
Abstract
Ortiz-Prado, Esteban, Katherine Simbaña-Rivera, Diego Duta, Israel Ochoa, Juan S. Izquierdo-Condoy, Eduardo Vasconez, Kathia Carrasco, Manuel Calvopiña, Ginés Viscor, and Clara Paz. Optimism and health self-perception-related differences in indigenous Kiwchas of Ecuador at low and high altitude: a cross-sectional analysis. High Alt Med Biol. 23:26–36, 2022.
Background:
Living at high altitude causes adaptive responses at every physiological and molecular level within the human body. Emotional and psychological short- or long-term consequences, including mood changes, higher mental overload, and depression prevalence, as well as increased risk to commit suicide have been reported among highlanders. The objective of this report is to explore the differences in self-reported dispositional optimism and health perception among sex-, age-, and genotype-controlled indigenous Kiwcha natives living at two different altitudes.
Methods:
A cross-sectional analysis of the comparison of means of subscales and summary scores of the 36-item short-form health survey (SF-36) self-reported questionnaire and the Life Orientation Test-Revised was conducted among 219 adults Kiwchas living at low (230 m) and high altitude (3,800 m) in Ecuador.
Results:
High-altitude dwellers presented lower scores in all the studied dimensions of SF-36 and the total score. Differences were found for the role limitation sphere due to vitality (p = 0.005), mental health (p = 0.002), and social functioning (p = 0.005). In all the cases, participants living at low altitudes scored higher than those living at high altitudes. Lowland women were more optimistic than their high-altitude counterparts.
Conclusions:
We observe that populations located at high altitudes have more unfavorable self-reported health states. Although our results depict the existence of significant differences in the health status of indigenous peoples living at different altitudes, further studies are needed to explain in depth the sociodemographic and/or environmental factors that might underlie these differences.
Introduction
Humans have settled in almost every region of the planet, including those high-altitude mountainous regions around the world (West et al., 2007). These particular regions are often hostile, having colder temperatures and lower atmospheric pressure than places situated close to sea level. Currently, more than 5.7% of the population reside above 1,500 m of altitude and at least 140 million live above what is considered high altitude (2,500 m) (Burtscher, 2014). It has been difficult to define at which elevation the effects of high altitude become more severe and where the threshold is located in terms of mild or severe hypoxia (West et al., 2007).
Imray in 2011 (Imray et al., 2011) used the classification of high-altitude exposure according to the recommendations from the International Society of Mountain Medicine, a categorization that seems to be most pragmatic. The author defined low altitude as everything located below 1,500 m, moderate or intermediate altitude between 1,500 and 2,500 m, high altitude from 2,500 to 3,500 m, and the very high altitude from 3,500 m to 5,800, and more than 5,800 extreme high altitudes, and above the 8,000 m is considered the death zone (Imray et al., 2011).
The effects of high-altitude exposure on people have been described several times before (West et al., 2007; Burtscher, 2014; Moore, 2017). Acute exposure to hypobaric hypoxia, especially above 2,500 m, triggers several physiological responses in the body, mainly driven by cardiorespiratory compensatory mechanisms (Naeije, 2010; Gaur et al., 2021). At the same time, chronic and long-term exposure to high altitude have been associated with genetic, anatomic, and physiological compensatory mechanisms that create better-adapted organisms to live in high-altitude locations (Beall, 2007; Moore, 2017; Julian and Moore, 2019).
The effects of long-term high-altitude exposure on the central nervous system and cognitive development have been studied before (Aquino Lemos et al., 2012; Wehby, 2013; Yan, 2014; Hu et al., 2016). Most analyses have been conducted in animal models and have shown that neurological tissue maturation and cellular replication might be affected during simulated hypobaric hypoxia (Floyd et al., 2020). In humans, studies on neuropsychological functioning are scarce. In small cohorts, it has been reported that children born above 4,000 m of elevation are less attentive and responsive to visual and auditory stimuli than children born at lower altitudes (Saco-Pollitt, 1981). Neuropsychological assessment among high-altitude children and adolescents indicated a minor reduction in psychomotor speed with increasing altitude (Hogan et al., 2010).
Despite this evidence, the long-term effects of chronic hypoxia on human behavior and attitudes toward life have rarely been studied (Kious et al., 2018). It has been hypothesized that living at high altitude may have an effect on the serotonin metabolism, reducing the synthesis of the 5-hydroxytryptophan (5-HTP), thus decreasing serotonin levels within the central nervous system (Kious et al., 2018). The results published by Kious et al. (2018) might direct our understanding on how low serotonin levels might be linked to mood symptoms that are common among people residing at high altitude (Kious et al., 2018).
It has also been reported that brain chemistry seems to be altered due to long-term exposure to higher altitude (Shi et al., 2014; Hwang et al., 2019). Del Maestro, Ahmad, Dong, and de Aquino also reported significant correlations between high-altitude depression, anxiety-related symptomatology, and sleep problems (DelMastro et al., 2011).
The time-lapse between the exposure to high altitude and the presence of measurable effects is still unclear. Some reports suggest that even short-term visits to high-altitude locations might have a negative impact on mental health (MH). For instance, Barbara Shukitt-Hale and Harris R. Lieberman in 1996 have described the effects of altitude on cognitive performance and mood states (Shukitt-Hale and Lieberman, 1996). They have reported that even 1 month of high-altitude exposure was sufficient to increase emotional instability (Shukitt-Hale and Lieberman, 1996). Psychotic symptoms have also been reported among healthy mountain climbers, while reaching extreme altitudes even for relatively short periods of time (Hüfner et al., 2018).
Previous research has also described adverse effects in populations residing in harsh or unwelcoming climates (Kurlansik and Ibay, 2012; Melrose, 2015). Seasonal affective disorder is a condition in which life self-perception can be deteriorated in colder climates (Kurlansik and Ibay, 2012). The fact that living at higher altitudes is often associated with colder weathers could be associated with this negative response toward life among highlanders.
All these effects might be linked, at least partially, with the development of some psychiatric conditions. For instance, the role of high-altitude hypoxia as a risk factor for major depression or suicide has also been reported (Gamboa et al., 2011; Ortiz-Prado et al., 2017; Reno et al., 2018). Despite the availability of some evidence, it could be interpreted that chronic hypoxia exposure is associated with poor outcomes in MH and pessimistic attitudes about the future. In this sense, we have conducted what we believe is the first comparative analysis of the differences in self-perception toward physical and MH, emotional well-being, and dispositional optimism in two well-controlled populations located at low and high altitude.
We hypothesize that those living at high altitudes will show worse perception of their own physical and MH than those living at low altitudes.
Methods
Study design
A cross-sectional analysis of differences in self-reported physical and MH status and dispositional optimism among Kiwcha natives living in low and high altitudes in Ecuador.
Setting
This study was carried out in two different cantons in Ecuador: Oyacachi located at 3,800 m of elevation in the province of Napo with a population of 570 adult Kiwchas living at high altitude and Limoncocha, a canton with 890 adults Kiwcha natives living at 230 m in the Amazonian province of Sucumbios.
Participants
This study included 219 adult Kiwchas, 135 women (61.5%) and 84 men (38.5%), who voluntarily agreed to participate in the study. In Oyacachi, a small Kiwcha community with 570 adults, we recruited 96 participants, and in Limoncocha, a community with 890 adults, we recruited 123 volunteers. In both communities, Spanish and Quechua are the only spoken languages. Because in some cases there may be dwellers who speak one language better than the other, an official translator was included as part of fieldwork in both communities.
Inclusion criteria
The study was carried out in otherwise healthy women and men who volunteered with their participation in the study. The age range included every person older than 18 years, who was legally able to participate in the study. We only included subjects who were raised and born in their communities and have not left their home for more than 3 months at once.
Exclusion criteria
We excluded those volunteers that were younger than 18 years of age or those who were not born in Limoncocha or Oyacachi.
Variables and outcomes
Health status
We evaluated health profiles among participants using the 36-item short-form health survey (SF-36) (Ware and Sherbourne, 1992), a well-known self-reported questionnaire used to assess perceived health status. The questionnaire evaluates eight dimensions of physical and emotional well-being. The dimensions included in the questionnaire are physical functioning, role functioning, role emotional, vitality (VS), MH, social functioning (SF), body pain, and general health (GH). In addition, the SF-36 includes a question addressing health change in relation to the last year. In this study, we used the Spanish version of the SF-36 (Prieto and Anton, 1995), which has demonstrated good psychometric properties (Vilagut et al., 2005) that are comparable with those found for the original version in English.
Optimism
This construct was assessed using the Life Orientation Test-Revised (LOT-R) (Scheier et al., 1994), a 10-item scale that measures how optimistic or pessimistic the person feels about the future. We used the Spanish version of the scale (Otero et al., 1998), which present, good psychometric properties (Gustems-Carnicer et al., 2017).
Outcome
To find significant differences in terms of self-perception, quality of life and optimism between the two groups.
Data sources
Individual-level sociodemographic information, place of residence, and past medical history were obtained in situ in both communities. Information on the SF-36 self-questionnaire and the LOT-R was deployed within the communities with the help of our research team members in case someone had any question. Both questionnaires were presented in Spanish (see Supplementary Data), because the two communities are fluent in Spanish, while a continuing follow-up was provided during the entire process in case any doubt on word meaning arouse. In case someone could not fully understood some word or any part of the questionnaire, a local translator (Spanish-Quechua) was present at any time to resolve any linguistic trouble.
Study size and sample size calculation:
In terms of the number of patients required to achieve significance, the sample size (n) and margin of error (E) were given by the following formula:
where N is the population size (n = 570 in Oyacachi and n = 890 in Limoncocha), (r) is the fraction of expected responses (50%), and Z(c/100) is the critical value for the confidence level (c). The total number of medical and physical evaluation required to achieve significance was 82 for the high-altitude group and 96 for the low-altitude control group.
Data analysis
Descriptive statistics were used to analyze and visualize differences between the two populations. Before conducting any analysis, normality tests were conducted to choose the appropriate analyses to be performed. After testing for normality using a Levene's test, most variables did not meet the requirements to be treated as parametric, thus, non-parametric test were used to asses statistical differences. Unpaired Wilcoxon test was performed to test differences of continuous variables and Chi-squared test was used to test the association or independence of categorical variables. When the expected values were <5 in any of the categories, Fisher's exact test or Spearman's test was used when the variable had evident asymmetries with histograms before the selection of the test. All statistical analysis accepted significance with a p-value <0.05. Bonferroni's correction was used to avoid family-wise error rate for each group of multiple comparisons α = 1−(1−α) 1/k. All calculations were completed using the R software (R Core Team, 2020).
Ethical consideration
A full ethics approval was obtained (MED.EOP.17.01) throughout the Universidad de las Americas bioethics committee (CEISH). All participants voluntarily signed an informed consent form accepting and fully understanding the objective of our study. A local Quechua-Spanish translator was hired in both communities in case anyone had problems understanding some parts of the informed consent or the questionnaires. To protect the identity and autonomy of every subject, all personal or identifiable information was anonymously coded to guarantee their individual rights.
Results
A total of 219 persons fully completed the self-reported questionnaires, 56% (n = 123) were part of the low-altitude group and 44% (n = 96) were from the high-altitude group.
Age and sex differences
In the low-altitude (Limoncocha) group, 37.5% (n = 44) were men and 63.5% (n = 79) were women, while in the high-altitude group (Oyacachi), 41.6% were men (n = 40) and 58.4% (n = 56) were women. No significant differences were found regarding the distribution of participants by sex (p-value: 0.54).
In the lowland group, the mean age was 43 years (standard deviation [SD] = 17), while in the high-altitude group, the mean age was 42 years (SD = 17). These differences were not statistically significant (p = 0.8)
SF-36 self-administered questionnaire
The overall scores for the SF-36 questionnaire show a significant difference between the low- and high-altitude group (Table 1).
The Overall Scores for the 36-Item Short-Form Health Survey Questionnaire Show a Significant Difference Between the Low- and High-Altitude Group
After using Bonferroni's correction, the significance level was set up at p = 0.0051.
IQR, interquartile range; SF-36, 36-item short-form health survey.
The median and the interquartile range of scores for each domain and for the total score of the SF-36 by the altitude (low vs. high) show differences in most subscales (Fig. 1)
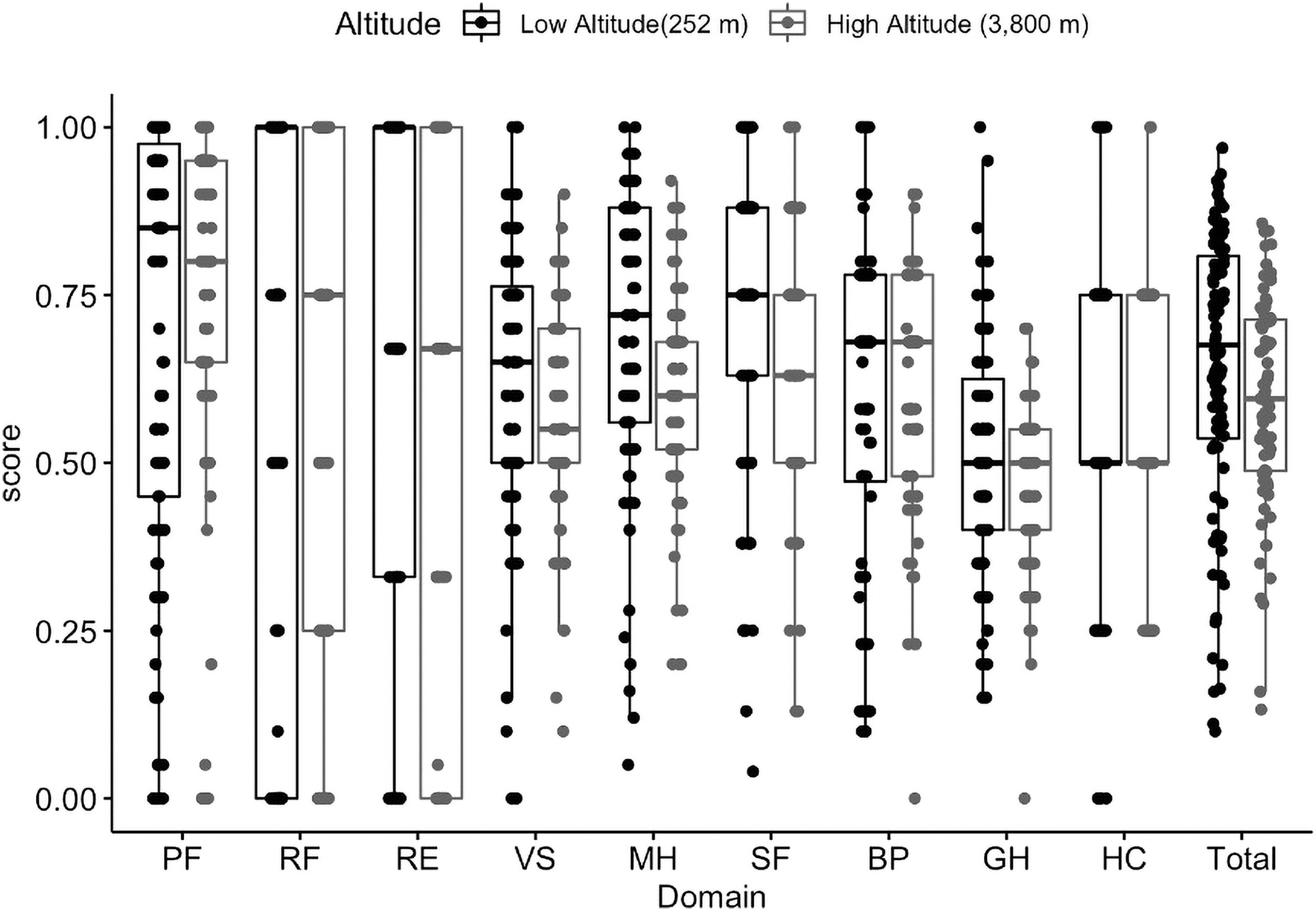
The median and the interquartile range of scores for each domain and for the total score of SF-36 by low altitude (gray) versus high altitude (dark gray). BP, body pain; GH, general health; HC, health change; MH, mental health (emotional well-being); PF, physical functioning; RE, role functioning/emotional; RF, role functioning/physical; SF, social functioning; SF-36, 36-item short-form health survey; Total, SF-36 total score; VS, vitality (energy/fatigue).
Unpaired Wilcoxon tests, for comparing the scores by altitude, indicated that the scores were significantly different for the dimensions; after using a Bonferroni's correction, the significance level was set at p = 0.0051: VS (p = 0.005), MH (p = 0.002), and SF (p = 0.005).
Perceived health by sex
For males, the results after Bonferroni correction (p = 0.0051) indicate no significant differences between men living at low altitude and those living at high altitude. Also, no significant differences were found for the scores of women living at low altitude compared to those living at high altitude. No significant differences were found between men and women within the same location (Table 2).
36-Item Short-Form Health Survey (SF-36) Total Score and SF-36 Domains' Scores for Each Sex and Altitude Where Participants Were Living
After using Bonferroni's correction (significance level at p = 0.0051), no significant differences were found within sexes.
Perceived health by age group
Figure 2 shows the median scores for each dimension and the whole SF-36 for each age group (young adults, adults, and elderly) by living altitude. For young adults, after Bonferroni correction (p = 0.0051), significant differences were found regarding MH (p = 0.002) and GH (p = 0.004). Table 3 shows median and interquartile range (IQR) for each age group by altitude they were living in.
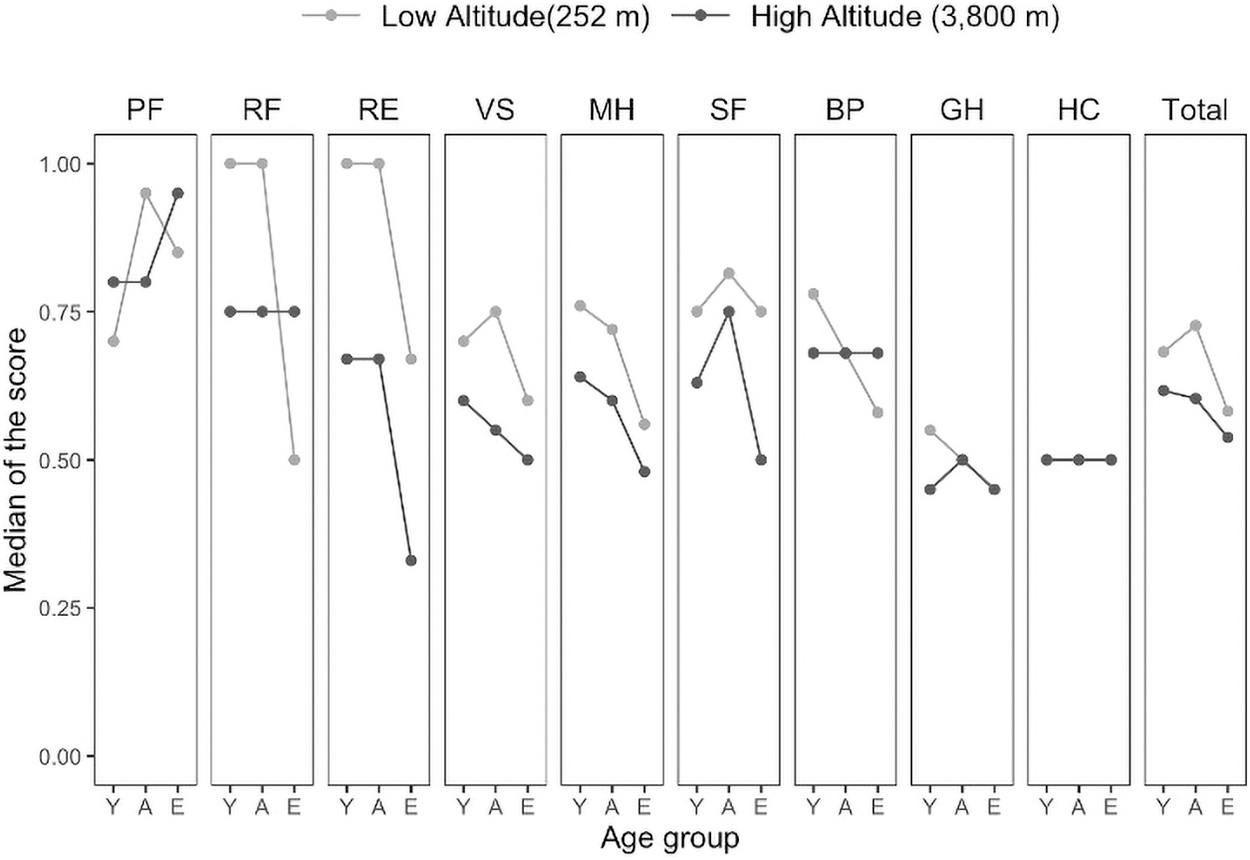
SF-36 total score and domains' scores by altitude where participants were living according to age group. A, adults; E, elderly; Y, young adults.
36-Item Short-Form Health Survey (SF-36) Total Score and SF-36 Domains' Scores for Each Age Group and Altitude Where Participants Were Living
After using Bonferroni's correction, we set up the significance level at 0.0051.
Young adults living at low altitude presented higher scores than those living at high altitude. For adults and elderly, no significant differences were found in relation to the scores of dimensions of the SF-36, and neither for the total score (Fig. 2).
Optimism and pessimism using the LOT-R
The LOT-R results in the lowland people had a median of 16.0 (IQR: 14.00–18.00), the same as the high-altitude group 16.0 (IQR: 13.00–17.50). No significant difference was found in the overall comparisons (p = 0.37).
When comparing the results by sex, women scored 16.0 in the low-altitude group (IQR: 15.0–18.0) and 15.0 (IQR: 13.0–17.0) in the high-altitude group, showing a statistically significant difference (p = 0.029), which indicates that women living at low altitude are more optimistic than those living at high altitude.
For men, the low-altitude group had a median score of 16.0 (IQR: 14.0–18.0), while the high-altitude group had a median of 18.0 (IQR: 14.9–19.0); although men living at high altitude scored higher in the LOT-R test, this difference was not statistically significant (p = 0.15). Also, no significant differences were detected when comparing each age group regarding the altitude of residence, young adults (low altitude = 16, IQR = 14.00–18.00; high altitude = 15, IQR = 13.00–18.00), adults (low altitude = 15, IQR = 14.00–18.00; high altitude = 16, IQR = 13.00–17.00), and elderly (low altitude = 17, IQR = 15.00–18.00; high altitude = 17, IQR = 15.50–18.00).
Sociodemographic differences between communities
In terms of sociodemographic differences, we recognize that high-altitude inhabitants have a greater share of economically active population than the low-altitude group (Table 4).
Demographic Characteristics of Oyacachi and Limoncocha Parish
Although more people work at Oyacachi, education attainment is lower among highlanders; despite this, access to running water, electricity, and garbage collection is easier for highlanders (Table 4).
Discussion
This is the first study that aims to evaluate the level of optimism among people living at different elevations and one of very few studies analyzing health status self-perception at different altitudes (Gonzales et al., 2013). We have used the SF-36 scale, which is one of the most widely used quality-of-life scales related to GH (HRQOL) in the world (Alonso et al., 1995; Lima et al., 2009). This tool has been widely validated in different languages, as well as being reliable for clinical and research uses. An additional advantage of the SF-36 is the generation of eight domain scores, which give doctors and nurses a quick overview of different aspects of HRQOL of their patients (Abbasi-Ghahramanloo et al., 2020; van der Meulen et al., 2020).
When analyzing the data obtained from both indigenous groups located at a high and low altitude, we found significant differences in SF-36 dimensions related to physical symptoms such as VS, a dimension that assesses behaviors related with energy and fatigue, which is a common body response to high-altitude exposure (Naeije, 2010; Gaur et al., 2021). Unsurprisingly, and in line with our hypothesis, those living at high altitude present less VS. In fact, it seems that this perception is also supported by the presence of psychological symptoms, represented by worse MH and SF in indigenous people from high altitude than those living in low altitude.
The presence of these psychological difficulties in the population living at high altitude could be due to the alteration of serotonin metabolism and brain bioenergetics, attributable to permanent hypobaric hypoxia exposure (Kious et al., 2018). Bardwell et al. found a significant deterioration in the mood of marines exposed to training in high-altitude locations and stress stimuli (cold, physical activity, and decreased oxygen availability) characterized by increased fatigue, anger, and depression, which may persist even 90 days after exposure to those conditions.
This may be due to an increase in the levels of stress hormones that could cause a bad mood (Bardwell et al., 2005). When evaluating alterations in the hypothalamic pituitary adrenal axis, in the face of exposure to high altitude among hikers and natives, discovering an increase in cortisol levels when exceeding 3,000 m above sea level, however, the cortisol levels of natives (Sherpas) did not change (Park et al., 2014). Also, the results might be explained in light of the possibility of development of chronic mountain sickness, an incapacitating syndrome due to lifelong exposure to hypoxia experienced by people living at high altitude (Villafuerte and Corante, 2016).
Patients with this syndrome complain about difficulty in exercising and presenting bone and join pain, which can aggravate performance in job and the perception of fatigue, and less VS, as indicated by our participants living at high altitudes. It is clear that altitude produces changes in the organism, which might lead to mood changes, but at the same time, mood changes can cause physical symptoms, like psychomotor retardation in depression (Buyukdura et al., 2011), which reduce behavioral components that might explain the perception of fatigue and less VS in high-altitude inhabitants.
Other sociodemographic and environmental factors might be involved in the origin of these differences. Certainly, people living at high altitude face different situations that those living at low altitude (e.g., weather conditions, steep locomotion, access to natural resources, etc.), which might explain their divergent SF. Then, it is not possible yet to assert that geographical altitude “per se” is the only factor that explains the presence of such psychological affectations.
In this sense, geographical, climatological, and environmental factors are significantly different in both communities (GAD Oyacachi, 2019; GAD Limoncocha, 2019). Oyacachi is located at a very high altitude (2,500–3,500 m) according to The International Society of Mountain Medicine, while Limoncocha is located at low altitude (<1,500 m) (Imray et al., 2011) (Fig. 3.

Topographical map of Ecuador displaying and highlighting the location of the cantons of Oyacachi (in the Andes Mountains) and Limoncocha (in the Amazon Rainforest). Map elaborated by the authors using ArcGis.
Oyacachi has an average range that goes from—2° to 17°C degrees, while in Limoncocha, temperature varies from 18 to 26°C. Living in colder weather, as well as living in harsh weather, has been associated with behavioral changes that are linked to depression (Wirz-Justice et al., 2019; Øverland et al., 2020).
The effects of altitude on mood are evidenced from another point of view from multiple studies that have found higher rates of suicide in residents of altitude; however, these are studies were developed from a database with limitations (Brenner et al., 2011; Reno et al., 2018). Betz et al. (2011) conducted an individual analysis of cases; it found that individuals who suffered suicide were more likely to have relatives with a history of depression; in the same way, several factors such as age, gender, and residence can influence access to health care in high-altitude populations. Also, Sabic et al. (2019) reported a link between altitude and suicide among US Army veterans, thus demonstrating that even in well-developed countries, presumably with minor interlocal sociodemographic differences, altitude is associated to a higher mental overload.
By segregating the groups by gender, no significant difference was found by gender. Also, no significant differences were reported between adult and elderly populations of the two study groups, probably explained by the presumption that elderly populations are often less likely to articulate MH problems due to the concerns of stigma, shame, and cultural and religious misconception (Jang et al., 2009).
Geographical altitude and weather conditions can certainly affect cultural habits and specifically how people socialize. Persons living at high altitude spend more time within their homes due to harsher weather, which certainly affects socialization. It seems in our studied populations the effect of altitude is different according to gender, probably due to differences in tasks performed day by day, especially because women tend to stay at home most of the day and also can have less interest or access to information about opportunities to development, which can result in a more pessimistic view of the world.
When separating the groups by age, differences between the two locations were only found in young adults. Most of the differences were observed in dimensions related with psychological distress. Young adults living at high altitudes were more prone to MH distress when compared with their counterparts living at low altitude. Apparently, this could be due to different degrees of cultural influence in different age groups, Jang et al. (2009). It showed that older adults are more exposed to altered cultural concepts and stigmas regarding mental illnesses, which are evidenced as a negative attitude toward MH services; this could translate into difficulties to express alterations in the mood of elderly populations in our study.
In terms of optimism, we only found that women have a less optimistic view toward the future among the high-altitude dwellers, while among men, we found no statistically significant differences. We speculate that men due to social pressure may choose to report that they feel better and have a better view of their future regardless of where they live, while women, often being more realistic than men, report more accurately than men (Brenner and DeLamater, 2016). Chang et al. (2010) found statistically significant gender differences in reporting psychological outcomes: men were more likely to report more positive psychological outcomes for themselves rather than for others, and women were more likely to report more negative and realistic psychological outcomes for themselves.
In relation to the effects of chronic hypoxia on people's optimism, it can be speculated that living in conditions with a generally more hostile climate, colder, rainier, and with less available partial pressure of atmospheric oxygen, may cause people to feel more vulnerable toward their future.
Although we know that the level of education can be linked to a person's perception of his or her own reality and emotional situation. The high-altitude group has 13.7% of illiteracy, while the low altitude group has 5.43% (Table 4); nevertheless, both parishes have 5 schools per every 1,000 inhabitants (GAD Oyacachi, 2019; GAD Limoncocha, 2019). In view of differences in terms of sources, external income and having oil and gas production in Limoncocha (low altitude) might interfere with major access and better quality in terms of education.
At the same time, access to health care in both parishes is similar, both having only one primary health center for their entire population, assuming that there are more similarities than differences between these two populations.
These results are the first one in the world reporting optimism levels among high-altitude dwellers, and while more definitive information and results are needed, opening the door for future studies is always necessary.
Limitations
First, one limitation is a scarcity of data in the literature directly addressing the influence of altitude on MH and well-being. Another limitation of this study is that, despite obtaining a significant sample to carry out this research, not all people belonging to these indigenous communities, who met the inclusion criteria, were willing to participate. Whether the inclusion of these subjects who did not participate would have produced variations in our data or even induced changes in some results is impossible to elucidate.
We are also aware that the SF-36 questionnaire is not well validated in the elderly; therefore, we have been cautions to emit definitive conclusions. A minor problem related with questionnaires is that we required applying the translation to Spanish and the intervention of a Spanish-Quechua translator to clarify some word meaning in the forms. Anyway, all participants were able to complete the questionnaire with no help once possible, meaning troubles were solved.
The lack of regression and correlation analyses, not employing variables that could predict well-being variables such as income, education level, socioeconomic status, medical comorbidities, reduces the power of our conclusions since these data were not collected. In that sense, we recommend further analysis to try to better understand the complex link between optimism and health-related self-perception at high altitude.
Conclusion
We observe that age-, sex-, and genotype-matched Kiwcha indigenous populations located at different elevations have differences in terms of how they perceive their own health status. High-altitude natives are more likely to report unfavorable health states represented by lower scores in all dimensions of the SF-36, when compared with their counterparts at low altitude. Indigenous people living at high altitude are significantly more prone to report alterations in VS, MH, and SF than those living at low altitude. When comparing age groups, differences were only found among young adults, mostly in dimension related to psychological distress. Although our results reveal the presence of significant differences in health status of indigenous peoples of Kiwcha lineage living at different altitudes, no significant within-sex differences were found. Further studies are needed to explain in depth the sociodemographic and environmental factors that could underlie such differences.
Footnotes
Acknowledgments
The authors thank the patients and their families who contributed to the completion of this analysis. We also want to express our gratitude to the Oyacachi and the Limoncocha health center's staff for their collaboration, while performing our site visits. We thank David Jacome for his contribution to the elaboration of the Ecuadorian topographic map.
Authors' Contributions
E.O.P. was fully responsible for the conceptualization, data collection, and elaboration of the study. E.O.P., C.P., and K.S.R. participated in drafting the article equally and are fully responsible for it. D.D., I.O., and J.S.I.C. visited indigenous communities and applied the questionnaire. I.O., J.S.I.C., and E.O.P. contributed with data collection and the construction of figures and tables. E.O.P., C.P., M.C., E.V., and G.V. contributed with the descriptive statistical analysis and the ![]() section of the article. E.O.P., G.V. and C.P. critically reviewed the entire article and produced several comments before the submission. All authors have read and approved the article.
section of the article. E.O.P., G.V. and C.P. critically reviewed the entire article and produced several comments before the submission. All authors have read and approved the article.
Ethics Approval and Consent to Participate
All data were collected from the patient's medical records after obtaining written informed consent. The study was approved by the Universidad de las Americas review board (CEISH). All data were anonymized, and all identifiable information and biological samples were stored according to the local guidelines.
Consent to Publish
Written informed consent was obtained from every patient in the study.
Availability of Data and Materials
All data are available upon reasonable request. Since information from indigenous communities were studied, only anonymized and not identifiable data can be shared. If you need further detail, please contact us at e.ortizprado@gmail.com
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work: design of the study and collection, analysis, and interpretation of data, and writing, did not receive financial support of any kind, except for the publication fee paid in full by Universidad de las Americas, Quito, Ecuador.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.