
Abstract
Abstract
Background and Objectives:
High altitude may increase blood pressure (BP) and the kidney plays an important role in acclimatization. Little is known about how transplanted kidneys respond to the hypoxic stress at high altitude. We compared 24 hour ambulatory BP in a climber with a kidney transplant and hypertension at sea level and at high altitude (2860–4300 m).
Methods:
Welch-Allyn ABPM 6100 monitor was used to collect heart rate, systolic BP (SBP), and diastolic BP every 30 minutes while awake, and hourly while asleep. BP was monitored for 49 hours at sea level and for 53 hours at 2860–4300 m.
Results:
Overall mean SBP did not differ between altitudes. At high altitude, the participant's mean nocturnal BP increased, but this “reverse dipping” pattern was not observed at sea level. The participant had no evidence of altitude illness or infectious complications at high altitude.
Conclusions:
This case builds on previous reports that kidney transplant recipients may safely travel to high altitude. Further study is required to determine the generalizability to other travelers with kidney transplant and/or underlying hypertension, and the clinical significance of short-term elevated nocturnal BP at high altitude.
Introduction
With the increase in adventure travel and advancing medical technologies, a growing number of individuals with major comorbidities and polypharmacy are traveling to high altitude (Keyes et al., 2016). Hypertension is one of the most common diseases in both the general population and high altitude trekkers (Faulhaber et al., 2011; Keyes et al., 2016). Information is limited on people with chronic kidney disease or solid organ transplant at high altitude (Luks et al., 2008; White et al., 2009; Luks, 2016). Whether these conditions predispose individuals to acute altitude illnesses or other pathological responses at high altitude remains unclear.
The kidney plays an important role in acclimatization by moderating volume status and erythropoietin production (Goldfarb-Rumyantzev and Alper, 2014). Prior investigations suggest that these functions should be preserved in renal transplant recipients (Luks, 2016) though only a few reports have examined clinical outcomes of kidney transplant patients at high altitude (White et al., 2009; Suh et al., 2015; van Adrichem et al., 2015) and none of these participants had associated hypertension.
Travel to high altitude may influence blood pressure (BP) differently in normotensive and hypertensive individuals (Keyes et al., 2017). Furthermore, the role and efficacy of antihypertensive medications in hypertensive individuals at altitude remain unclear (Luks, 2009; Bilo et al., 2011; Parati et al., 2014).
We present a case study of a hypertensive renal transplant recipient at high altitude and compare his 24-hour ambulatory BP (ABP) at low and high altitude.
Case Presentation
We evaluated a 57-year-old man who received a cadaveric kidney transplant in 2002 at age 45 years due to type 2 membranoproliferative glomerulonephritis and end-stage renal disease. He progressively returned to mountain sports within 6 months of receiving his transplant and was back to mountaineering within 1 year. Since his transplant he has been >6000 m on multiple occasions and has reached a maximal altitude of 6500 m without developing mountain sickness or other acute problems.
His medical history also includes hypertensive cardiomyopathy and mild valvulopathy. There was no history of diabetes. His medications include losartan 50 mg daily, doxazosin extended release 4 mg daily, mycophenolate mofetil 250 mg twice daily, tacrolimus 2.5 mg daily, deflazacort 6 mg daily, allopurinol 100 mg daily, and 25-hydroxyvitamin D 0.266 mg every 2 weeks. These medications did not differ between study periods at high altitude and at sea level, except that the dose of doxazosin was increased to 8 mg twice daily 4 months before the low-altitude study period.
The patient had no proteinuria at a clinic visit in September 2015, 4 months before the low-altitude study period and 11 months after the high-altitude study period. His clinic weight was 65.5 kg in September 2014, 1 month before high-altitude visit and 62 kg in September 2015, 4 months before low-altitude evaluation.
High-altitude ABP was measured in the Khumbu valley, Nepal, when the participant enrolled as a participant in a prospective observational cohort study on BP, hypertension, and high altitude in October 2014 (Keyes et al., 2017). Because of the limited information on kidney transplant patients at high altitude, we solicited the participant's consent to perform additional 24-h ABP monitoring at sea level for this report, and to share these data with his physicians. He gave written consent to participate in the larger study and for this case report.
Welch-Allyn ABPM 6100 monitor was used to collect heart rate, systolic BP (SBP), and diastolic BP (DBP) every 30 minutes 07:00–22:00 hr, and hourly 22:00–07:00 hr. Summary high-altitude data have been partially reported separately (Keyes et al., 2017). In this study, we compare detailed ABP measurements during ascent from 2860 to 4300 m with ABP measured at near sea level in the south of Spain in January 2016, 15 months after the high-altitude study period. The participant wore the device for 2 consecutive days and we recorded his daily activities. Acute mountain sickness (AMS) was evaluated using the Lake Louise score (LLS) at 2860, 3440, and 4300 m with a score of 3 or more including headache considered positive for AMS.
Results
High-altitude ascent
24-ABP was measured for a total of 53 hours during ascent from 2860 to 4300 m. The percentage of overall, awake, and asleep BP values above American Heart Association (AHA) recommended normal cutoffs was 42%, 25%, and 93%, respectively (O'Brien et al., 2013). Nocturnal BP demonstrated a reverse dipping pattern. SBP and DBP rose 7% and 18%, respectively. BP varied with activity, but mean SBP and DBP remained similar across altitudes and showed no relationship with altitude (Table 1 and Fig. 1).
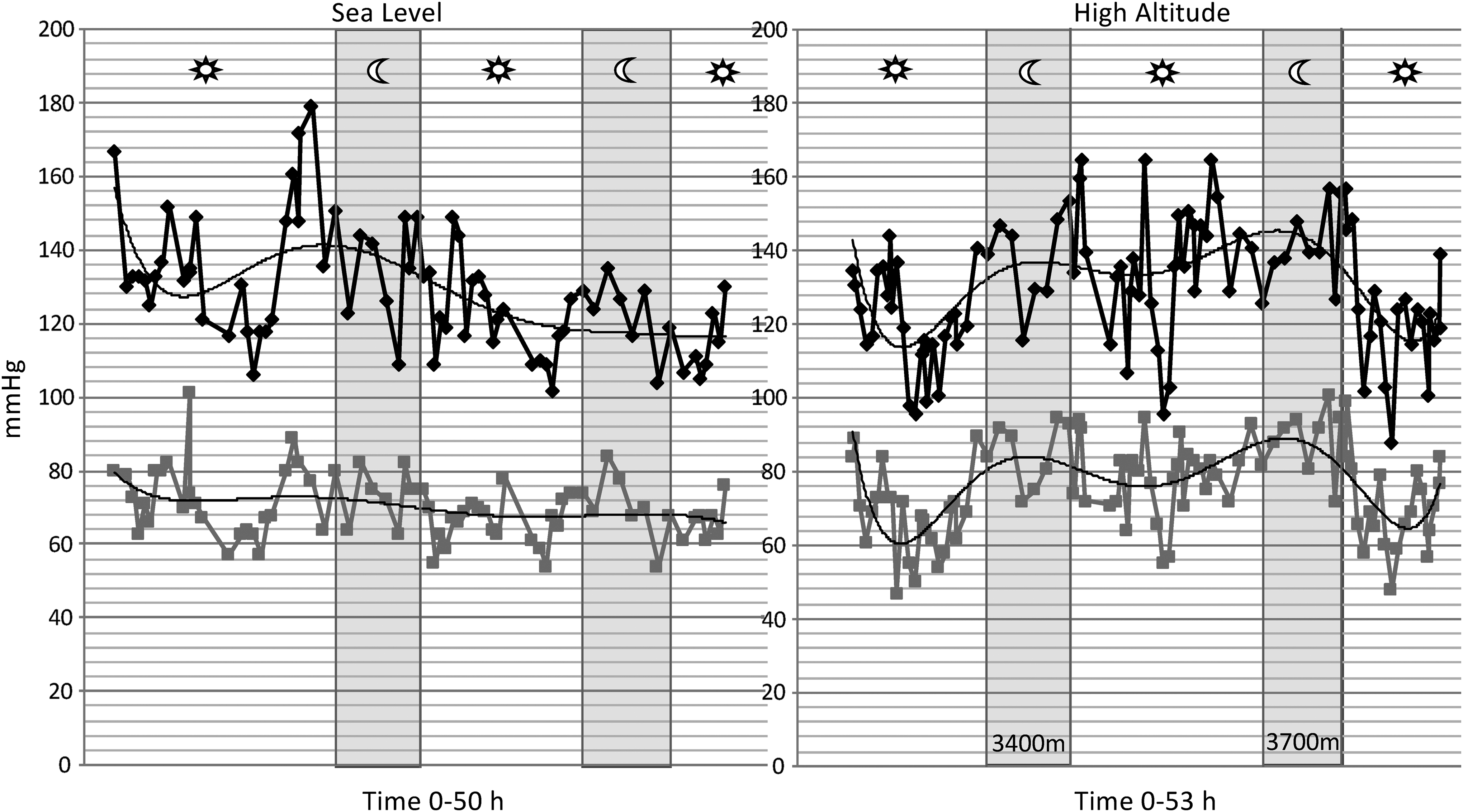
Systolic (black) and diastolic (gray) blood pressure measurements over the study period at sea level and at high altitude. Light gray areas designate sleep times.
Mean Ambulatory Blood Pressure and Heart Rate at Sea Level and During Trekking and Sleep Between 3440 and 4300 m
DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure; SD, standard deviation.
The patient reported no symptoms of AMS when assessed contemporaneously at 2860, 3440, and 4300 m by formal recording of LLS. He also denied any symptoms occurred during his ascent to 5000 m when questioned verbally about this after descent to 4300 m. He had no clinical evidence or complaints of peripheral edema at any altitude. He also denied symptoms of infection throughout his high-altitude sojourn.
Comparison between sea level and high altitude
Sea level and high-altitude ABPs were measured for a total of 49 and 53 hours, respectively. Activity logs showed less sustained activity at sea level, although strenuous physical activity was recorded on both days at sea level (data not shown).
Mean overall and awake SBPs were the same at sea level and high altitude (Table 1). At sea level, fewer BP values were above AHA normal cutoffs compared with high altitude (overall 25.0% vs. 41.9%, awake 23.2% vs. 25.3%, and asleep 31.3% vs. 92.9%, respectively). However, the highest measured BP occurred at sea level, and maximum measurements at sea level were higher than maximum measurements at high altitude (Table 1). There were no critically high SBP measurements (>180 mmHg) at either altitude.
Mean nocturnal SBP and DBP were lower at sea level (Table 1). Overall DBP was higher at high altitude due to the increase in nocturnal DBP. At sea level, nocturnal SBP and DBP decreased by 4% and 1%, respectively. The observed decrease did not reach the dipping cutoff of 10%, classifying the participant as “nondipper,” whereas at high altitude, nocturnal BP paradoxically rose above daytime values, classifying him as a “reverse-dipper” or “riser.”
Discussion
In this climber with a kidney transplant and hypertension, overall mean SBP did not differ by altitude and maximal BP values occurred at sea level. He did not develop AMS, suggesting his transplanted kidney was able to respond with appropriate diuresis and natriuresis to help him acclimatize (Luks, 2016). In addition, despite immunosuppressant medication, he developed no serious infectious diseases during his trek.
Of note, the patient's nocturnal BP pattern differed between sea level and high altitude. Nondipping and reverse-dipping tendencies are more common in patients with chronic kidney disease and in kidney transplant recipients than in the normal population (Redon et al., 1999; Velasquez et al., 2016). These tendencies are associated with worse long-term clinical outcomes (Muxfeldt et al., 2009; Wang et al., 2016); however, the short-term significance of this phenomenon at high altitude is unknown. Our subject remained asymptomatic and demonstrated no adverse short-term effects. Whether longer high-altitude exposure with persistent nondipping or reverse dipping might have long-term adverse consequences is also unknown and may merit further investigation.
The reverse-dipping pattern was not present when measured at low altitude. This may relate to sympathetic activation that occurs at high altitude (Mazzeo et al., 1995; Hansen and Sander, 2003) and is associated with higher nocturnal BP (Chouchou et al., 2013). Sleep is impaired at high altitude, and the higher nocturnal pressures could represent the patient being awake at night (Bloch et al., 2015). In addition, serum sodium concentration has been associated with nocturnal BP response (Bankir et al., 2008) and dietary sodium may have varied between home and a trekking/climbing diet that may be higher in sodium.
Measurements were made 15 months apart and, therefore, changes in the patient's clinical status may also contribute to the differences between altitudes. Importantly, he was on an increased dose of doxazosin, an alpha blocker, which may have a greater effect on nocturnal BP than on daytime pressure. Interestingly, the patient had his highest BP at daytime, at low altitude, while on the higher dose of medication.
The patient had a higher clinic weight before the high-altitude measurement than the low-altitude measurement. We cannot determine whether this was due to water or muscle mass, though the patient was training for the climb. These clinic weights do not necessarily reflect the patient's weight during the study periods and we have no contemporaneous measurements of his volume status. Clinically, he had no evidence of edema or volume overload at high altitude. Given that diuresis is a hallmark of acclimatization, it is unlikely that volume overload accounted for higher nocturnal BP, though differences in volume status could explain higher maximum pressures at sea level.
High-dose glucocorticoids are another potential cause of nondipping (Prisant, 2004). The patient's glucocorticoid regimen did not change however between measurements. Some reports have suggested that nocturnal nondipping is inconsistent and may not be reproducible (Prisant, 2004). A strength of our report is that we observed a consistent pattern on two nights, rather than a single measurement at each altitude.
This case builds on previous reports that kidney transplant recipients may safely travel to high altitude (Suh et al., 2015; van Adrichem et al., 2015). Our case is unique in that the patient also had underlying hypertension and was older than the participants in earlier studies. Despite his complicated medical history, our patient has been able to enjoy a successful high-altitude mountaineering career. Our findings suggest the need for future work to confirm whether high altitude impairs nocturnal dipping in other people with kidney transplants or hypertension.
Footnotes
Acknowledgments
This article was funded, in part, by a Hultgren grant from the Wilderness Medical Society and the Nepal International Clinic. We thank Welch-Allyn for its generous donation of the 24 ABPM monitor and our patient for his participation.
Author Disclosure Statement
No competing financial interests exist.