
Abstract
Head and neck cancer represents the seventh most common cancer worldwide. Although multidisciplinary sequential treatments have been used, there is still an urgent need for new treatment approaches that can effectively improve the outcomes of patients with advanced stages of head and neck cancer. Gene therapy is a rapidly evolving field in cancer therapy that has been shown to improve the efficacy of antitumor treatment. China is at the forefront in clinical trials and practice of gene therapy. Chinese researchers have mainly focused on gene therapeutics based on oncolytic virus and recombinant adenovirus expressing p53, antiangiogenesis factor or herpes simplex virus-thymidine kinase. Currently, two gene therapy drugs, Gendicine and Oncorine, have been marketed in China, and a number of upcoming gene therapy agents are under development for the treatment of head and neck cancer. Most gene therapy agents have demonstrated excellent tolerance. However, the therapeutic effects need further improvement. With current innovations in tumor biology and knowledge, gene therapy has great potential as a safe and effective anticancer treatment. In recent years, new gene therapy agents with promising effects have been incorporated into clinical trials in China. Thus, gene therapy may become an important part of anticancer therapy and is expected to improve the therapeutic effect of head and neck cancers in the near future.
Head and neck cancer represents the seventh most common cancer worldwide. Although multidisciplinary sequential treatments have been used, there is still an urgent need for new treatment approaches that can effectively improve the outcomes of patients with advanced stages of head and neck cancer. Gene therapy is a rapidly evolving field in cancer therapy that has been shown to improve the efficacy of antitumor treatment. China is at the forefront in clinical trials and practice of gene therapy. Chinese researchers have mainly focused on gene therapeutics based on oncolytic virus and recombinant adenovirus expressing p53, antiangiogenesis factor or herpes simplex virus-thymidine kinase. Currently, two gene therapy drugs, Gendicine and Oncorine, have been marketed in China, and a number of upcoming gene therapy agents are under development for the treatment of head and neck cancer. Most gene therapy agents have demonstrated excellent tolerance. However, the therapeutic effects need further improvement. With current innovations in tumor biology and knowledge, gene therapy has great potential as a safe and effective anticancer treatment. In recent years, new gene therapy agents with promising effects have been incorporated into clinical trials in China. Thus, gene therapy may become an important part of anticancer therapy and is expected to improve the therapeutic effect of head and neck cancers in the near future.
Introdution
H
Gene therapy refers to treatments that introduce exogenous genetic material (DNA or RNA) into cells to treat or prevent diseases (Fig. 1). Among the clinical trials on gene therapy, about 64% have investigated treatment of malignant tumors, such as cancers of the head and neck, prostate, kidneys, lungs, breast, and skin. 11 Gene therapeutics in China are mainly based on adenoviral gene therapy systems, and two gene therapy drugs, Gendicine and Oncorine, have been on the market in China for more than a decade. Studies on the treatment of head and neck cancers performed in China are mainly focused on gene therapy on oncolytic virus and recombinant adenovirus expressing p53, antiangiogenesis factor or herpes simplex virus (HSV)-thymidine kinase (TK) (Fig. 2). Among the drugs that have been used in clinical trials, some have demonstrated excellent efficacy and safety.
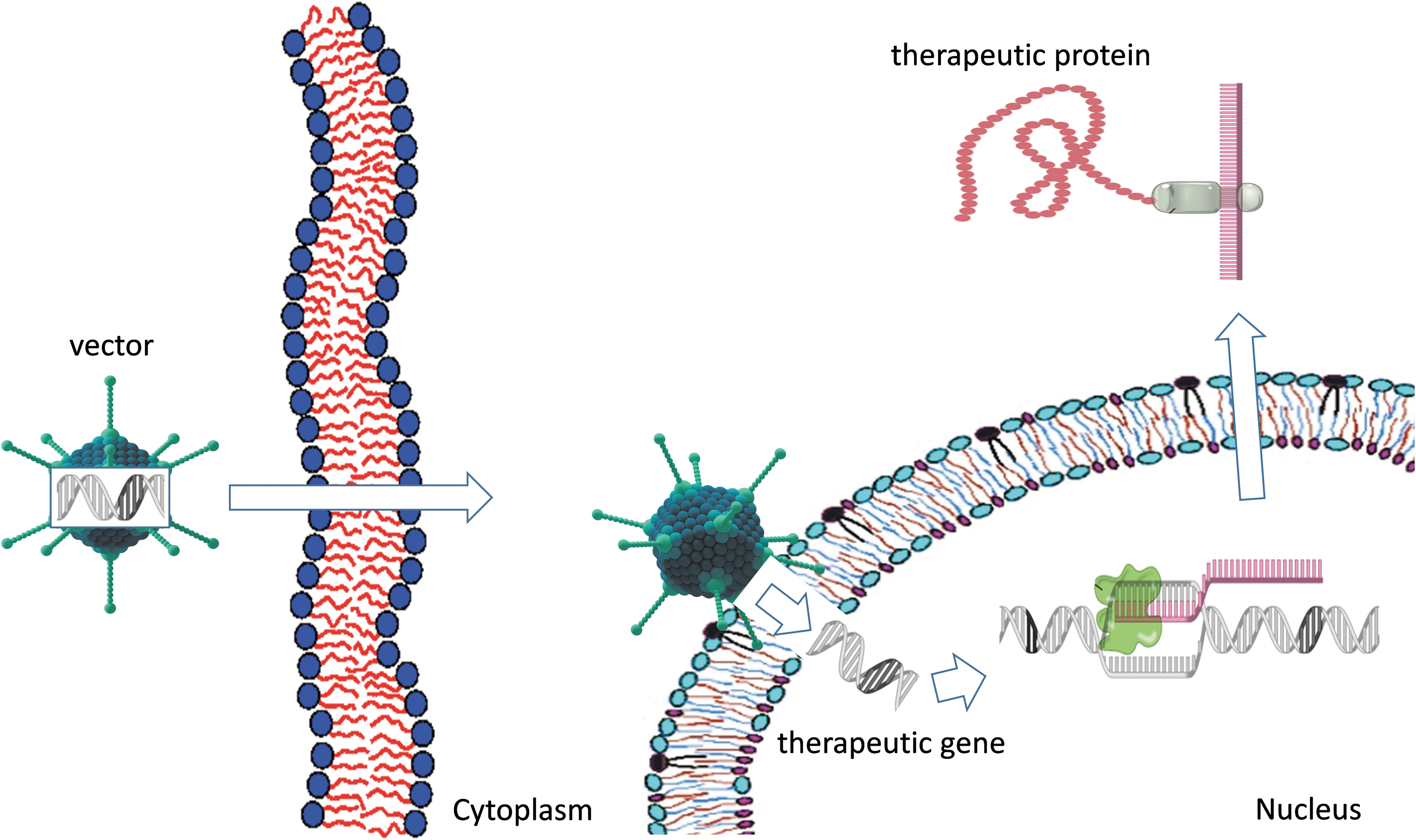
Gene therapy introduces genetic material into cells through virus vector, and continuously expresses the therapeutic protein.
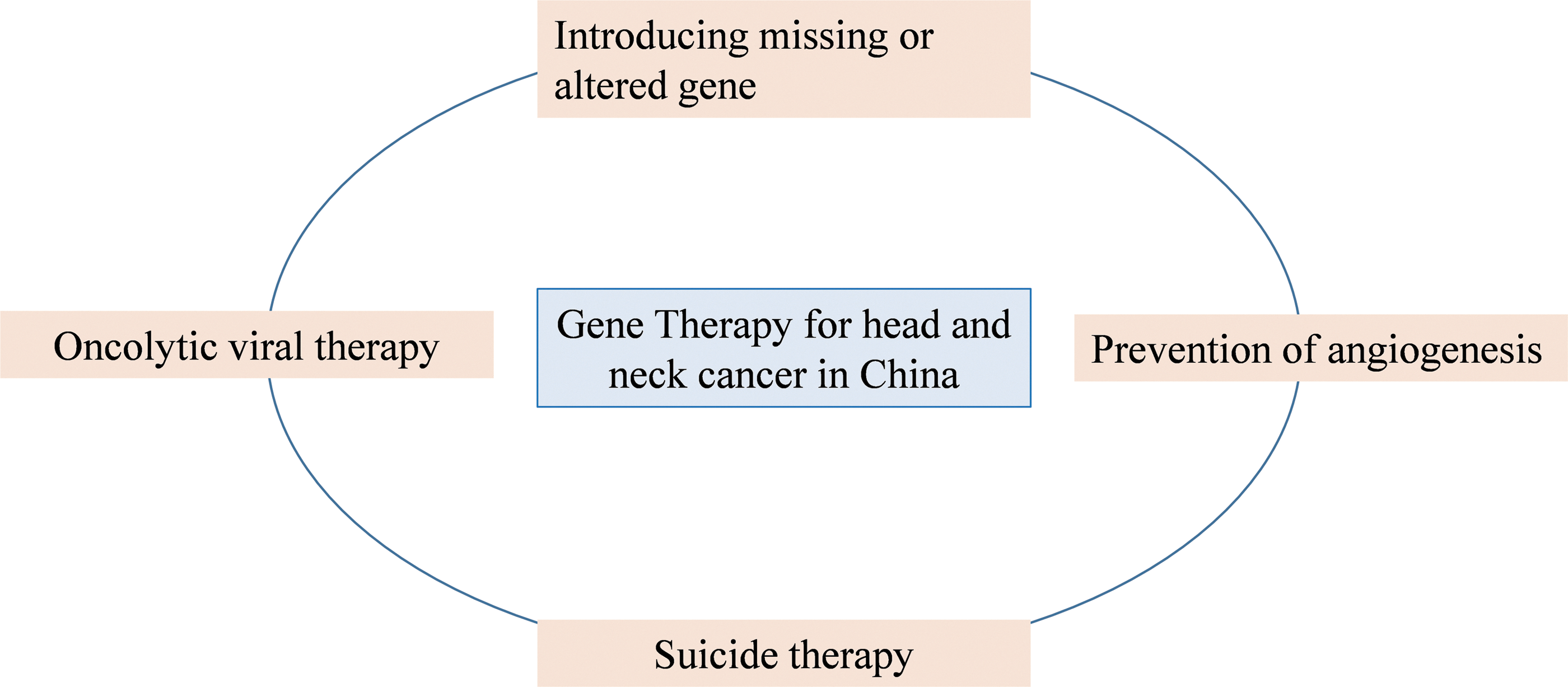
Strategies used in clinical trials of gene therapy in China for the treatment of head and neck cancer.
The present review aims to summarize the development and current status of gene therapy for head and neck cancer in China.
Introducing Wild-Type p53 Gene Into Cancer Cells
Gendicine
There are a number of gene therapy agents using rAd-p53 for cancer treatment, and clinical gene therapy programs have used rAd-p53 for the treatment of head and neck cancers in China since 1998. After completion of clinical trials, the first gene therapy treatment drug was approved for head and neck squamous-cell carcinoma by the China Food and Drug Administration (CFDA) on October 16, 2003. The next year, Gendicine officially entered the Chinese market. 12 Gendicine is a milestone, being the first gene therapy product for the treatment of cancer approved by a government agency in the world. 13 Although Western researchers in the field believed clinical trial results had not yet met the demand of the food and drug administration for approval and required further investigation and clinical data to satisfy concerns, Gendicine opened a window into the world of gene therapy treatment for cancer.
Gendicine is a recombinant human serotype-5 adenovirus that contains the wild-type tumor suppressor gene p53. After administration, Gendicine infects the targeted tumor cells by receptor-mediated endocytosis and then delivers the adenovirus genome carrying the therapeutic p53 into the cytoplasm and nucleus, leading to overexpression of genes encoding the p53 protein. The antitumor activity of p53 includes, among other functions, induction of apoptotic pathways, activation of immune response factors, inhibition of DNA repair and anti-apoptotic functions, downregulation of multidrug resistance gene expression to deter therapeutic resistance, vascular endothelial growth factor (VEGF) gene expression to block blood flow to tumors, and matrix metalloproteinase expression. 14 The adenoviral delivery vehicle is supposed to trigger and/or increase an immune response in patients. To do so, it may induce various nerve factors, hormones, and cytokines, according to the developer of Gendicine. 14 In a study by Peng et al., 14 infiltration of lymphocytes and inhibition of VEGF activity in tumor tissue of patients in clinical trials was observed after injection of Gendicine. However, Gendicine studies and information are very deficient in published English language literature.
In a Phase I clinical study from 1998 to 2000 in China, Han et al. 15 evaluated the efficacy and toxicity of Gendicine, which was called SBN-1 at that time. Twelve patients were enrolled and received intratumoral injection of Gendicine (1 × 1010, 1 × 1011, or 1 × 1012 viral particle doses) every other day for a course of five injections, and the treatment was performed for two cycles. Immunohistochemical examination of p53 levels in tumor tissues showed significant enhancement after treatment. Over the 3-year follow-up period, all enrolled candidates remained alive and cancer free. At the 2005 International Society for Cell and Gene Therapy of Cancer conference held in Shenzhen, China, Chinese researchers reported that 11 of the 12 head and neck squamous carcinoma patients in that trial were still alive at the end of November 2005, 6 years after the trial's onset. This demonstrates the promising effects of Gendicine for the treatment of head and neck squamous carcinoma.
In another Phase I Chinese clinical study, 16,17 administration of Gendicine in combination with radiotherapy was more effective at obtaining complete regression compared to radiotherapy alone. This multicenter randomized clinical trial of 135 patients with head and neck squamous-cell carcinoma showed that a combination of Gendicine, radiotherapy, chemotherapy, surgery, and hyperthermia treatment elicited significant beneficial synergistic effects. Of the enrolled patients, 77% had stage III–IV cancer and were not eligible for surgery or either radiotherapy or chemotherapy treatments were unsuccessful. Comparison of gene therapy combined with radiotherapy (GTRT) versus radiotherapy alone (control) resulted in a GTRT response rate of 93% compared to 79% in the control group. Radiotherapy doses (70 Gy) were administered in 35 fractions over 7–8 weeks, and Gendicine (1 × 1012 viral particles) was given 3 days before radiotherapy every week for a total of 8 weeks to the GTRT group. In the GTRT group, 64% of patients showed complete and 29% showed partial regression compared to 19% and 60% in the control group, respectively (p < 0.01). The complete regression rate in the GTRT group was threefold higher than that in the control group, suggesting that Gendicine in combination with radiotherapy has obvious beneficial synergistic effects. 14
Until 2006, >3,500 patients who received Gendicine in clinical practice in China had good outcomes. Besides head and neck squamous carcinoma, this treatment regimen also showed good therapeutic effects in other malignances, such as liver, breast, lung, and stomach cancers. However, these results were only published in Chinese language journals. In a later Chinese study, Gendicine was also shown to have a promising clinical effect in the treatment of dysplastic oral leukoplakia, which is the most common precursor of oral squamous-cell carcinoma. 18
In Chinese Gendicine studies, no serious adverse events have yet been reported. Patients in clinical trials conducted in China only exhibited common cold phenomena, such as self-limiting fever. However, Western researchers have obtained different results on the safety of this medicine, with many other gene therapy studies reporting serious adverse events. One patient died in a U.S. clinical trial in 1999, and two children developed leukemia in a clinical trial in France in 2003. As a result, a similar gene therapy named Advexin, which delivers p53 by adenovirus, was turned down by the U.S. FDA in 2008. 19 According to the developer of Gendicine (Dr. Zhaohui Peng [Shenzhen SiBiono GeneTech Co. Ltd., Shenzhen, China]), 14 the type-5 adenovirus vector used supposedly explains the greater safety of Gendicine. Adenovirus vectors are not known to integrate into the human genome to produce adverse effects. However, no relative data from clinical studies available support this hypothesis. Nonetheless, Gendicine has been widely used in China since its approval by the CFDA, and there have been no reports of serious adverse events to date.
Oncolytic Viral Therapy
Oncolytic viruses are a promising new therapeutic approach for malignant tumors. This approach employs viruses to replicate selectively inside tumor cells, enabling them to kill tumor cells specifically through lytic cell death during the normal progression of the virus life cycle. 20 These viruses can then amplify the oncolytic effect by infecting adjacent tumor cells. Several oncolytic viruses have been used in clinical trials in countries such as the U.S. and China and have shown positive therapeutic features and remarkable safety. Thus, they have become an ideal alternative treatment for many cancers.
The first oncolytic virus for cancer treatment that was tested in clinical trials (in the U.S.) is ONYX-015, also known as dl1520. ONYX-015 is a chimeric adenovirus vector carrying an inactivating deletion in the gene encoding the viral E1B-55 kD protein. 21 It is engineered to replicate in and lyse cells selectively with p53 deficiency. A study by McCormick et al. 22 showed that ONYX-015 preferentially replicates in and destroys p53-mutant cells. Moreover, preclinical studies conducted in the United States demonstrated that ONYX-015 also selectively replicates in tumor cells with intact p53. 23,24 Subsequent studies revealed that ONYX-015 can also kill tumor cells with a mutation in the upstream p14ARF pathway, which is a tumor suppressor that activates cellular p53 expression. 25 –27 This finding inspired studies of oncolytic viruses in China, and a number of oncolytic viruses have emerged for the treatment of head and neck cancers.
Oncorine
Oncorine is the first commercialized oncolytic virus approved by the CFDA in November 2005. 28 Oncorine, also known as H101, is an oncolytic adenovirus similar to ONYX-015. It carries an E1B deletion and is typically administered via intratumoral injection. Oncorine in combination with chemotherapy has been shown to be safe and effective in Chinese clinical trials on head and neck cancer, 29 –31 and was the first combination chemotherapy treatment approved for the treatment of nasopharyngeal carcinoma in China.
In a Phase I clinical study in China, 15 patients with malignant tumors were treated with 5 × 107 to 1.5 × 1012 Oncorine viral particles per day for 5 days. 29 The results showed that all patients tolerated intratumoral injection of Oncorine well, and no dose-limiting toxicity or serious adverse events were found in the course of treatment. The main side effects experienced were pain at the injection site and fever. Adenoviral DNA was not detected in the plasma, urine, oropharyngeal swabs, or swabs of the injection site of any patient. 29 In a Phase II Chinese clinical study, the efficacy and toxicity of intratumoral Oncorine injection in combination with chemotherapy was evaluated. 31 A total of 50 patients with malignant tumors in multiple centers were treated with 5 × 1011 Oncorine viral particles per day for five consecutive days every 3 weeks. The response rate was 28.0%, including three patients with complete regression and 11 patients with partial regression. The response rate of injected lesions was significantly higher than that of control (noninjected) lesions (p < 0.001). 31 A Phase III clinical trial in China conducted on 160 patients with head and neck or esophageal squamous-cell cancer compared the effects and toxicity of intratumoral Oncorine (H101) injection combined with cisplatin or Adriamycin chemotherapy plus 5-fluorouracil (PF or AF, respectively) versus PF or AF alone. 30 Intratumoral Oncorine injection doses included 5.0 × 1011 to 1.5 × 1012 viral particles per day for five consecutive days every 3 weeks, and all patients received at least two cycles of chemotherapy. Among 123 patients, the overall response rate in the H101 + PF group was 78.8% compared to 39.6% for PF alone. 30 These results demonstrated that intratumoral Oncorine injection combined with chemotherapy was significantly effective against squamous-cell cancer of the head and neck or esophagus. Moreover, administration of Oncorine was safe, with no serious adverse events.
In recent years, Oncorine was also used for the treatment of unresectable hepatocellular carcinoma and shown to benefit these patients when combined with transhepatic arterial chemoembolization. This combination treatment regimen was shown to improve overall and progression-free survival in a Chinese study. 32 Although it was approved for the market in China in 2005, Oncorine has not been approved by any other country to date. In 2015, the U.S. FDA approved an oncolytic viral therapy agent named IMLYGIC® for the treatment of melanoma, 33 representing the first oncolytic virus approved for clinical use in the United States.
H103 and KH901
After Oncorine, two other oncolytic viral agents, H103 (developed by Shanghai Sunway Biotech Co. Ltd.) and KH901 (developed by Chengdu Kanghong Biotechnology Co. Ltd.), were developed for the treatment of head and neck cancer in China and have been investigated in Chinese clinical trials. 20 H103 is an engineered oncolytic adenovirus armed to express heat shock protein-70 (HSP70) constantly in the tumor cells. In addition, the endogenous adenovirus E1a promoter of H103 was replaced by a cytomegalovirus promoter followed by insertion of HSP70, IRES, E1a, and poly A genes in the recombinant virus. HSPs are known to chaperone a broad repertoire of tumor antigens to antigen presenting cells. Thus, use of HSPs is believed to be a promising avenue in cancer treatment. HSP70 is continuously expressed after administration of H103 to lyse cancer cells and stimulate the innate immune response against them simultaneously. A preclinical study conducted in the United States showed that intratumoral inoculation with H103 can inhibit both primary and metastatic tumors in animal models. 34 The antitumor effect of H103 is thought to be mediated through the combined effects of its viral oncolytic activity and HSP70-mediated immune response against tumor antigens. 34
H103 was approved to enter Phase I clinical trial in China in June 2003; this trial included 27 patients with advanced solid tumors and examined H103 dose escalation. 35 H103 was injected intratumorally in doses ranging from 2.5 × 107 to 3.0 × 1012 viral particles, and the maximum tolerated dose of H103 was not defined. Common adverse events included fever, mild injection-site reaction, leucopenia, lymphopenia, thrombocytopenia, and hypochromia. Two patients developed dose-limiting toxicities of grade III fever with the 1.5 × 1012 viral particle dose and transient grade IV thrombocytopenia with the 3.0 × 1012 viral particle dose. The objective response to H103-injected tumors was 11.1%. Meanwhile, transient and partial regression of distant tumors in three patients who were not injected with H103 was observed. These results demonstrate that intratumoral administration of H103 is safe and has promising antitumor activity. However, further investigations are still required.
KH901 is a conditionally replicating oncolytic adenovirus that selectively replicates in tumor cells and expresses granulocyte macrophage colony-stimulating factor (GM-CSF). 36,37 Addition of exogenous GM-CSF into the oncolytic viral genome was intended to stimulate the host immune response, thereby enhancing the antitumor effect. KH901 was approved for clinical trials by the CFDA on March 18, 2005. In the Chinese Phase I clinical trial, safety, feasibility, and biological activity of intratumoral KH901 injection were tested in patients with recurrent head and neck cancer. 37 Thirteen patients received a single injection of KH901 containing 3 × 1011 (n = 3), 1 × 1012 (n = 3), 3 × 1012 (n = 4), and 1 × 1013 (n = 3) viral particles. Eleven patients received multiple doses; five patients received a total of six injections of 1 × 1012 viral particles twice per week, and six were injected with 3 × 1012 viral particles instead. Overall, KH901 treatment was well-tolerated. Main toxicity issues included flu-like symptoms, anemia, injection-site pain, and inflammation. Dose-limiting toxicity was not reached in the study. High levels of GM-CSF were detected in the circulation of all single-dose patients 12 h after injection but became undetectable 15 days after administration. Copies of KH901 were detected in the urine, but little was found in the feces. These results demonstrate that the virus replicated successfully. As intratumoral administration of KH901 was well-tolerated and expression of GM-CSF was observed, a Phase II clinical trial of KH901 intratumoral injection combined with standard chemotherapy was initiated in China. However, details of the results from this trial have not yet been reported.
Recombinant Human Endostatin Adenovirus
Angiogenesis is crucial for the growth, invasion, and metastasis of malignant tumors. Folkman et al. 38 revealed that endostatin, an endogenous angiogenic inhibitor derived from collagen XVIII, had antitumor activity. Endostatin suppresses VEGF-stimulated endothelial cell proliferation, migration, and tumor angiogenesis. Furthermore, administration of endostatin has low toxicity and did not result in drug resistance. 39 In the last two decades, Chinese researchers have developed gene therapy strategies using a recombination of replication-deficient adenovirus vectors containing the endostatin gene. These vectors continuously express endostatin protein in host cells to create an enduring therapeutic effect. One of these vectors, E10A, has shown promising therapeutic effects and has entered into clinical trials in China.
E10A
E10A was developed by Guangzhou Double Bioproducts Co. Ltd. (Guangzho, China). This agent is a type-5 recombinant replication-deficient adenovirus vector carrying the human endostatin gene. It can directly introduce the endostatin gene into tumor cells and continuously expresses endostatin protein to limit vascularization. 40,41 Intratumoral injection of E10A to nasopharyngeal carcinoma, gastric cancer, and hepatocellular carcinoma in animal models has shown increased levels of endogenous endostatin protein after administration with a longer half-life, as well as significant inhibition of tumor growth. 42 –44
In 2007, a Phase I clinical trial conducted in China showed that E10A had no dose-limiting toxicity after weekly intratumoral injection of doses ranging from 1 × 1010 to 1 × 1012 viral particles. 45 Higher levels of endostatin expression were detected throughout the period of treatment, and no neutralizing anti-adenovirus antibodies were detected. E10A was detected in the blood, throat, and injection site of patients but rarely in the urine and feces. 46 In a multicenter randomized Phase II clinical trial conducted in China, 140 patients with locally advanced or metastatic head and neck squamous-cell or nasopharyngeal carcinoma who were not considered suitable for surgery or radiotherapy were consecutively enrolled. 39 The objective response rate (ORR) was 29.9% in the control group versus 39.7% in the E10A group (p = 0.154). However, administration of E10A showed different therapeutic effects in subgroups of patients with head and neck squamous-cell and nasopharyngeal carcinomas. The ORR for nasopharyngeal carcinoma patients was 44.4% in the E10A group versus 40.6% in controls (p = 0.487), and 36.5% for E10A patients versus 20.0% in controls with head and neck squamous-cell carcinoma (p = 0.090). Although the response to E10A treatment was somewhat better in head and neck carcinoma patients, the difference between the two cancer types was not statistically significant. Patients who previously received chemotherapy had an ORR of 44.8% compared to 22.6% in the control group (p = 0.06), and patients injected with E10A who received three to four treatment cycles had significantly better objective (p = 0.014) and overall (p = 0.026) responses than controls. The overall disease control rate was significantly higher in the E10A group (92.6%) versus the control (80.6%; p = 0.034). The median follow-up of patients was 10.47 months, and the median progression-free survival was 3.60 and 7.03 months in control and E10A groups, respectively. The progression-free survival of patients given chemotherapy and E10A showed a 3.43-month improvement, and the hazard ratio of progression was significantly lower in the E10A group versus the control. These clinical trial results on E10A therapeutic efficacy were not as satisfying as expected, although it was shown to be safe. 39 E10A is currently in a Phase III clinical trial in China, but the data have not yet been disclosed.
Suicide Therapy
AdV-TK
AdV-TK is an engineered recombinant replication-incompetent adenoviruses vector containing HSV-TK. HSV-TK is a suicide gene commonly used in clinical trials of gene therapy. The protein product of HSV-TK is an enzyme that converts the nontoxic antiviral drug ganciclovir (GCV) into a highly cytotoxic phosphorylated form. 47 Moreover, the HSV-TK/GCV system also exhibits a bystander effect and induces antitumor immune responses within the human body. 48,49
AdV-TK was developed by Shenzhen Tiandakang Gene Engineering Co. Ltd. (Shenzhen, China), and has entered clinical trials in China. In a Phase I Chinese clinical study, the safety and efficacy of AdV-TK intratumoral injection followed by systemic administration of GCV was investigated in 18 patients with head and neck cancer and other malignancies. 49 AdV-TK was injected with a dose-escalation format starting with 2.5 × 1011 to 1 × 1012 viral particles on day 1. Then, 5 mg/kg of GCV was injected intravenously every 12 h from day 2 to day 15. The most common treatment-related toxicities were transient fever and reaction at the injection site. Anti-adenovirus antibody levels increased continuously during treatment, while anti-HSV antibody levels remained stable. These results demonstrated that AdV-TK followed by GCV is safe for cancer patients and has few environmental effects. 49
Another clinical study in China evaluated the effect of AdV-TK/GCV and photodynamic therapy for treatment of oral cancer. 50 Ten patients were injected with the hematoporphyrin derivative and irradiated with the corresponding laser frequency, and AdV-TK was injected locally into the tumor. Clinical efficacy after infusing veins with GCV was assessed by the imaging and hemodynamic analyses. After administration, the tumors showed clear shrinkage or were completely eliminated. 50
Conclusions
In China, a number of new agents of gene therapy are being developed for the treatment of head and neck cancer. Gene therapy is a newly established cancer treatment strategy with promising medicinal products available for new drug applications. Most clinical trials conducted in China have demonstrated that multiple gene therapy agents can improve antitumor treatments. Although initial successes have been seen, gene therapy is still in its infancy and requires further research and development. A significant advantage to gene therapy is its low toxicity compared to traditional anticancer therapies. However, it is unfortunate that investigation of its therapeutic effects have not yet met the expectation of investigators worldwide. Understanding of the molecular targets and environmental interactions of different gene therapies in cancer remains limited and has hindered further development of related medical technologies. As knowledge related to tumor biology grows, accelerated growth in new drug developments for gene therapy is anticipated. A review of early gene therapy studies in China revealed that most of the randomized controlled clinical trials were not conducted in compliance with standard Good Clinical Practice guidelines, and trial protocols and study designs have not been accounted for effectively. Nonetheless, China has now established a more mature system of clinical trials compared to practices in the past decade, and researchers are making progress in pursuing new technological innovations to combat cancer with gene therapies that aim to repair or replace abnormal genes, promote host immunity and/or cancer cell apoptosis, block angiogenesis, and much more. It is believed that increasing discoveries of new drug agents of gene therapy will emerge as an important part of anticancer treatment.
Footnotes
Acknowledgments
This work was supported by the Project of Science and Technology Commission of Shanghai Municipality (grant nos. 10410711200, 08140902100, 11495802000, 14DZ1941400, and 14DZ1941402) and the National Key Research and Development Program (grant no. 2016YFC0905003,5000).
Author Disclosure
All authors declare no conflicts of interest.