonary responses to hypoxia may be influenced by sex. In a very recent study of healthy young adults exposed to acute isocapnic hypoxia, it was observed that the increase in pulmonary artery systolic pressure was greater among women than men despite similar ventilatory responses (Fatemian et al., 2015). There are also data to show that with intermittent hypoxia, sympathovagal balance was enhanced, and parasympathetic nervous system activation was depressed in men but not in women despite, again, similar ventilatory responses (Wadhwa et al., 2008).
Plausible differences between men and women, if genuine, could relate to differences in sex hormones. Sex steroids have overlapping chemical and physiological properties with corticosteroids that are used to prevent and even treat AMS. Testosterone is a known pulmonary artery vasodilator and may have other properties, including immunomodulation, altering expression of cytokines, and potential antithrombotic actions (Smith et al., 2006). The phase of the menstrual cycle has been shown to affect physiological responses in women with attenuation of acute hypoxic pulmonary vasoconstriction in response to endogenous estrogens (Lahm et al., 2007; Pollard et al., 2007). The included women in our study were at differing phases of their menstrual cycle, and four were on oral contraceptive pill, which may be important confounding factors.
It is unknown whether differences in sex hormonal profiles could influence the efficiency of ventilation–perfusion within the lung and help explain the observed trend to higher SpO2 levels in women both at rest and during hypoxia in this study. This is an interesting finding that warrants further exploration in a larger field study at genuine HA. It has been previously shown that women have a slightly but significantly higher resting SpO2 than men, although the respective changes with hypoxia have been less well studied (Ricart et al., 2008). Indeed, there are recognized differences in red blood cell counts, hemoglobin, and 2,3-diphosphoglycerate plasma concentrations between women and men, which are additional factors to consider (Ricart et al., 2008).
We did not observe any significant differences in the pulmonary vascular responses between men and women, with both demonstrating similar increases in pulmonary vascular resistance and pulmonary artery systolic pressure and a fall in the pulmonary artery acceleration time with acute hypoxia as previously reported (Boos et al., 2012, 2013).
This study has a number of additional limitations, which need to be acknowledged. The sample size of this study was small, limiting the power to detect a potential significant difference in some of the echo parameters that might have been appreciated with a larger sample size. However, the study is strengthened by the two-way repeated measures design, and the two groups were very well matched for age and ethnicity. This study was performed under experimental NH and cannot necessarily equate to that which would occur with terrestrial HA, where the rate of ascent would likely be far slower and the environmental circumstances vastly different. The study cohort includes only young adults, and it is unknown whether sex differences might not be manifested until women are menopausal or postmenopausal. Finally, the degree of hypoxia was represented as moderate HA at ∼4800 m, and there were no cases of significant AMS.
Conclusion
The cardiopulmonary effects of acute NH are not influenced by underlying sex and are consistent with the recognized baseline differences between men and women.
Footnotes
Acknowledgments
The authors would like to thank the Drummond Foundation, Leeds Beckett University, the Centre for Aviation Medicine, the Defence Medical Services, and the Surgeon General's Department for their support.
Funding
Research reported in this study was supported by the Surgeon General, United Kingdom, and the Drummond Foundation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Defence Medical Services.
Author Disclosure Statement
No competing financial interests exist.