
Abstract

Introduction
A
Eliane was the first to use a reduced conditioning regimen in patients suffering from Fanconi anemia (FA), resulting in improved outcome. The FA proteins help to maintain genomic stability during DNA replication, so bialleleic mutations in FA genes lead to bone marrow failure and susceptibility to acute myeloid leukemia, solid tumors, congenital abnormalities, and infertility (Auerbach, 2009). The FA proteins are also involved in the repair of DNA interstrand crosslinks. The bone marrow's high sensitivity to DNA interstrand crosslinking agents required an appropriate decrease in the doses of drugs used in the conditioning regimen. Thus, after some crucial in vitro studies (Berger et al., 1980), Eliane Gluckman introduced a new conditioning regimen (comprising low-dose cyclophosphamide and thoraco-abdominal irradiation) with improved outcomes for allotransplanted patients (Socie et al., 1998).
Some years later, I met Alain Fischer. He was using the knowledge acquired in CD18-deficient patients to set up a monoclonal-antibody-based protocol to block rejection by natural killer cells—the only circulating lymphocytes in some severe combined immunodeficiency (SCID) conditions, but which frequently cause rejection of a partially human leukocyte antigen (HLA)–mismatched transplant (Fischer et al., 1991). Eliane and Alain's work and ideas convinced me that personalized approaches to regenerative medicine might solve the immunological problems that occur in allotransplantation in particular settings. More than 20 years and several clinical protocols later, it is clear that this approach is the right one—even though there are still scientific and strategic obstacles to overcome.
Advances
When considering all the various cell and gene therapy protocols performed to date, gene therapy produced the most impressive advances. The key idea in treating inherited diseases of the hematopoietic system is simple: to replace the diseased bone marrow with autologous gene-modified cells in order to stably establish expression of the missing protein and thus restore its function.
In fact, conventional allogeneic stem cell transplantation still has to face a number of major obstacles if it is to be used successfully in all the patients who need it. The degree of HLA mismatch, the occurrence of graft-versus-host disease, uncontrolled severe opportunistic infections, and the time needed to build up a new adaptive immune system are today's greatest hurdles (Gennery et al., 2010; Moratto et al., 2011; Fernandes et al., 2012).
The use of autologous, gene-modified stem cells appeared to be a way of solving all these problems at once. Since 1999, around 70 patients affected by SCID-X1 or adenosine deaminase (ADA) deficiency have undergone gene therapy and have formally provided proof that this approach works (Aiuti et al., 2009; Hacein-Bey-Abina et al., 2010; Gaspar et al., 2011).
Briefly, SCID-X1 newborns achieved a stable immunological T cell compartment after the infusion of ex vivo-manipulated hematopoietic stem cells (HSCs). The time course of recovery was significantly shorter than that usually observed after a partially HLA-mismatched transplant. The newly developed T cells are functional, as evidenced by the clearing of the ongoing severe infections and the subsequent stable protection against infectious agents (with no need for other treatments). The newly generated T cells have a polyclonal repertoire. More than 14 years later, thymopoiesis is still ongoing—even in patients who subsequently developed leukemia.
Despite the absence of gene-corrected B cells in the treated SCID-X1 patients, some patients are still able to produce normal levels of immunoglobulins via γC-independent pathways. However, the development of memory B-cells and the persistence of a strong humoral response against recall antigens require the involvement of the γC-dependent cytokine IL-21, which is why these features are missing in these patients.
The development of full humoral responses and the long-term maintenance of normal levels of memory B-cells can only be obtained by conditioning before transplantation. Despite this caveat, genetic correction of the immunodeficiency greatly improved the patients' general health status and enabled them to lead a normal life.
Insertional Genotoxicity
The first SCID-X1 gene therapy trial also highlighted the significant toxicity associated with the LTR's strong enhancer effect on the murine leukemia virus (MLV)–based retroviral vector, which was responsible for five cases of leukemia in the two SCID-X1 trials. The onset of leukemia occurred 23–68 months after gene therapy. The disease was fatal in one patient but was cured in the four others (Hacein-Bey-Abina et al., 2008; Howe et al., 2008).
Despite the development of these severe adverse events (SAEs), the overall survival and event-free survival rates of this first cohort of 20 patients remained impressively high and challenged the results obtained in Europe and worldwide with partially HLA-mismatched donors—showing the power of this approach (Fig. 1) (Fernandes et al., 2012). The occurrence of these SAEs prompted an in-depth analysis of retroviral insertion sites, which was made possible by knowledge of human sequence and the availability of appropriate technologies (Schmidt et al., 2001; Schroder et al., 2002). Gamma retroviral vectors do not integrate randomly; each type of retrovirus follows a unique set of precise rules, explaining the biased pattern of integration sites observed in transduced human cells.
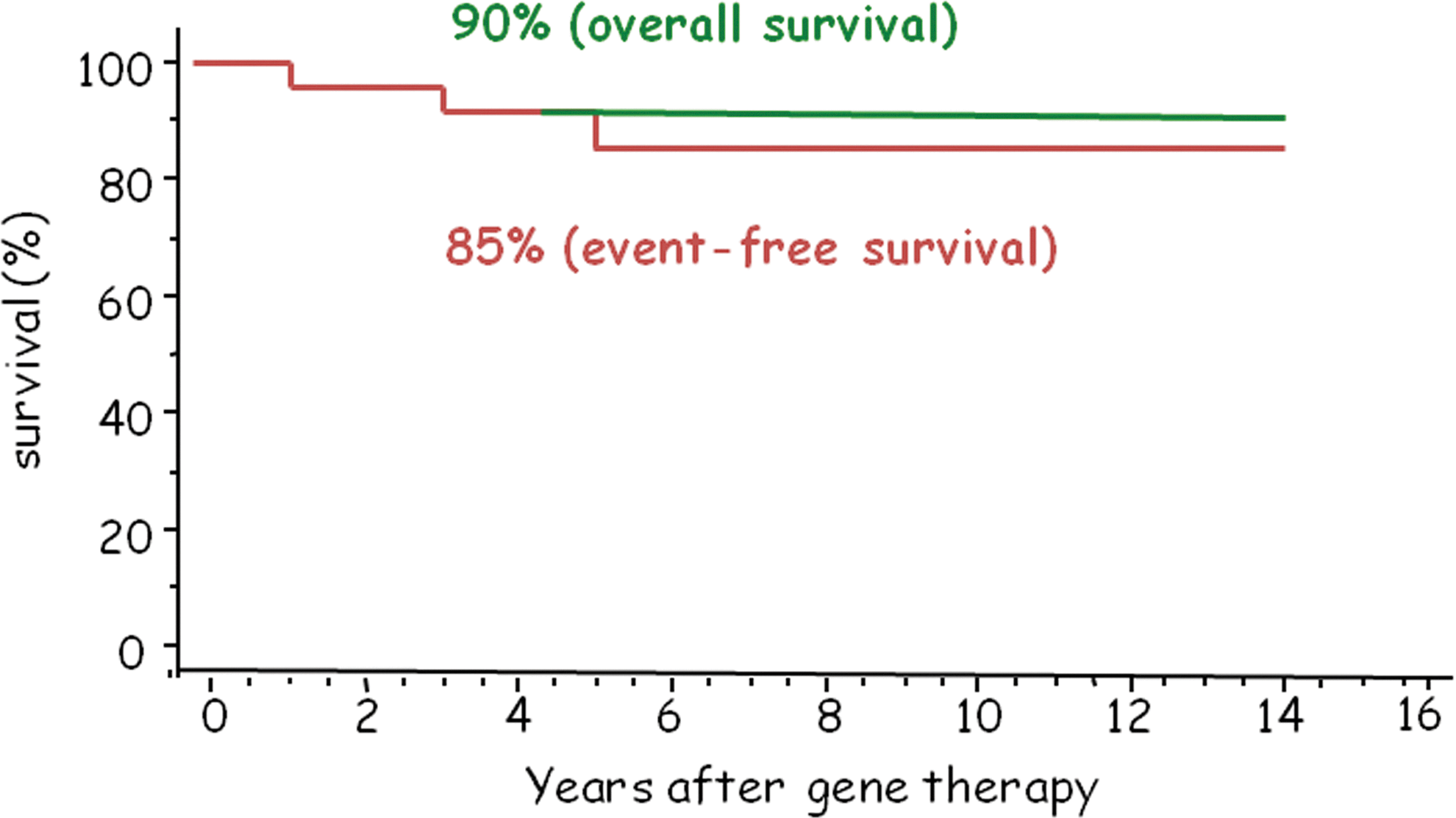
Overall and event-free survival rates in the 20 patients with SCID-X1 (Paris–London combined data). The curves represent the overall survival and the event-free survival of the 20 patients affected by SCID-X1 and treated in Paris and London. x-axis, years after gene therapy; y-axis, survival is expressed in percentage. The median follow-up is 12.5 years, ranging from 8 to 16 years.
The Moloney MLV and its derived vectors integrate preferentially in transcriptionally active promoters and regulatory regions. The vectors' integration pattern shows a characteristic clustering around enhancer and promoter regions associated with modifications of histones H3K4me3 and H3K9me1, which are involved in chromatin configuration and binding to RNA Polymerase II (Wang et al., 2010).
The insertional activation of proto-oncogenes by MLV-derived vectors caused not only T-cell acute lymphoblastic leukemia in the first clinical trials for SCID-X1 (Hacein-Bey-Abina et al., 2003; Howe et al., 2008) but also Wiskott–Aldrich syndrome and myelodysplastic syndrome in patients treated for chronic granulomatous disease (Stein et al., 2010; Avedillo Diez et al., 2011). The strong transcriptional enhancers present in the MLV-LTR likely had a major role in the mechanism of these SAEs; this observation thus allows the development of safer vectors.
Enhancer-less, self-inactivating (SIN) retroviral vectors with an internal weak promoter (capable of inducing limited and, in some cases, tissue-specific transcription of the therapeutic gene) have been created. In order to increase the safety of this procedure, the introduction of HIV-derived vectors constitutes a further step toward the prevention of insertional mutagenesis because they (i) do not target regulatory elements and (ii) randomly integrate into actively transcribed genes (without a preference for dangerous oncogenes) (Biffi et al., 2011; Moiani et al., 2013).
Two more years of patient follow-up are needed before we can say whether or not SIN-lentiviral vectors are significantly safer than the first-generation gamma retroviral vectors. Once this concern is solved, a number of questions on the use of gene therapy will remain. The most urgent issue is to determine how many vector copy numbers (VCNs) can produce a cure without inducing SAEs. Various VCNs have been detected in trials and there is not yet a clear answer to this question.
However, the genotoxicity of retroviral vectors is related to several factors other than vector design. These include nature of the target cells and the patient's genetic background. Hundreds of patients have been reinjected with millions of transduced mature T cells (Cieri et al., 2014) in the absence of insertional mutagenesis events. Furthermore, insertional mutagenesis events have not been observed in any of the 40 ADA-deficient patients treated up with a gene therapy protocol based on the use of first-generation MLV vectors has developed (Aiuti et al., 2009). Unfortunately, there are no animal models able to predict the risk of genotoxicity—despite huge efforts by several groups (Kustikova et al., 2005; Montini et al., 2009). In the absence of this type of animal model (which would enable us to move forward more rapidly), we can only proceed into the clinic with a high degree of caution.
The Target Cells
The target cell population is important in terms of both the genotoxic risk and the efficacy and long-term stability of the gene therapy procedure. In the hematopoietic system, the clinical gene therapy protocols' targets are CD34+cells. This is a highly heterogeneous population that encompasses not only stem cells but also multipotent progenitors and lineage-restricted cells. A number of factors influence the proportion of CD34+cells and their location inside the bone marrow: the patient's status (steady or stressed) and age, the cell source (cord blood or mobilized peripheral blood), and the underlying disease. Ideally, only CD34+lin− cells should be transduced, cryopreserved during quality testing, and then injected into the patients in “sufficient” quantity. The sufficient quantity has been defined through experience with autologous and allogeneic bone marrow transplantation. Results indicate that at least 3×106 nonmanipulated CD34+cells per kg body weight are needed to restore long-term hematopoiesis.
Of all the genetic diseases treated with gene therapy to date, the cell characteristics of the bone marrow and the most immature hematopoietic progenitors were similar to those of the normal counterpart in only two cases: X-linked adrenoleukodystrophy and metachromatic leukodystrophy (Cartier et al., 2009; Biffi et al., 2013). In all the other cases, major differences were present at the time of collection. These differences should have an impact on the number of HSCs that can be harvested and on the transduction efficiency.
In some forms of SCID, an elevated percentage of pro-B cells are present in the bone marrow at the time of collection (Noordzij et al., 2002, 2003; Lagresle-Peyrou et al., 2008). This percentage can be very high in SCID patients with ongoing opportunistic infections, which therefore dilutes the total number of CD34+lin− cells present.
Mobilization of beta-thalassemic patients with G-CSF alters the distribution of CD34+cells and induces the massive release of CD34+CD36+precursor cells into the circulation. The latter are primed toward the erythroid differentiation pathway and thus display reduced self-renewal capacity. Chronic inflammation processes (such as those characterizing HIV-1 infection and chronic granulomatous disease) can also modify the CD34 reservoir (Sauce et al., 2011) (Fig. 2).
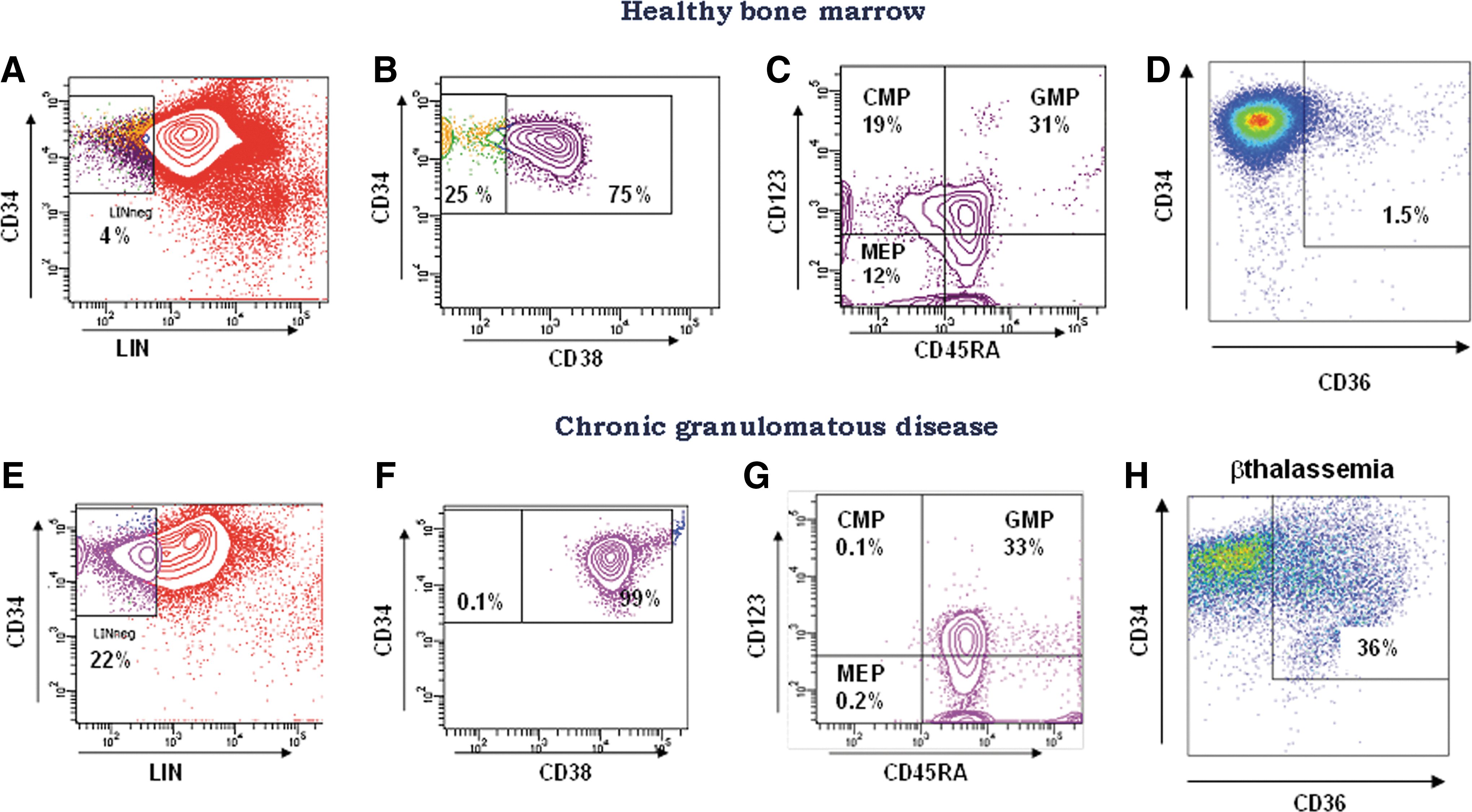
Representative staining for hematopoietic stem cells and precursor cells in a healthy control and in two diseased bone marrow samples. Flow cytometry analysis of mononuclear cells from healthy bone marrow
The Wiskott–Aldrich syndrome protein is a key regulator of cytoskeletal remodeling in all the hematopoietic cell compartments. Mutation results in reduced actin polymerization and immune system impairment, a low T cell count and impaired T cell chemotaxis, and cell migration. Mobilized hematopoietic peripheral cells from WASP-deficient patients may contain a high proportion of pro-B cells—probably because of the alteration in B cell homeostasis described in these patients. Moreover, these peripheral mobilized hematopoietic cells cannot be cryopreserved because of an excessively fragile cell membrane; this latter characteristic was discovered by Salima Hacein-Bey-Abina (in collaboration with Anne Galy, who then modified the clinical protocol accordingly).
Lastly, the fortunate absence of SAEs in the 40 ADA-deficient patients treated with a first-generation gamma retroviral vector suggests that as-yet-unidentified disease-related factors or differences in the bone marrow target cells influence the likelihood of adverse events. All these features must be taken into account during the preparation of cells for transplantation, in order to introduce disease-specific steps for the preferential correction of true HSCs. This field is progressing rapidly thanks to the required continuous, close, integrated collaboration between hematopoiesis researchers and experts in translational medicine at dedicated university hospital campuses.
Expected Progress
Since 2006 (the date of the first gene therapy clinical trial based on the use of a SIN HIV-1-derived vector), no mutagenic events have been observed with SIN gamma or lentivirus vectors. If these favorable results are maintained going forward, the greater safety of SIN vectors will have been formally demonstrated. The introduction of the lentiviral gene therapy vectors (with their greater capacity to accommodate genes and their tissue-specific transcription factors) has even enabled a patient with beta thalassemia to gain a transfusion-independent phenotype (Naldini et al., 1996; Pawliuk et al., 2001; Cavazzana-Calvo et al., 2010).
Thanks to this proof of principle, the gene therapy approach is no longer restricted to immunodeficiencies and can be used to treat a group of diseases that represents a worldwide health burden in millions of people who do not have access to either allogeneic bone marrow transplantation or even conventional supportive care (such as safe transfusion). Of course, this proof of principle requires further development if it is to provide transfusion independence to a βo/βo patient or a sickle cell anemia patient. This achievement is just around the corner, thanks to progress in HSC collection, manufacture of high-titer vector, and improvements in transduction efficiency.
Lastly, all the results obtained in gene therapy for inherited diseases can now be applied to the management of acquired diseases (such as HIV infection). The hematopoietic stem cell transplantation from an allogeneic donor with an HIV-resistant genotype (a result of a naturally occurring 32-base pair deletion in the gene encoding chemokine receptor 5 [Δ32 CCRS]) in conjunction with a full myeloablative conditioning regimen resulted in apparent elimination of HIV in a leukemia-affected recipient (Hutter et al., 2009). To date (more than 5 years later) the patient has not required any retroviral treatment and appears to be free of HIV infection (Allers et al., 2011; Yukl et al., 2013). This well-studied case provides the proof of principle that hematopoietic stem cells engineered to become HIV-infection resistant represent a powerful strategy against HIV, a pandemic infection, still with no cure.
Combining of Cell Therapy and Gene Therapy
Cell therapy and gene therapy are advancing together to improve patient care. We can expect to be able to rebuild a new immune system not only in primary immunodeficiencies but also in severe acquired clinical conditions (such as those in HIV-1-infected patients). Innovations in cell therapy (such as the generation of T cell in culture systems that mimic the thymic epithelium) are now ready to be transferred into the clinic and could provide HIV patients with a new compartment of HIV-infection-resistant T cells. The use of OP9-delta-1 and delta-4 reagents enables the generation of huge quantities of pro- and pre-T-cells that are capable of colonizing the empty thymus. Hence, these steps can now be performed in a Petri dish, rather than in the patient's diseased thymus (Awong et al., 2009).
By studying a murine model of immunodeficiency, Isabelle André-Schmutz has recently proved that the coinjection of nonmanipulated, cord-blood-derived CD34+cells and delta-4-expanded T cell progenitors has a synergic effect on T cell generation and on CD34 intake in the bone marrow—opening up new opportunities in the field of hematopoietic transplantation (Reimann et al., 2012).
A nongenotoxic conditioning regimen is a prerequisite for performing gene-modified autologous transplantation without the need for expensive controlled environment units and highly specialized teams of medical and nonmedical staff. In theory, a number of specific drugs and monoclonal antibodies are available, but unfortunately big pharma is not very keen to develop them for the so-called orphan applications (Czechowicz et al., 2007).
The use of “bone-marrow-specific drugs” to create the requisite space in bone marrow niches would mean that patients could be treated without the occurrence of toxic or infectious complications and could be hospitalized in a conventional ward for few weeks. Once the gene-modified stem cells had been injected, standard hospitalization for a few weeks would significantly decrease the global cost of treatment for the patient and society in general. Although major technical challenges in cell and gene therapy have been overcome after three decades of basic and translational research, a huge amount of work has yet to be performed before we can achieve this objective. We now need to enter a new era in which academic laboratories (capable of providing important fundamental discoveries and state-of-the-art know-how in cell therapy technology) must collaborate with biopharmaceutical companies that have the infrastructure for integrating these various advances and providing them to the patients in real time.
Footnotes
Acknowledgments
I thank the patients and staff of the Biotherapy Department and Immunological and Hematological Pediatric Service of the Necker Hospital in Paris, the reference center for hemoglobinopathies in Creteil, the Institut des Maladies Emergentes et des Thérapies Innovantes–CEA, and all the members of Unit 768–INSERM. I am particularly grateful to Prof. Salima Hacein-Bey-Abina and Dr. Isabelle André-Schmutz for the continuous constructive discussion and friendly support. I apologize to the authors of many relevant studies that I have been unable to cite because of the formatting constraints.
This work was supported by INSERM, Assistance Publique Hôpitaux de Paris, ANRS, AFM, the CELL-PID No. 261387, the ERC No. 69037, the Eurofancolene No. 305424, Net4CGD No. 305011, and The Imagine Institute.