
Abstract
Clinical trials of adeno-associated virus (AAV)-based gene therapy have made remarkable progress in recent years. We aimed to perform a systematic review and meta-analysis of the literature to assess the efficacy and safety of AAV-based gene therapy for hemophilia. We systematically searched the Web of Science, Embase, PubMed, and the Cochrane Database of Systematic Reviews databases, for clinical trials involving patients diagnosed with hemophilia and treated with AAV-mediated gene therapy. Data on the annualized bleeding rate (ABR), annualized infusion rate (AIR), the incidence of treatment-related adverse events (TRAEs), severe adverse events (SAEs), and alanine aminotransferase (ALT) elevation were extracted as our outcomes. A total of 12 articles from 11 clinical trials were selected from 868 articles for meta-analysis. Pooled analyses showed that AAV-based gene therapy in hemophilia patients reduced the number of bleeding events and the number of factor infusion events by an approximate average of 7 per year and 103 per year, respectively. Eighty percent, 18%, and 63% of hemophilia patients had elevated TRAE, SAE, and ALT levels, respectively. Moreover, subgroup analysis found a significant reduction in ABR and AIR 2–3 years after the therapy. Additional findings that were not pooled including coagulation factor activity are presented in the accompanying tables. Our analysis supported the efficacy and safety of AAV-mediated gene therapy for hemophilia, providing evidence for its application as a therapeutic option for widespread clinical use in hemophilia patients in the future.
INTRODUCTION
Hemophilia is a bleeding disorder resulting from a genetic mutation. It is classified into three subtypes according to which clotting factor is deficient, namely hemophilia A (factor VIII deficiency), hemophilia B (factor IX deficiency), and (rarely) hemophilia C (factor XI deficiency). 1 Since hemophilia is an X-linked recessive disorder, it occurs almost exclusively in males, although female heterozygous carriers may present with reduced coagulation factor levels and mild symptoms. 2 Hemophilia A and B represent the most prevalent and widely recognized types of hemophilia, manifesting shared disease pathophysiology and clinical management principles, which served as the focal point for this study. 1,3
According to reports from >100 countries, the incidence of hemophilia A and B is estimated at 12.8 and 2.7 per 100,000 males, respectively, in high-income countries, and 6.6 and 1.2 cases per 100,000 males, respectively, in low-income countries. 4,5 Severe hemophilia causes spontaneous bleeding in joints and muscles, potentially leading to synovitis, arthropathy, and musculoskeletal complications. 6 Currently, the principal treatment for hemophilia is clotting factor replacement. However, this approach is limited due to immunogenicity issues, complications, and the need for frequent injections, which negatively impact patients' quality of life. 7 Therefore, researchers are actively pursuing more effective, durable, and safer treatment methods.
Over the past few decades, gene therapy research has predominantly focused on the potential for effective supplementation in cases of mutant coagulation factors using a singular gene delivery product. 8 In particular, adeno-associated virus (AAV) vectors, initially identified as impurities in adenovirus preparations, are garnering increasing attention among researchers. 9 AAVs have been extensively studied as gene therapy vectors. They belong to a family of parvoviruses that have a single-stranded DNA genome within their protein shell and rely on coinfection with other viruses to replicate. 10 Since numerous clinical trials have utilized AAV-based gene therapy to treat hemophilia patients, a promising treatment model has already been established. 11 –13
Several trials, including GENEr8-1, HOPE-B, and B-AMAZE, have reported increased factor activity, reduced bleeding episodes, and decreased dependency on factor replacement after AAV-mediated factor gene therapy. 14 –16 However, limited sample sizes, diverse treatment methods, and nonrandomized designs might have led to evaluation bias and an incomplete understanding of the efficacy and safety of this therapy.
As yet, no meta-analysis has comprehensively assessed the benefits of AAV-based gene therapy in hemophilia patients. Thus, we conducted a systematic review and meta-analysis of published studies to synthesize data on the safety and efficacy of AAV-based gene therapy for hemophilia to bridge this research gap. Our analysis provides substantial evidence for the recommendation and clinical use of AAV-based gene therapy for hemophilia treatment.
METHODS
Search strategy and study selection
On August 1, 2023, we systemically searched Embase, PubMed, Web of Science, and the Cochrane Database of Systematic Reviews databases using search terms related to “gene therapy,” “hemophilia,” “adeno-associated virus,” and “AAV” without language restrictions. Furthermore, we evaluated the reference lists of the identified articles and implemented a meticulous selection process to identify the most pertinent studies. Our study was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis 2020 statement (Supplementary Table S1), and was prospectively registered in PROSPERO (CRD42023434449). 17 All identified studies were independently screened for relevance by two investigators.
Further elaboration on the search methodology is detailed in Supplementary Table S2. Eligible studies included clinical trials involving patients aged >18 years who were diagnosed with hemophilia and treated with AAV-mediated gene therapy. Meta-analyses, review papers, guidelines, commentaries, and secondary articles were excluded. Articles that did not involve gene therapy for AAV and that had no data in the text that could be used for merging, or where the type of study was not a clinical trial, were excluded. Furthermore, studies with small population size (<5) were also excluded.
Data extraction
Data extraction was independently performed by two researchers by the predefined eligibility criteria. Discrepancies were resolved through a deliberation process involving a third researcher until a consensus was reached. The extracted data included the following: NCT number, first author, publication year, study design, sample size, serotype, and production platform, dose, age, follow-up duration, data cutoff date, primary endpoint, annualized bleeding rate (ABR), annualized infusion rate (AIR), treatment-related adverse events (TRAEs), severe adverse events (SAEs), and alanine aminotransferase (ALT) elevation.
Quality assessment
The quality of the observational studies was independently evaluated by two researchers using the methodological index for nonrandomized studies (MINORS). 18 The MINORS tool comprises a total of 12 items, of which the initial 8 are exclusively concerned with noncomparative studies and aim to assess the methodological quality of nonrandomized clinical research. These 8 items are evaluated using a scoring system (0, not reported; 1, reported but inadequate; or 2, reported and adequate), with an ideal score of 16 for noncomparative studies. Disagreements were resolved through discussion by a third researcher.
Data synthesis and analysis
Stata version 12.0 and 15.0 software were utilized for conducting a meta-analysis combining continuous and dichotomous variables, and the data were presented as the weighted mean difference (WMD) and risk ratio, respectively. WMD refers to AAV-based gene therapy in hemophilia patients, which reduces the approximate average number of bleeding events and infusion factor events per year. The Cochran Q test was used for heterogeneity analysis to identify statistically significant heterogeneity across the included studies, and the I 2 statistic (range: 0–100%) was employed to quantify the degree of the observed heterogeneity.
A moderate heterogeneity level was defined as p < 0.1 and I 2 > 50%. We utilized a funnel plot and Egger's test to investigate potential publication bias and the trim and fill analysis to adjust for studies with publication bias. In cases where summary outcome data were not reported, we extracted the outcome data based on distinct cohorts and assigned them the corresponding labels. We performed subgroup analyses based on different hemophilia types including hemophilia A and hemophilia B, as well as follow-up period. The study characteristics and results are presented in tables and figures.
RESULTS
Literature search
Figure 1 shows a flowchart of the systematic methodology used to conduct the literature search and subsequent selection in our meta-analysis. The literature search was performed on August 1, 2023, and a total of 868 articles were identified. Through a thorough literature search, 5 articles each were obtained from the Cochrane Database of Systematic Reviews (97 articles), PubMed (213 articles), Embase (257 articles), and Web of Science (298 articles), respectively, and 3 articles were physically retrieved.
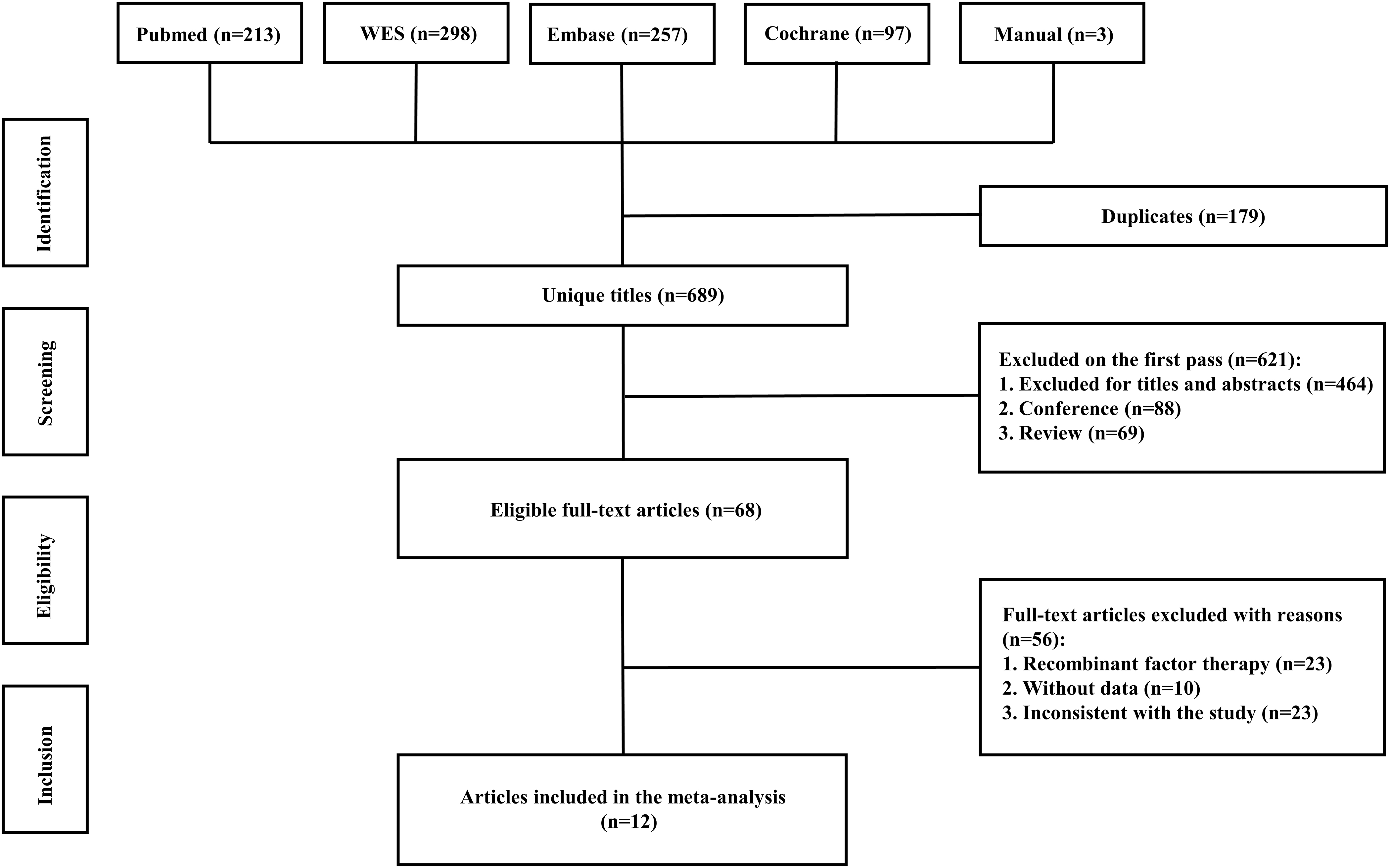
Flowchart of the systematic literature search and selection process.
After eliminating duplicate publications, 689 studies were reviewed based on their titles and abstracts. Of them, 621 were eliminated after the first screening, and then the full-text versions of the remaining 68 studies were assessed. Finally, we included a total of 12 articles derived from 11 clinical trials in our study. 11 –16,19 –24
Study characteristics
The pertinent characteristics of the 12 incorporated studies, which were published between 2014 and 2023, are detailed in Supplementary Table S3. These single-arm studies, which encompassed a total of 280 patients, employed a variety of >5 diverse vector types and administered over 10 distinct dosages of AAV-based therapies. The MINORS tool was employed to evaluate the quality of the incorporated studies, revealing a favorable overall standard (median, 13; range, 12–16). Supplementary Table S4 details the outcome of the qualitative appraisal.
Efficacy of AAV-mediated gene therapy
ABR data reported in eight articles were used for pooled analysis, which was derived using the following formula: (number of bleeding events/total number of days) × 365.25. The total number of days refers to the duration of follow-up before and after the study treatment of hemophilia patients with AAV-based gene therapy. A random-effects model was chosen due to significant heterogeneity (I 2 = 69.9%, p < 0.001). The results of the analysis indicated a pooled WMD of −7.35 (95% confidence interval [CI]: −10.40 to −4.30) (Fig. 2A). Further analysis examined the WMD concerning different types of hemophilia.
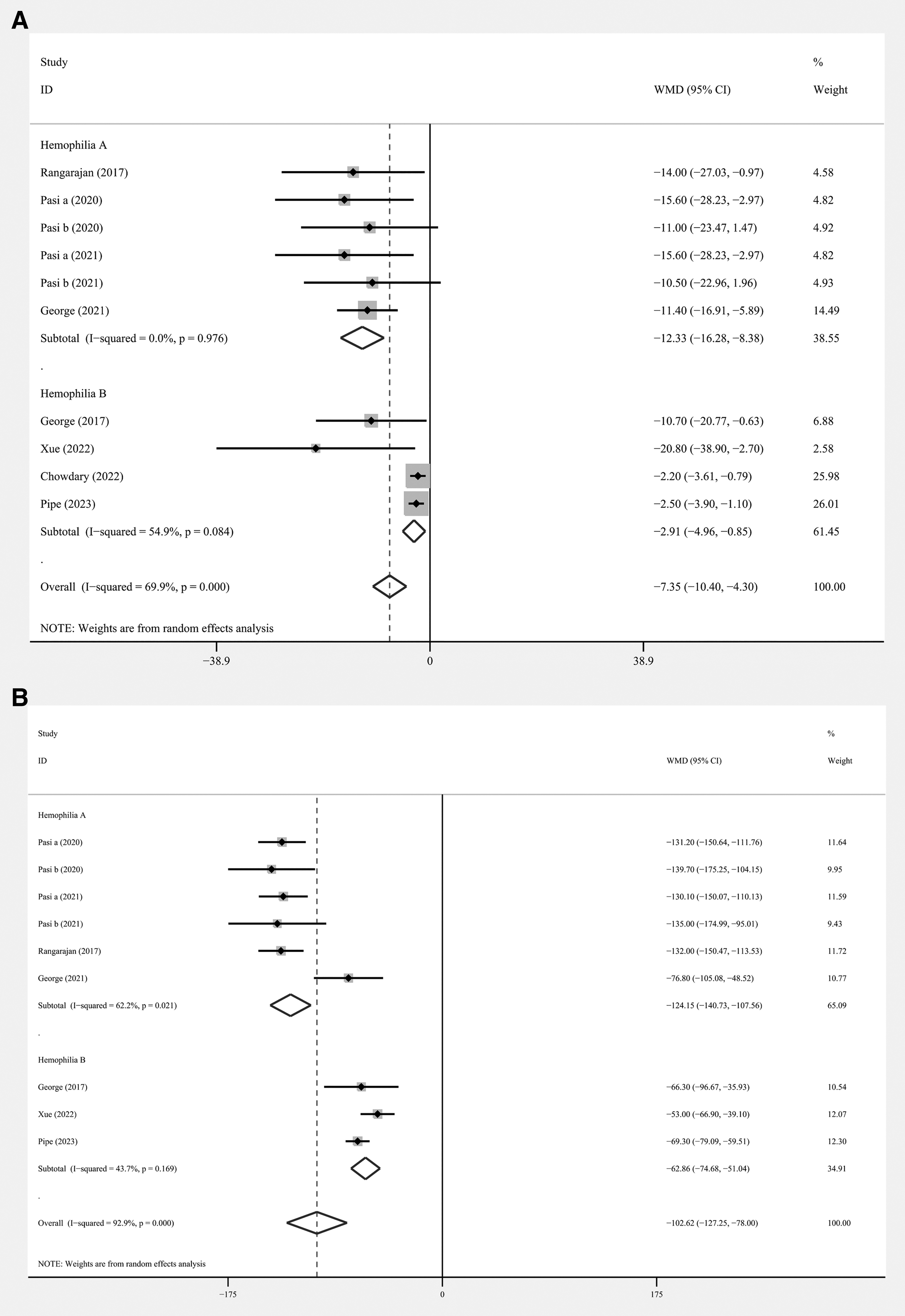
Forest plots of the effect of AAV-based gene therapy on
Subgroup analysis demonstrated that the pooled WMD in hemophilia A patients was −12.33 (95% CI: −16.28 to −8.38), while it was −2.91 (95% CI: −4.96 to −0.85) in hemophilia B patients. The AIR of Factor VIII or IX was calculated as follows: (total number of infusions administered during a specific time frame/duration in days) × 365.25. The duration in days pertains to the period of observation both before and after the administration of AAV-based gene therapy in the treatment of hemophilia patients. Seven articles provided data on AIR, and the summary AIR was −102.62 (95% CI: −127.25 to −78.00), with significant between-study heterogeneity (I 2 = 92.9%, p < 0.001) (Fig. 2B).
Subgroup analysis revealed that hemophilia B patients had a lower pooled WMD of −62.86 (95% CI: −74.68 to −51.04), whereas hemophilia A patients had a higher pooled WMD of −124.15 (95% CI: −140.73 to −107.56). Furthermore, our subgroup analysis based on the follow-up duration of patients after vector infusion revealed that AAV-based gene therapy significantly reduced ABR (WMD = −8.79, p = 0.001) and AIR (WMD = −115.68, p = 0.003) in hemophilia patients after 2–3 years of treatment and also significantly reduced AIR (WMD = −89.61, p < 0.001) in patients after 1 year of treatment (Fig. 3).
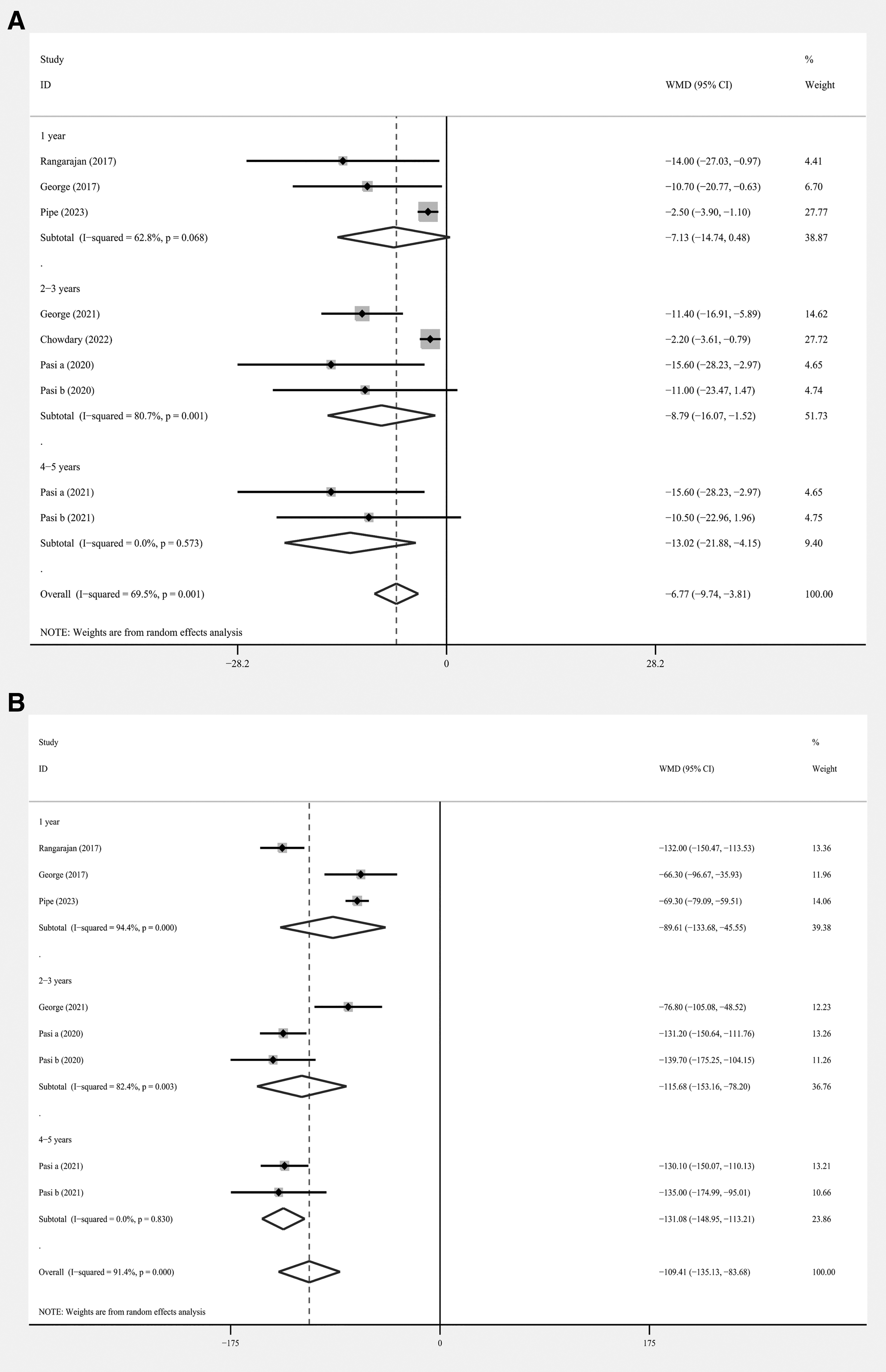
Forest plots of subgroup analyses of the effect of AAV-based gene therapy on
Supplementary Table S5 presents a comprehensive overview of the ABR and AIR results before and after gene therapy administration through AAV in hemophilia patients, along with the percentage reduction observed in their mean values. Both AIR and ABR were substantially reduced after gene therapy, with AIR decreasing by >95% in the vast majority of studies and ABR decreasing by >90% in most cases, except in a few studies. Supplementary Table S6 presents a comprehensive overview of factor VIII or factor IX activity before and after gene therapy through AAV in hemophilia patients, and an overview of the follow-up period in the eight studies. Generally, the intervention markedly improved factor VIII or factor IX activity.
Safety of AAV-mediated gene therapy
We analyzed the TRAEs and SAEs associated with AAV-based gene therapy for hemophilia. The pooled data revealed the incidence of TRAEs as 0.80 (95% CI: 0.67 to 0.91), with significant heterogeneity (I 2 = 81.87%, p < 0.01), while that of SAEs was 0.18 (95% CI: 0.10 to 0.26), also with significant heterogeneity (I 2 = 55.05%, p = 0.02) (Fig. 4A, B). In hemophilia A, the incidence of TRAEs and SAEs were 0.94 (95% CI: 0.90 to 0.97) and 0.15 (95% CI: 0.10 to 0.19), respectively.
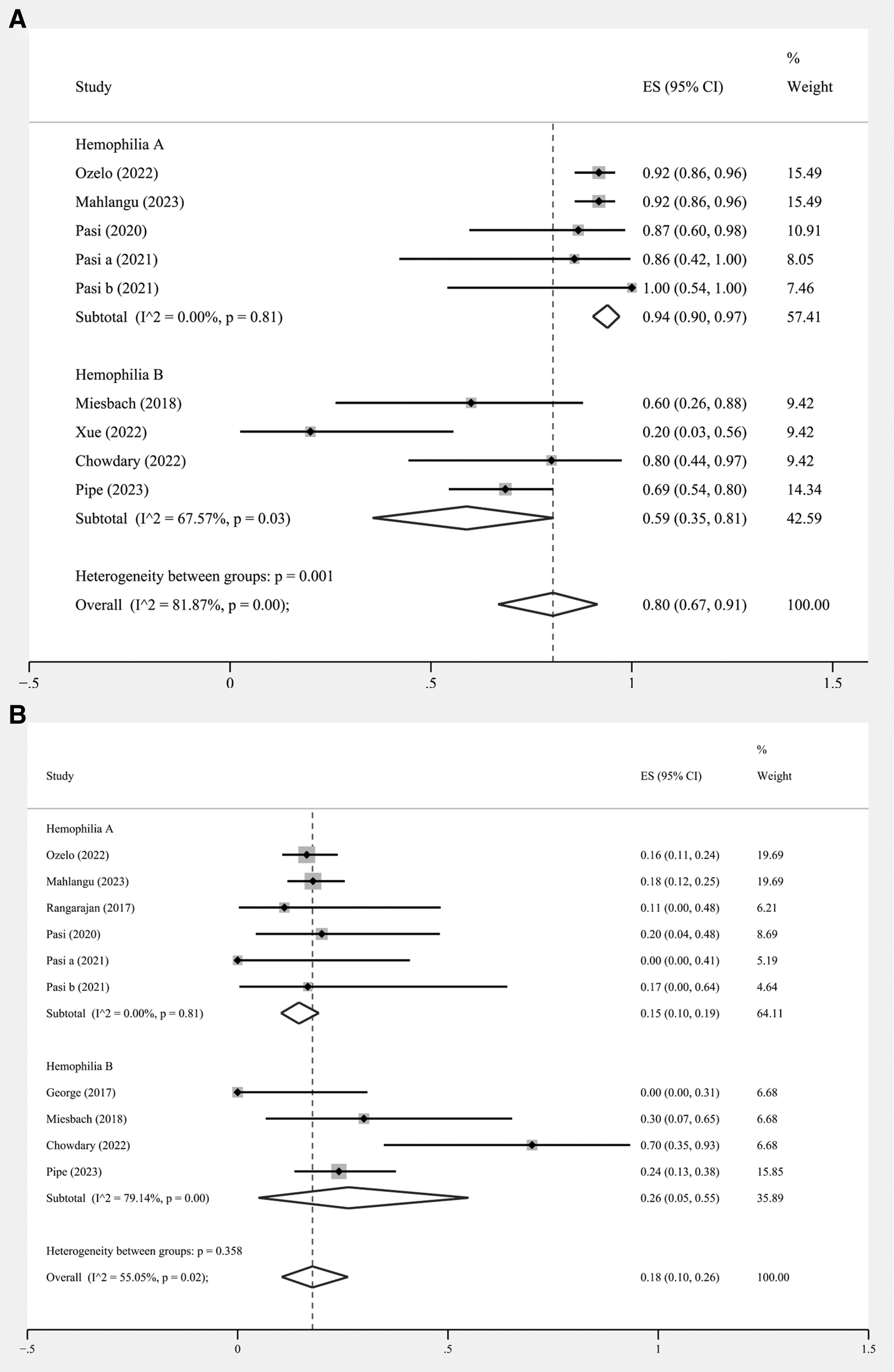
Forest plots of the incidence of adverse events:
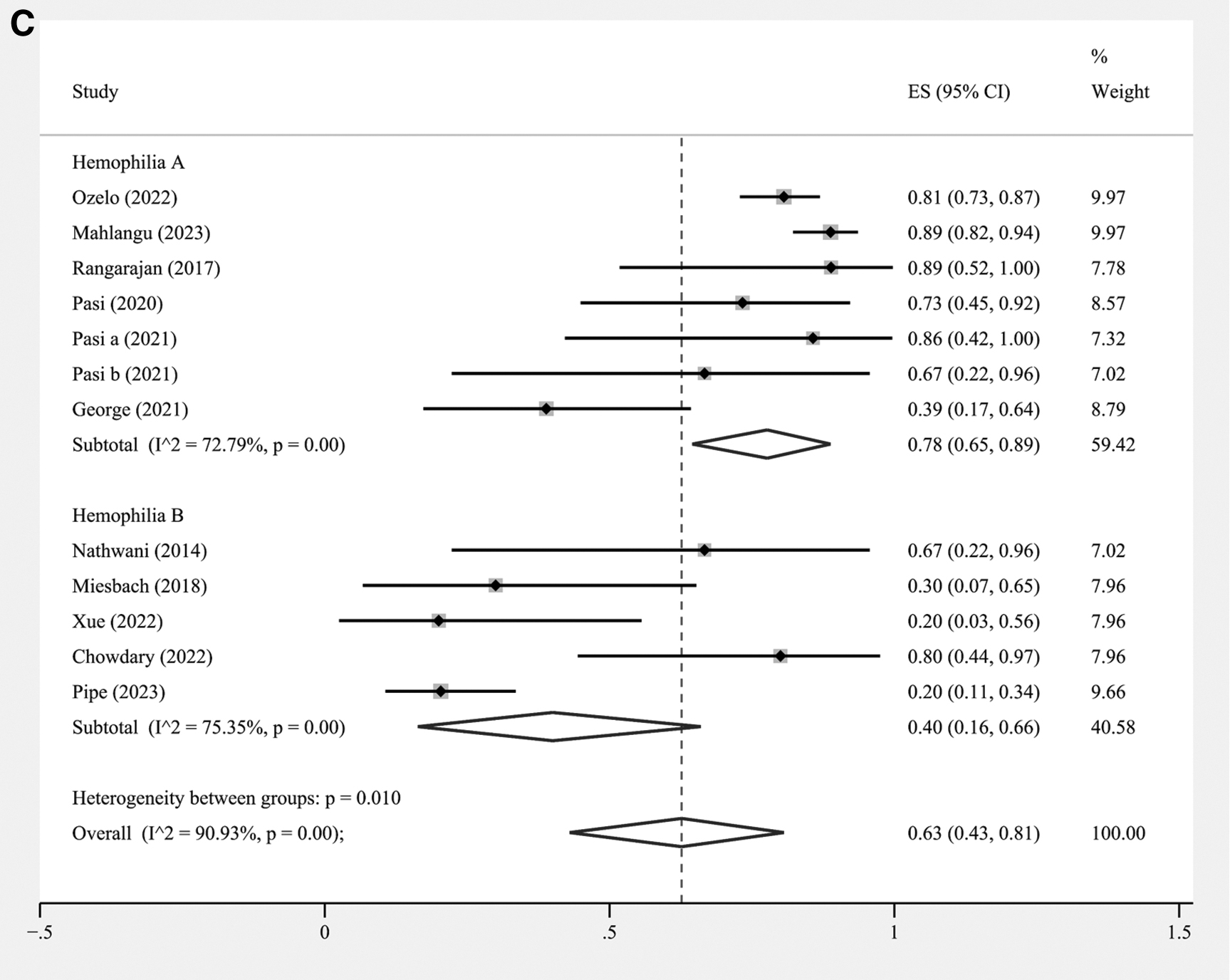
In hemophilia B, the incidence of TRAEs and SAEs were 0.59 (95% CI: 0.35 to 0.81) and 0.26 (95% CI: 0.05 to 0.55), respectively. Further investigation of adverse events (AEs) showed that the incidence of ALT elevation in the pooled data was 0.63 (95% CI: 0.43 to 0.81) with significant heterogeneity (I 2 = 90.93%, p < 0.01), 0.78 (95% CI: 0.65 to 0.89) in hemophilia A patients, and 0.40 (95% CI: 0.16 to 0.66) in hemophilia B patients (Fig. 4C).
Publication bias
To guarantee the authenticity of the meta-analysis results, we used funnel plots and Egger's test to determine the presence of publication bias. The test outcomes concurred with the majority of the findings, except for the ABR (p < 0.001) (Supplementary Fig. S1). Although we corrected for bias using the trim and fill analysis, our findings remained unchanged (Supplementary Fig. S2).
DISCUSSION
The past few decades have seen remarkable breakthroughs in gene therapy for hemophilia. In 2011, liver-directed gene therapy based on AAVs exhibited promising outcomes in patients with severe hemophilia B, and the earliest reported study of such treatment in hemophilia A patients was published in 2017. 21,25 Although some studies previously reviewed AAV gene therapy for hemophilia, we aimed to acquire a more exhaustive and accurate comprehension of the effect of this novel therapy in hemophilia management by taking advantage of statistical methods to derive and amalgamate data from the included studies. 26 –28 The current standard treatment for individuals with hemophilia A and B is factor VIII or IX replacement therapy, and recombinant factor preparations are considered first-line treatments. 29
Despite the confirmed efficacy and safety of this treatment modality, the need for multiple intravenous injections adversely impacts patients' quality of life. 29 Even if extended half-life recombinant formulations were administered, the challenge of lifelong intravenous access remains unresolved. 30,31 As a gene delivery vector, AAVs present a novel approach for the sustained intracellular transportation of recombinant factor VIII or factor IX DNA, thereby enabling high expression levels in vivo. 32 Compared with other types of gene therapies, AAV-based gene therapy has a lower risk of insertional mutagenesis and significantly improves the quality of life of hemophilia. 11,19,33
AAV-based gene therapies offer a potential cure for patients with just a single intervention. Furthermore, they require fewer intravenous clotting factor injections and less frequent interventions, and have a lower incidence of side effects compared with traditional treatments. 19,24,25 ABR and AIR are commonly utilized as endpoints to assess the efficacy of therapy in clinical trials involving individuals with hemophilia.
According to our pooled data, AAV-based gene therapy resulted in reduced ABR and AIR among hemophilia patients. Mahlangu et al. suggested that continuous expression of endogenous factor VIII levels led to better bleeding protection compared with exogenous VIII administration, and that the AAV-based product valoctocogene roxaparvovec offered superior bleeding control compared with factor VIII infusion prophylaxis in patients with severe hemophilia 2 years after injection. 15 Likewise, Ozelo et al. posited that AAV-modulated gene therapy enabled stable endogenous factor activity without requiring regular prophylactic treatment with factor infusions. 12
Among the classic clinical trials of extended half-life recombinant factor fusion proteins for hemophilia management, Shapiro et al. conducted the A-LONG trial, which utilized recombinant factor VIII Fc fusion protein (rFVIIIFc) in previously treated adolescents and adults with severe hemophilia A, reporting a median ABR of 4.0 during the last 3 months of the study. 34 Powell et al. employed rFIXFc in patients with severe hemophilia B who had received previous treatment and found a significant reduction in ABR in both dose groups (83% and 87%, respectively). 35
Emicizumab is a bispecific, humanized monoclonal antibody that is injected subcutaneously, and has a half-life of ∼30 days and high bioavailability. 36,37 Emicizumab links factor X to factor IXa to take on the role of factor VIII, thereby promoting hemostasis, and has been approved to treat hemophilia A. 38 Pipe et al. utilized emicizumab to treat 41 patients in the HAVEN 4 trial for a minimum of 24 weeks, resulting in a mean ABR of 2.7. 39 Reductions in ABR and AIR are contingent upon the continuous and steady expression of coagulation factor VIII or IX within the patient.
Numerous clinical trials have validated the ability of AAV-regulated gene therapy to stabilize factor VIII or factor IX expression in hemophilia patients, thereby maintaining their activity at a specified high level. 12,15,16 The sustained expression of these factors is linked to the stable formation of circular DNA inscribed in the nucleus. Differences in the metabolism of circulating coagulation factors, intracellular vector uptake, and changes in the capsid sequence may also affect factor activity levels. 40 However, it must be noted that ABR results are primarily based on patient reports, which may be subjective, raising the possibility of bias from the actual value.
Furthermore, although we conducted a combined analysis of the specific values in which AAV-based gene therapy altered ABR and AIR, the efficacy results should be interpreted with caution due to the greater emphasis on outcome measures than other studies, the absence of comparable data, and various confounders that may have influenced the results.
Safety is a critical outcome of interest in clinical trials, and we consolidated data in eight and nine included articles, respectively, yielding an incidence of 0.80 for TRAEs and 0.18 for SAEs. Prophylactic immunosuppressive regimens were adopted in these studies to enhance the extent of the response and increase factor levels, which might have contributed to improving SAEs. In a clinical trial of recombinant factors for hemophilia patients, Giangrande et al. used the glycosylated human recombinant factor N8-GP in previously treated adults and adolescents with hemophilia A, reporting a 19.4% incidence of SAEs. 41 Regarding clinical trials of emicizumab, Callaghan et al. reviewed four HAVEN studies, concluding that the incidence of SAEs in hemophilia A patients receiving emicizumab was 23.3% (93/399). 42
Nonetheless, despite the relative advantages of AAV-based gene therapy in hemophilia patients, several studies have demonstrated a potential relative disadvantage concerning safety. For instance, Powell et al. administered rFIXFc to previously treated hemophilia B patients and observed an SAE rate of 10.9%, while Mahlangu et al. conducted a phase III study evaluating rFVIIIFc in hemophilia A patients where the incidence of AEs was 65.9% and that of SAEs was 7.3%. 35,43 The variety of AEs associated with AAV-based gene therapy in hemophilia has been attributed to several mechanisms, such as immune responses triggered by vector capsids, protein products, and cytosine guanine dinucleotide-containing transgenes used in gene therapy. 14,44
Furthermore, it was demonstrated that factor VIII abnormally accumulated within the endoplasmic reticulum, triggering a cellular stress response. 45,46 An alternative hypothesis implicates CD8+ lymphocytes as pivotal in the cascade of events by mediating the elimination of virally infected hepatocytes, ultimately leading to decreased levels of therapeutic clotting factors. 47
Taken together, despite the current acceptable safety profile of AAV-mediated gene therapy in hemophilia A and B patients, it must be emphasized that the majority of studies conducted thus far comprised small cohorts, thereby increasing the potential for imprecision. Therefore, large-scale studies are necessary to gain further insight into the safety of AAV-based gene therapy for hemophilia patients.
Nasopharyngitis has been reported as a common AE among hemophilia patients receiving alternative therapies involving recombinant factor replacement or emicizumab. In contrast, our comprehensive analysis found that nearly all studies reported increased ALT levels as an AE after gene delivery. 35,41,48 Our meta-analysis revealed that the incidence of ALT elevation resulting from AAV-based gene therapy in hemophilia patients was estimated at 0.63.
There are several potential causes of elevated ALT levels, such as the interaction of cytotoxic T lymphocytes with the AAV capsid, which induces an immune response in transduced hepatocytes. 33 In addition, the type and dose of vector used for gene delivery, release of cytokines during delivery, number of CpG motifs, and use of other potentially hepatotoxic drugs may contribute to increased ALT levels. 49,50
Nathwani et al. reported an increase in ALT in two hemophilia patients who received a higher vector dose (2 × 1012 vector genomes [vg]/kg). 25 T cells specific for the AAV8 capsid were detected in the peripheral blood of one of these patients, but the cause remained unknown in the other patient. Furthermore, Pasi et al. proposed that elevated ALT levels in the absence of a cellular immune response could not be explained by abnormal hepatocyte turnover. 23 These findings underscore the importance of monitoring ALT levels in hemophilia patients undergoing AAV-mediated gene therapy and of taking into consideration potential factors that may contribute to elevated ALT levels.
Our study is the first systematic review and meta-analysis of AAV-based gene therapy for hemophilia. Nonetheless, there were some limitations. First, >50% of the outcomes showed high levels of heterogeneity. Even though the factors resulting in heterogeneity were varied, such as the AAV-based vector type, production method, treatment dose, and participant selection criteria, due to data restrictions, we only performed subgroup analysis for follow-up duration and hemophilia type. However, heterogeneity was still observed in particular subgroups, notably in hemophilia B patients. Second, the trials analyzed in our study were nonrandomized, single-group trials, some of which had inadequate sample sizes.
The lack of a control group also restricted our ability to directly compare gene therapy, and alternate therapeutic interventions in terms of their efficacy and safety, potentially introducing significant bias to our results. Furthermore, we discovered significant publication bias regarding the ABR, emphasizing that our findings should be interpreted with caution. Despite the above-mentioned limitations, our evidence-based analysis supports earlier studies demonstrating the advantages of AAV-based gene therapy in the treatment of hemophilia patients. Consequently, we anticipate that AAV-based gene therapy will be acknowledged as a safe and efficacious therapeutic option for hemophilia in the future and extensively used in clinical practice.
CONCLUSIONS
Our comprehensive analysis supported the efficacy and safety of AAV-mediated gene therapy for hemophilia, and provided evidence for widespread clinical use as a therapeutic option for hemophilia in the future. Nevertheless, more rigorous prospective randomized controlled trials, including a larger cohort and long-term follow-up, are imperative to fully elucidate the advantages of AAV-based gene therapy in hemophilia.
DATA AVAILABILITY STATEMENT
The authors of this article will make available the raw data that supports the conclusions presented herein.
Footnotes
AUTHORs' CONTRIBUTIONS
J.A. and G.G. conceived the project and drafted the article. Z.H., X.Y., and J.L. performed the screening and extraction. Z.H., X.Y., and D.L. performed the statistical analysis. J.A. and G.G. revised the article. All authors have read and approved the final article.
AUTHOR DISCLOSURE
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
FUNDING INFORMATION
This study was supported by the National Key R&D Program of China (2023YFC3403200), the National Natural Science Foundation of China (82070784 and 81702536), and the Science & Technology Department of Sichuan Province, China (2022JDRC0040).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.