
Abstract
Myofunctional therapy is an additional, alternative treatment in dentistry that should be considered, especially in growing children. This article describes a case study with the orthodontic treatment results accomplished while implementing myofunctional therapy. In addition, the report shows how the correction of breathing patterns and tongue placement during rest and swallow makes positive facial changes.
Introduction
Dental practitioners can observe and evaluate oral habits and craniofacial growth and development by completing a thorough exam. Each exam should consist of the extraoral and intraoral exam together with updates on medical and dental history, dietary and eating habits, and sleeping patterns. 1 The patient's medical history should include questions about allergies, frequency of upper respiratory tract infections, repeated ear infections, bedwetting, attention-deficit/hyperactivity disorder diagnosis, and the current list of medications. 2 –4 Any sleep studies that were done and their results should also be recorded.
Myofunctional therapy is a process in which the muscles of the oro-facial complex are retrained through exercises to establish nasal breathing, correct tongue placement on the roof of the mouth during rest, and correct chewing and swallowing patterns. 3 The goal of this therapy is early intervention through activities to help eliminate incorrect oral habits and promote proper craniofacial growth. 5 The extraoral evaluation from the perspective of myofunctional therapy includes observation of breathing, swallowing patterns, tongue position, and oral habits. Proper breathing happens through the nose while the abdomen expands and contracts. Therefore, each nasal breath should be slow, regular, and silent while lips are fully closed. 6
In the case of nasal obstruction, or due to the presence of oral habits, respiration is instinctively diverted to mouth breathing. 5,7 Mouth breathing automatically causes the tongue to sit on the floor of the mouth and can be the reason for tongue thrust. Physiologically correct tongue position is on the palate, providing support and growth of the upper arch. 5,8 Nasal breathing has many benefits. 6 The inhaled air through the nose is filtered, moist, and warm. The nose as a filter helps eliminate the allergens that can result in allergies. The paranasal sinuses' mucosa is also responsible for producing nitric oxide (NO) during nasal breathing. NO plays an important physiological role. It reaches the lungs, where it helps to increase oxygen absorption. NO also helps regulate blood pressure, neurotransmission, and immune defense. 7,8
There are many causes and harmful consequences of mouth breathing listed in the medical literature. For example, Abreu et al. 9 investigated children three to nine years of age in Brazil and found that rhinitis, enlarged tonsils, adenoids, and deviated nasal septum caused mouth breathing. The authors also noted that the mouth-breathing children would sleep with open mouths, drooling, and often snoring. In addition, they would lack proper rest while sleeping with the presence of irritability during the day. Therefore, mouth breathing might have lifelong harmful effects, including sleep-disordered breathing. 2 –4 McKeown 6 talked about low tongue position, which consequently played a role in forming atypical swallow and changes in facial characteristics, along with possible postural problems in patients who were chronic mouth breathers.
The etiology of malocclusion in patients with mouth breathing, also called open mouth posture, is often multifactorial and may influence dentoalveolar and skeletal growth. 7,10 Therefore, the treatment that begins while a child grows helps facilitate proper growth and development. 11,12 Myofunctional therapy relies on exercises and often uses functional appliances to help the treatment process. 3,5 In addition, this therapy heavily relies on the patient's cooperation. The lack of patient cooperation with the therapist may result in prolonged treatment time and less ideal results. 13 –16
This article aims to describe a treatment alternative for a mouth breather with the presence of a large overjet with a deep bite and crowding using myofunctional therapy and functional appliances.
Case Description
The nine-year-old caucasian female presented for her initial exam at the dental office. Written informed consent was obtained from the patient to participate in this study and to publish this article. The clinical exam revealed bilateral class I Angle orthodontic classification where the lower first molar is slightly in front of the upper first molar in anterio-posterior relationship between those two teeth, flared out upper incisors with 9 mm overjet and V-shaped upper arch, retroclined and crowded lower incisors, and deep bite. An overjet is a horizontal overlap between the upper and lower front teeth whereas an overbite is a vertical overlap between those teeth. During the clinical exam, an open mouth rest posture was observed, with upper incisors resting on the lower lip. A deep labiomental fold was present and venous pooling was noticed under the eyes. The midfacial deficiency was quite pronounced with sunken cheeks (Fig. 1). Her lips were dry and cracked. An incorrect swallow was noted, with mentalis and masseter muscles active during each swallow. The patient had a convex profile with a visibly thin lower lip and retruded chin (Fig. 1).
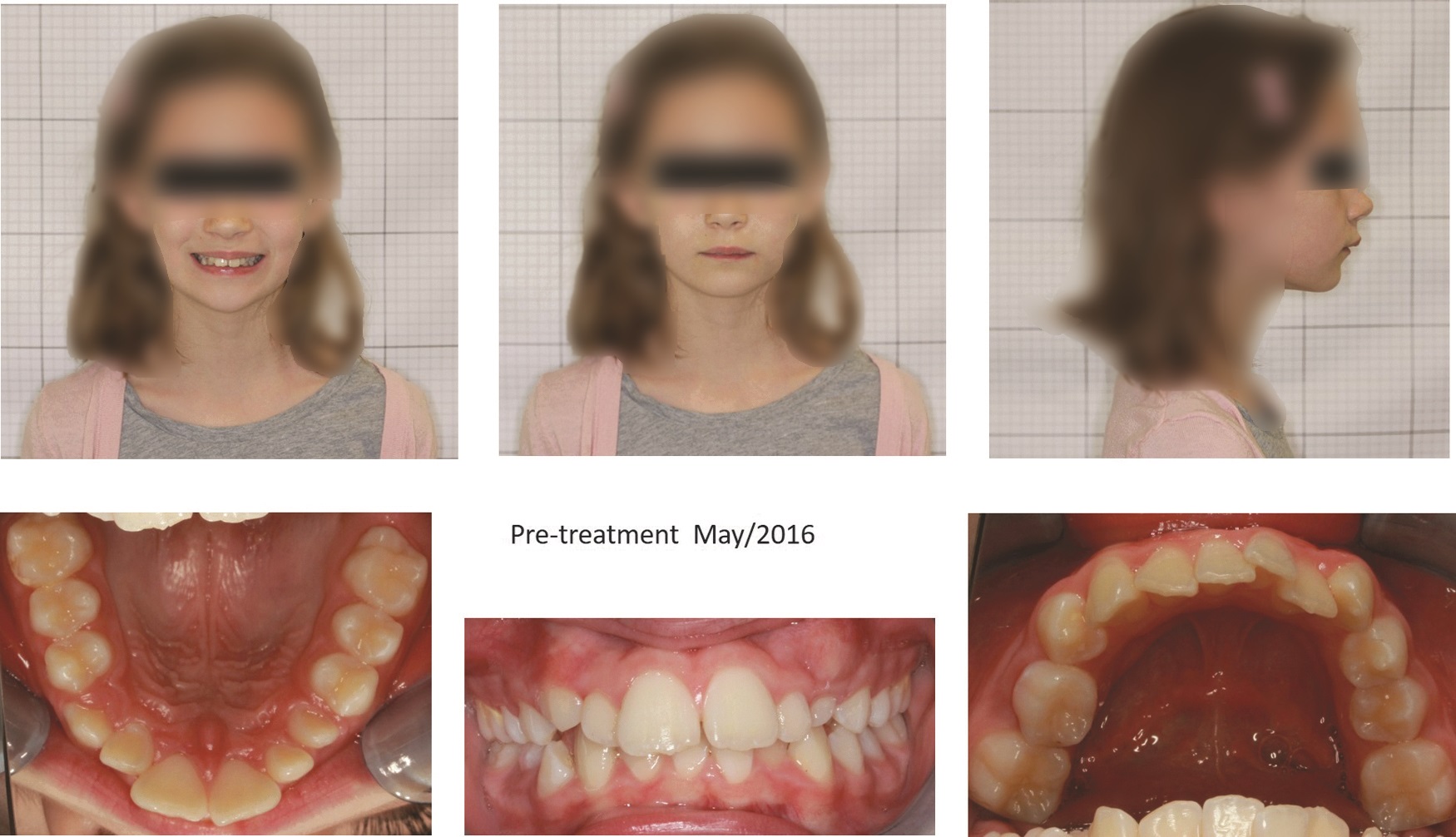
Pre-treatment photographs.
The medical history was collected and revealed no significant findings. The patient's parents did not report any pacifier use or digit sucking history. In their opinion, their child was not sleeping well, slept with an open mouth with noticeable drooling and snoring. She was tired in the mornings with little energy. Both parents did not want to start the orthodontic treatment using fixed orthodontic appliances due to their child's young age.
After completing the comprehensive exam, the dentist has presented the clinical findings and treatment options to the patient and her parents: Orthodontic therapy Myofunctional therapy No treatment
Myofunctional therapy was accepted as a form of treatment that focuses on establishing proper oro-facial muscle function. The therapy set up several goals to achieve the best possible results. The plan included: establishment of nasal breathing with lip seal, proper tongue placement during rest, and correct swallow.
The first goal in myofunctional therapy was to obtain nasal breathing. Although the initial airway space was sufficient on the cephalometric X-ray and visual exam revealed size one tonsils, the problem was an open mouth posture due to weak lips' seal and low tongue position-resting on the floor of the mouth. In addition, the lower lip was tucked under the upper incisors during rest. The second goal was to establish proper tongue position during rest, and the third goal was to learn to swallow without the active use of facial muscles while keeping the tongue on the roof of the mouth.
Treatment started with breathing exercises. This stage of treatment consisted of teaching the patient how to breathe through the nose and working on the lips' strength to achieve closed lips at rest. While there are many functional appliances available, Myobrace® appliances made by Myofunctional Research Co. 17 were used in treatment of this patient (Fig. 2).

Functional appliance (Myobrace).
The patient wore this appliance for one to two hours a day and every night. Myofunctional Research Co., 17 which supplies Myobrace appliances, also makes other valuable tools to help children be successful in their myofunctional therapy exercises. For example, they developed an application where children can watch and follow the instructions on given activities used in each clinical case. 18
The principles of the proper wear of the appliance were to have the lips fully closed at all times, breath through the nose and the keep the tip of the tongue on the “tongue tag” (a part built in the appliance). The patient was given breathing exercises to do at home. One of them was to keep the lips closed while concentrating on nasal breathing. The patient was asked to complete an activity that included the breath in (inhale), breath out (exhale), and then holding breath with lips closed and pinched nose, until she needed to take another breath. The child counted the time of holding the breath using the timer and then recording it on the provided piece of paper. At each follow-up visit, the patient would show the results to the dentist. Tongue exercises focused on its intrinsic and extrinsic muscles. The daily wear of the Myobrace appliance helped strengthen the orbicularis oris muscle and establish nasal breathing.
The strong lip seal and nasal breathing allowed the appliance to remain in the patients' mouth throughout the night. The appliance itself does not have any retentive features and only closed lips hold it in place. The visible changes in upper and lower front teeth alignment and the decrease in overjet were already evident after the first six months of treatment using the Myobrace appliance with given exercises (Fig. 3).

Changes in overjet during treatment.
After six months of active treatment with breathing and tongue position exercises, the patient started swallow exercises. The patient put her name for the prize draw with each accomplished goal.
Myofunctional therapy was completed after 14 months of active treatment, with facial and dental changes seen in Figure 4. Facial changes included fully closed lips at rest, bigger eyes, fuller cheeks and lips, vibrant skin tone, and straight profile. The dental changes showed a reduction of the overbite and overjet. In addition, the upper arch formed a U-shape, and teeth crowding was eliminated in the lower arch with the establishment of the proper swallow.

Post-treatment photographs.
Discussion
Mouth breathing habits, as well as sleep apnea, may influence facial morphology. 19 All treatment goals were reached in the presented case study. The patient established nasal breathing with a strong lip seal with tongue placement on the roof of the mouth during rest and swallow. As a result, the facial features have been improved. Figure 5 shows the changes in the patient's face and profile before and after the completion of active treatment.
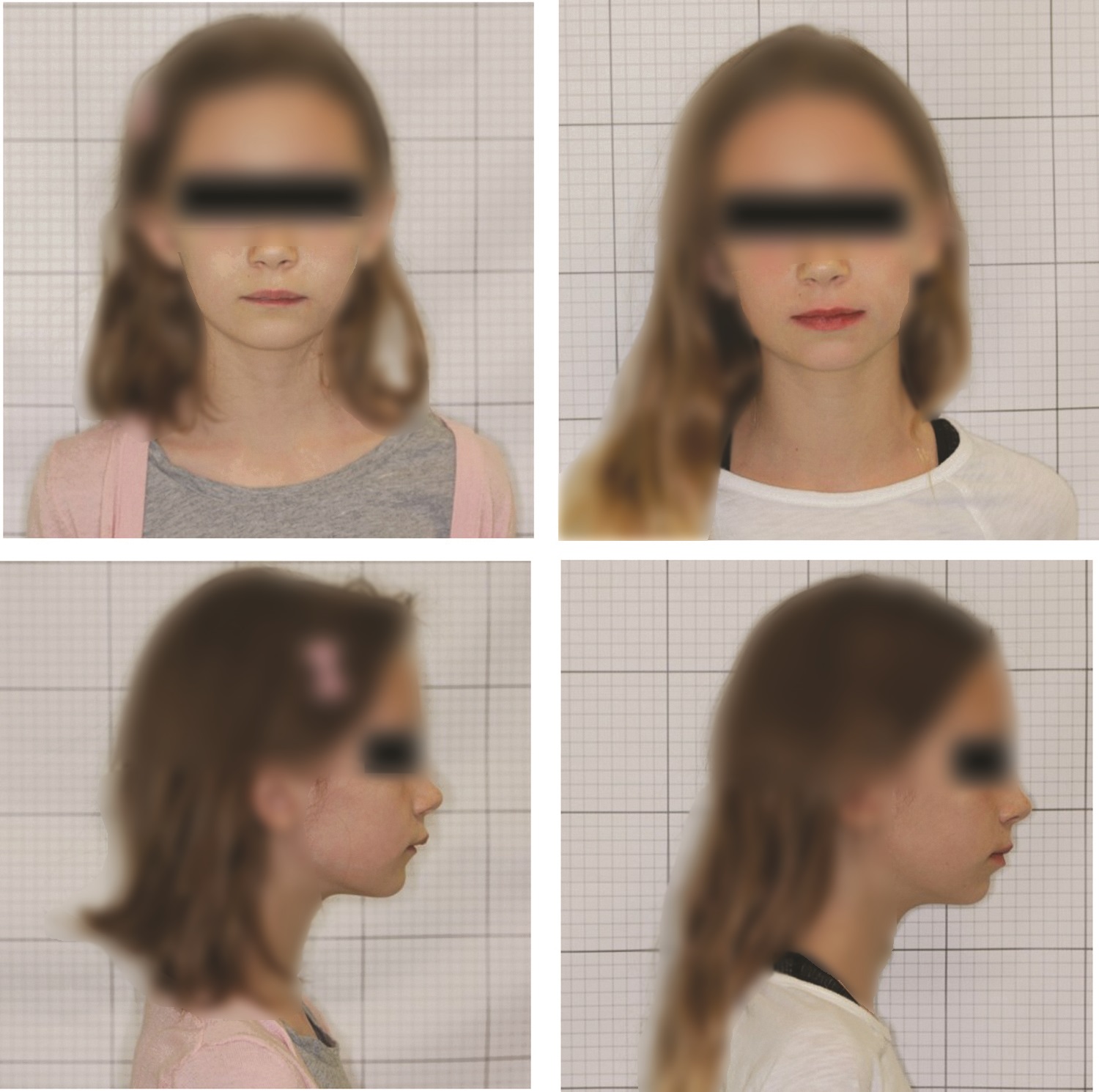
Face and profile changes before and after treatment.
The patient's skin tone has brightened up, with no dark circles present under the eyes. Maxillary sinuses have expanded with visible cheeks due to nasal breathing. Full lips are closed at rest, and a straight profile is achieved without the deep labiomental fold.
The clinician took the pictures every three months during the course of treatment, and each following picture showed positive facial and dental changes. Each time those facial and dental changes were noticed by the patient. The child was asked to find and list all differences between two pictures of her face taken at the current and previous visit, decide which look she likes more, and explain why. This approach helped the patient actively engage in treatment and continue required exercises by seeing the changes and improvements. That was a tremendous positive motivation for better compliance during active treatment and consequently better final results. The child was proud of the accomplished changes, smile, and appearance. Patient compliance influenced the accomplished final results. 20 As per her parents' feedback, their child slept much better after the treatment, was well-rested in the morning, and had more energy. The dental arch changes and tooth alignment had greatly improved although were not perfect.
In the presented case, the parents decided not to proceed with phase two orthodontic treatment as they were happy with the results accomplished with myofunctional therapy.
Conclusion
Myofunctional therapy is a treatment modality that concentrates on eliminating incorrect habits and establishing nasal breathing and correct tongue placement. Therefore, this therapy should be discussed and offered to patients. Although it is not guaranteed, the implementation of removable appliances such as the Myobrace helped in myofunctional therapy exercises and teeth alignment. In myofunctional therapy, patient understanding and cooperation are essential for successful treatment outcomes. Therefore, the patient needs to be actively involved and willing to work together. Patient education and engagement are a must in treatment success.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.▪