
Abstract
David Eidenbenz, Alexandre Kottmann, Ken Zafren, Pierre-Nicolas Carron, Roland Albrecht, and Mathieu Pasquier. Noncompressible chest wall in critically buried avalanche victims with cardiac arrest: a case series. High Alt Med Biol. 26:129–133, 2025.
Introduction:
In avalanche victims with cardiac arrest, a noncompressible chest wall or frozen body is a contraindication to initiating cardiopulmonary resuscitation. The evidence sustaining this recommendation is low.
Objective:
To describe the characteristics and prehospital management of critically buried avalanche victims declared dead on site, with and without noncompressible chest walls.
Methods:
Retrospective study including all critically buried avalanche victims declared dead on site by physicians of a helicopter emergency medical service in Switzerland, from 2010 to 2019. The primary outcome was the proportion of victims with a noncompressible chest wall reported in medical records. Secondary outcomes included victims’ characteristics and the relevance of the criterion, noncompressible chest wall, for management.
Results:
Among the 53 included victims, 12 (23%) had noncompressible chest walls. Victims with noncompressible chest walls had significantly longer burial durations (median 1,125 vs. 45 minutes; p < 0.001) and lower core temperatures (median 14 vs. 32°C; p = 0.01). The criterion, noncompressible chest wall, assessed in six victims, was decisive for declaring death on site in four victims.
Conclusion:
The presence of a noncompressible chest wall does not appear to be a sufficient criterion to allow to declare the death of critically buried avalanche victims. Further clinical information should be sought.
Introduction
In Switzerland, more than 200 people are caught in avalanches annually, resulting in approximately 25 deaths (Berlin et al., 2019; Tschirky et al., 2000; WSL Institute for Snow and Avalanche Research SLF (2023), n.d.). About a quarter of avalanche victims are critically buried (head and chest buried under snow), with survival rates ranging from 39% to 48% (Brugger et al., 2001; Haegeli et al., 2011; Hohlrieder et al., 2007; Procter et al., 2016). The survival probability for avalanche victims with cardiac arrest (CA) is low (Métrailler-Mermoud et al., 2019). Contraindications to cardiopulmonary resuscitation (CPR) in avalanche victims with CA are lethal injuries (such as decapitation or truncal transection), obstructed airway combined with a burial duration of >60 minutes and asystole, or a completely frozen body (Brugger et al., 2013; Lott et al., 2021; Van Tilburg et al., 2017). The criterion “completely frozen body” is related to the notion of a “noncompressible chest wall”. This results in insufficient blood flow to the brain during CPR, making CPR futile (Blasco Mariño et al., 2023; Schön et al., 2020).
The chest wall may become noncompressible for one of two reasons: postmortem rigidity or severe accidental hypothermia (Schön et al., 2020). Postmortem rigidity is caused by the depletion of adenosine triphosphate (ATP), resulting in inability to release the actin-myosin bond in muscle fibers. It begins 2–3 hours after death. Postmortem rigidity is first apparent in body parts with small muscles, such as the jaw and face, followed by regions involving larger muscles, including the trunk (Almulhim and Menezes, 2020; Dettmeyer et al., 2013).
Severe accidental hypothermia may also cause the chest wall to be noncompressible in avalanche victims. The mechanisms leading to muscle rigidity in hypothermia are not well understood, but decreases in enzyme activity, muscle perfusion, neuronal conduction, action potential repolarization, and acetylcholine and calcium release with the cooling of muscles and peripheral nerves likely cause dysfunction and rigidity (Clarke et al., 1958; Stocks et al., 2004). Clinically, this process first manifests as difficulty with fine motor skills, such as hand dexterity, and ultimately may cause the chest wall to be noncompressible in patients with moderate to severe hypothermia, especially in patients with hypothermia-induced cardiac arrest. (Musi et al., 2021; Pasquier et al., 2014; Pasquier et al., 2011).
Evidence for the recommendation to withhold or terminate CPR in patients with a noncompressible chest wall is weak. The relevance of this recommendation in the management of avalanche victims with CA is not known.
Our primary aim was to describe the characteristics and prehospital management of critically buried avalanche victims who were declared dead on site, depending on whether a noncompressible chest wall was reported.
Materials and Methods
Data collection
We retrospectively included all critically buried avalanche victims who were declared dead on site by the physicians of the helicopter emergency medical service, Swiss Air Ambulance-Rega from January 1, 2010, to December 31, 2019. We searched the prehospital medical records for date and location of avalanche accident, sex and age of victim, airway patency (obstructed airway defined as the mouth and the nose being completely filled with compacted snow or debris), presence of an avalanche transceiver, presumptive diagnosis, initial core temperature, medical management, and survival status. A patient was considered to have had a noncompressible chest wall if it was mentioned in the medical record, or if the body was described as completely frozen. Otherwise, the patients were considered not to have had a noncompressible chest wall. Two of the authors (D.E. and M.P.) blindly reviewed the cases and assigned each case to one of the following presumptive diagnostic categories by using predefined specific rules (Supplementary Data S1): trauma, asphyxia, hypothermia, and undetermined.
For each avalanche victim with a noncompressible chest wall, we evaluated whether this information was decisive for their management or not. We considered the criterion, noncompressible chest wall, as decisive if CPR was stopped or withheld immediately after assessment without any other diagnostic or therapeutic procedure, as recommended in the guidelines (Brugger et al., 2013; Van Tilburg et al., 2017). We considered the criterion, noncompressible chest wall, as not decisive if an avalanche victim underwent additional medical evaluation or management (vital signs, electrocardiographic monitoring, core temperature measurement, CPR, or evaluation of airway patency), indicating that the physicians had searched for supplemental clinical information to guide management. Because the criterion, noncompressible chest wall, was first introduced in guidelines for avalanche victims in 2013 (Brugger et al., 2013), we assessed its relevance for decision-making only for the period 2014–2019.
The primary outcome was the proportion of victims with a noncompressible chest wall reported among critically buried avalanche victims with CA. Secondary outcomes were the descriptions of the victims and the assessment of the relevance of this information on management.
Statistical analysis
We entered the data into an Excel spreadsheet (Microsoft, Redmond, WA, USA) and exported the data to Stata version 17 (Stata Corporation, College Station, TX, USA). We present continuous data as mean ± standard deviation (SD) when normally distributed or median and interquartile range (IQR) otherwise. We report categorical data as numbers and percentages. We used Student’s t test to compare continuous and normally distributed variables and the Wilcoxon (Mann–Whitney) two-sample statistic otherwise. We used Pearson’s chi-squared test and Fisher’s exact test for categorical variables. We defined a two-tailed p value of <0.05 as statistically significant. We assessed the agreement of diagnosis classification between the two authors by using the Cohen’s kappa statistic.
The cantonal ethics committee of Zürich (KEK-ZH) granted permission to use patient data without individual consent (BASEC N. 2020-00428).
Results
Of the 330 critically buried avalanches victims rescued during the study period, 53 met the inclusion criteria (Fig. 1). The avalanches in which the 53 victims were caught occurred between November 1 and May 31 at a median altitude of about 2,300 m (IQR 1,800–2,500) above sea level. Twelve of the 53 patients (23%) were described as having noncompressible chest walls. The demographics of the victims and their management are presented in Table 1. The presumptive diagnoses of the 53 victims were reviewed by 2 of the authors. Four of the diagnoses were discrepant (agreement 92%, Cohen’s kappa 0.87). The final diagnoses were determined by consensus.
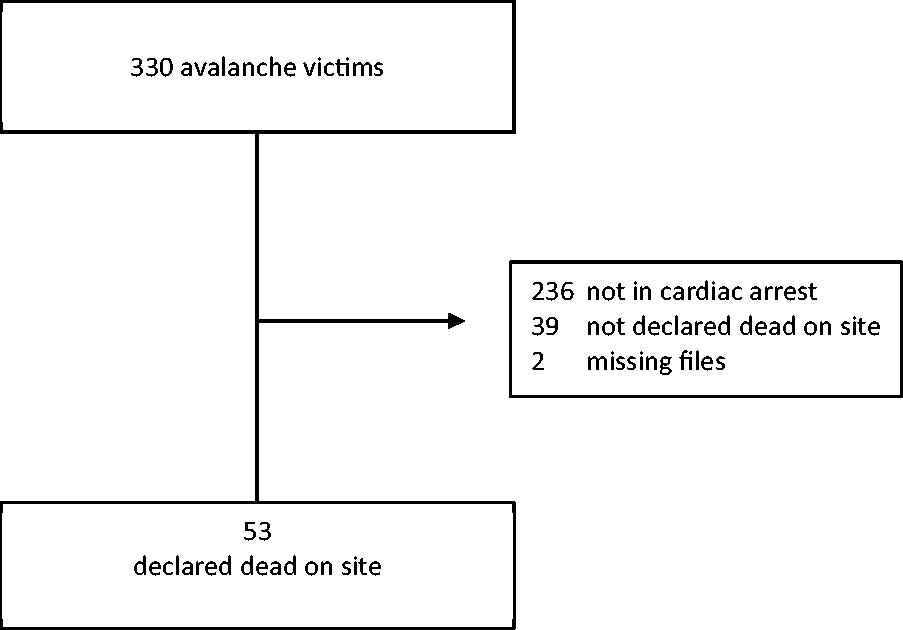
Flowchart of study patients. Critically buried avalanche victims who were declared dead on site. Swiss Air Ambulance Rega, 2010–2019.
Characteristics and Management of 53 Critically Buried Avalanche Victims who were Declared Dead on Site. Swiss Air Ambulance Rega, 2010–2019
Student’s t test.
Fisher’s exact test.
Wilcoxon (Mann–Whitney) test.
CA, cardiac arrest; CPR, cardiopulmonary resuscitation; IQR, interquartile range.
The relevance of the criterion, noncompressible chest wall, was assessed in six victims rescued after 2013. It was considered decisive in four victims and not decisive in two for whom other evaluations were done. The other sic victims were rescued before the introduction of the criterion in the guidelines.
Discussion
Only a minority (23%) of critically buried avalanche victims in CA and declared dead on site were reported as having noncompressible chest walls. Having a noncompressible chest wall was significantly associated with a longer burial duration and a lower core temperature than not having a noncompressible chest wall. Of the two processes inducing a noncompressible chest wall, i.e., postmortem rigidity and severe hypothermia, the latter is more likely in long burial (>60 minutes). The 60-minute burial duration is associated with the time when the core temperature is expected to drop below 30°C, the threshold below which the probability of hypothermic CA increases (Frei et al., 2019). The cutoff of 60 minutes of burial duration is indicative, as cooling rates have been reported to be between 0.6°C/h and 12°C in 50 minutes (Facchetti et al., 2014; Rauch et al., 2023). The time cutoff may be used for triage decisions if core temperature measurement is not available (Pasquier et al., 2023). Of 4,326 critically buried avalanche victims reported in one study, 3% (n = 140) had long burials (>60 minutes) (Eidenbenz et al., 2021). As regards the postmortem rigidity, its development is slowed in low ambient air temperatures, such as those encountered in an avalanche accident. The postmortem rigidity occurs later and lasts longer than at higher air temperatures (Schön et al., 2020).
Characteristics of the victims
With short burial durations, most avalanche victims experience CA caused by traumatic injuries or asphyxia. With long burial durations, the probability of undergoing CA secondary to hypothermia increases. The time limit after which hypothermia leads to irreversible death depends on the combination of weather, physiological, and insulation factors. It is different in every situation. No precise time cutoff can be established to distinguish a victim with a possibly reversible hypothermic CA from a dead victim. In this study, the shortest burial duration with a reported noncompressible chest wall was 410 minutes.
There is one report of an avalanche victim with unwitnessed CA who survived neurologically intact after hypothermia-induced CA with muscle rigidity. This victim was extricated after a critical burial of 5 hours. The rectal temperature was 19°C and the heart was described as “frozen stiff” by the cardiac surgeon after sternotomy (Althaus et al., 1982). In another case, the patient was in hypothermic CA, lying near a snowy mountain trail with drug intoxication. Muscle rigidity was present only in the jaw. (Bunya et al., 2018). These cases highlight that the difference between muscle rigidity secondary to hypothermia, a potentially reversible cause of CA, and postmortem rigidity cannot be distinguished, and that survival after rewarming has been reported.
Relevance of the criterion “noncompressible chest wall” on patient management
The criterion “noncompressible chest wall” first appeared in the guidelines that focused on accidental hypothermia in 2010 (Soar et al., 2010). It was later integrated in the avalanche management guidelines, which consider the presence of “lethal injuries or a whole body frozen” as the first criterion to assess at extrication of the victim that allows withholding or stopping CPR if present (Brugger et al., 2013; Lott et al., 2021; Van Tilburg et al., 2017).
In our study, since 2014, the proportion of avalanche victims with noncompressible chest walls was low, and the proportion of patients for which this criterion was assessed as decisive in declaring the death even lower.
The clinical assessment of a noncompressible chest wall in a prehospital setting may be difficult, may be subject to inter-rescuer variability, and could lead to undertreatment (absence of CPR and transport to an extracorporeal life support center for suspected hypothermic CA) if incorrectly assessed.
The presence of the criterion, noncompressible chest wall, does not appear to be sufficient to allow a rescuer to declare a critically buried avalanche victim in CA dead. This criterion was removed from the guidelines for management of avalanche victims in 2023 (Pasquier et al., 2023). The present study supports this decision. The changes in the recommendations over the years are summarized in Supplementary Data S2.
Perspective for future recommendations
In critically buried avalanche victims in CA with noncompressible chest walls, other clinical information should be sought to decide whether to pursue rescue efforts. Use of Doppler ultrasound has been proposed to assess the presence of orthograde flow in common carotid arteries in synchrony with chest compression during CPR with suspected noncompressible chest wall. Orthograde arterial flow is an indicator of compressibility of the chest wall (Blasco Mariño et al., 2023).
Future studies should focus on “pure” hypothermic CA, without the involvement of other potential CA etiologies like in avalanche victims.
Limitations
We retrospectively extracted the cases from a database that included avalanche victims rather than victims exposed to cold air. The number of patients with a noncompressible chest wall reported is small and may have been undereported in the medical records and therefore underestimated. We assessed if the criterion noncompressible chest wall was decisive only based on retrospective data. A prospective study could assess this point more reliably. Diagnostic tools are limited in a prehospital setting where only suspected diagnoses are reported and diagnostic uncertainty is high (Wohlgemut et al., 2023). Postmortem forensic analyses and autopsies were not conducted in avalanche victims to determine the primary cause of death.
Conclusions
A noncompressible chest wall is seldom reported in critically buried avalanche victims with CA. The burial duration for avalanche victims in CA with noncompressible chest wall is longer and the core temperature lower than for victims without noncompressible chest wall. It appears that a noncompressible chest wall cannot be used as the sole criterion for deciding whether to declare the death of a critically buried avalanche victim. Our findings support the removal of this criterion from the 2023 guidelines for the management of avalanche victims.
Footnotes
Acknowledgments
The authors thank Marlis Planzer from the Rega Center in Zürich for her help and assistance.
Authors’ Contributions
D.E.: Conceptualization; methodology; formal analysis; writing—original draft; visualization. A.K.: Data curation; writing—review & editing. P.-N.C.: Writing—review & editing. R.A.: Data curation; writing—review & editing. M.P.: Writing—original draft; supervision. K.Z.: Writing—review & editing.
Author Disclosure Statement
None to declare. None of the authors has any financial or personal relationships that could have influenced the work.
Funding Information
This research received no external funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.