
Abstract
Background:
In cross-training, the function of the homologous muscles in the contralateral limbs is influenced by motor activity in the unilateral limbs. It is strength gained in the contralateral limb after training the ipsilateral limb. The aim of this review was to evaluate the effectiveness of cross training in improving balance in stroke.
Materials and Methods:
Electronic databases such as PubMed/Medline and Google scholar were used to find the relevant studies. Four studies were included in this review (two randomized controlled trials, one pilot study and one case study), with a total of 106 participants, based on the eligibility criteria for the study. Outcome measures used included surface electromyography, 10-minute walk test (10MWT), timed-up and go (TUG) Test, Modified Ashworth scale and London Handicap scale.
Results:
All studies showed a significant decrease in TUG test and 10MWT scores. Cross training showed a positive effect in improving balance in patients with stroke.
Conclusions:
Cross training may be helpful in improving balance, but there is a need for further evidence to assess solely balance and not with mobility associated with stroke. More research is needed to draw firm conclusions. Studies with larger populations are needed.
Introduction
Stroke is considered a leading cause of disability. Typical disabilities resulting after stroke usually involve poor balance and walking difficulties, which usually results in poor coordination in the lower limbs. 1 Weakness or paralysis in the lower limbs results in a loss of voluntary control. This affects the activities of daily living and in turn reduces the quality of life of individuals after stroke. 2
The term cross education, also known as cross-transfer of strength or cross education, was given to describe improvements seen in the untrained contralateral limb. The cross education of strength and skill learning was first discovered in 1894 by Scripture et al., who determined that muscular strength and task steadiness could be improved in the contralateral limb following unilateral training. 3 The mechanisms behind the cross education of strength includes cortical and spinal adaptations, which alter the neural drive to the contralateral, untrained limb. 4 Neural plasticity in the cortical regions of the brain have been proposed to explain the cross education phenomenon. 5
The two main ideas used to explain the concept of cross training are “cross-activation” and “bilateral access.” cross Activation advocates contend that unilateral activity excites both ipsilateral and contralateral cortical motor areas, whereas bilateral access suggests that the homologous untrained muscle can access the unilateral adaptations of training through interhemispheric communication from the connected motor areas. 5,6
Cross training, also referred to as bilateral training, is a rehabilitation method designed to enhance motor function and aid in the recovery of the affected lower limb following a stroke. It involves integrating movements and exercises from the unaffected limb to stimulate and support the rehabilitation of the affected limb. The physiological mechanisms underlying cross training after a stroke are intricate and involve various adaptations within the neural, muscular, and cardiovascular systems. These adaptations include changes in the brain's connections and pathways (neuroplasticity), activation of muscles on both sides of the body, and improvements in blood circulation and cardiovascular fitness. By utilizing these mechanisms, cross training aims to facilitate the rewiring of neural pathways, strengthen muscles, improve coordination, and enhance overall motor function in stroke survivors.
Several specific techniques can be employed in cross training of the lower limbs after a stroke. These techniques aim to engage both the affected and unaffected limbs to promote motor recovery. Some commonly used techniques include: Mirror Therapy: Mirror therapy utilizes a mirror placed between the limbs to create an illusion of movement in the affected limb by reflecting the movements of the unaffected limb. The individual performs exercises and movements with the unaffected limb while watching the mirror image, which helps stimulate neural pathways and promotes coordination and motor control in the affected limb. Bilateral Movements: This technique involves performing symmetrical movements simultaneously with both the affected and unaffected limbs. For example, if the unaffected limb is performing a stepping motion, the affected limb would mirror the same motion. This technique helps promote bilateral activation of the motor cortex and encourages coordination and balance between the limbs. Assisted Movements: In this technique, the unaffected limb assists the affected limb in performing movements. For instance, the unaffected limb may provide support or assistance to the affected limb during exercises such as walking, reaching, or lifting. This technique helps in restoring movement patterns and strength in the affected limb. Weight-Shifting Exercises: Weight-shifting exercises involve shifting the body's weight between the affected and unaffected limbs. This can be done through activities like standing and transferring weight from one leg to the other or rocking side to side. By engaging both limbs in weight-bearing activities, balance, stability, and weight distribution can be improved. Crossed Bilateral Movements: In this technique, the individual performs movements with the unaffected limb across the midline of the body, engaging the affected limb in reciprocal movements. For example, reaching across the body with the unaffected arm and touching the affected leg. This technique encourages the integration of movements and coordination between the limbs. Dual-Task Training: Dual-task training combines a motor task with a cognitive or attention-demanding task. For instance, the individual may perform a lower limb exercise while simultaneously solving puzzles, counting, or naming objects. This technique helps improve multitasking abilities and functional performance in real-life situations.
It's important to note that the selection and progression of specific cross-training techniques should be tailored to the individual's abilities, goals, and stage of recovery. A qualified healthcare professional, such as a physical therapist or occupational therapist, can assess the individual's condition and design a customized cross-training program accordingly.
According to cross-training theory, the function of the homologous muscles in the contralateral limbs is influenced by motor activity in the unilateral limbs. 1 High-force training on the least affected (LA) side may encourage ipsilesional cortical plasticity, aiding stroke survivors' motor recovery in the limb that was more severely afflicted. 6 Urbin et al.'s study findings showed that high-intensity resistance training of an upper extremity muscle group that is not paretic can improve force production and voluntary muscle activation in a severely paretic muscle group after stroke. 7
Cross education is a helpful rehabilitation strategy for unilateral injuries or disorders, including acute injuries or immobilisation (casting) of a single limb and unilaterally impacting neurologic conditions like stroke. 8 The aim of this study was to review published research on cross training effects on balance in stroke.
Materials and Methods
Electronic databases including Google scholar and PubMed/Medline were searched to find recent studies on cross training of strength to help improve balance in stroke patients. The titles and abstracts of all identified studies were screened and those that were clearly outside the scope of the review were removed. Duplicates were removed at this stage. Following title/abstract screening, the rest of the studies were carefully screened for inclusion. Based on the information presented in the full text, eligible studies were included in the review. Search terms used were “lower limb cross training,” “cross education,” “stroke,” “balance,” and “cross education of strength.”
Studies were considered for the review if they met the following criteria: (1) Participants who had a stroke diagnosis; (2) at least one group of the study underwent an intervention of unilateral training to the LA limb; (3) reported clinical outcomes including balance assessment, (4) intervention must be performed on the lower limb; (5) published in English; (6) published from the year 2018. Studies were excluded if: (1) participants were healthy or presented with conditions other than stroke; (2) interventions were applied bilaterally; (3) interventions without involvement of the lower limbs; (4) full text article could not be retrieved in the English language.
There was no restriction based on the type, duration and length of the intervention used in the studies. The subjects included were all types of stroke. Characteristics of eligible studies depicted in Table 1 and flowchart of eligible studies are depicted in Fig. 1.
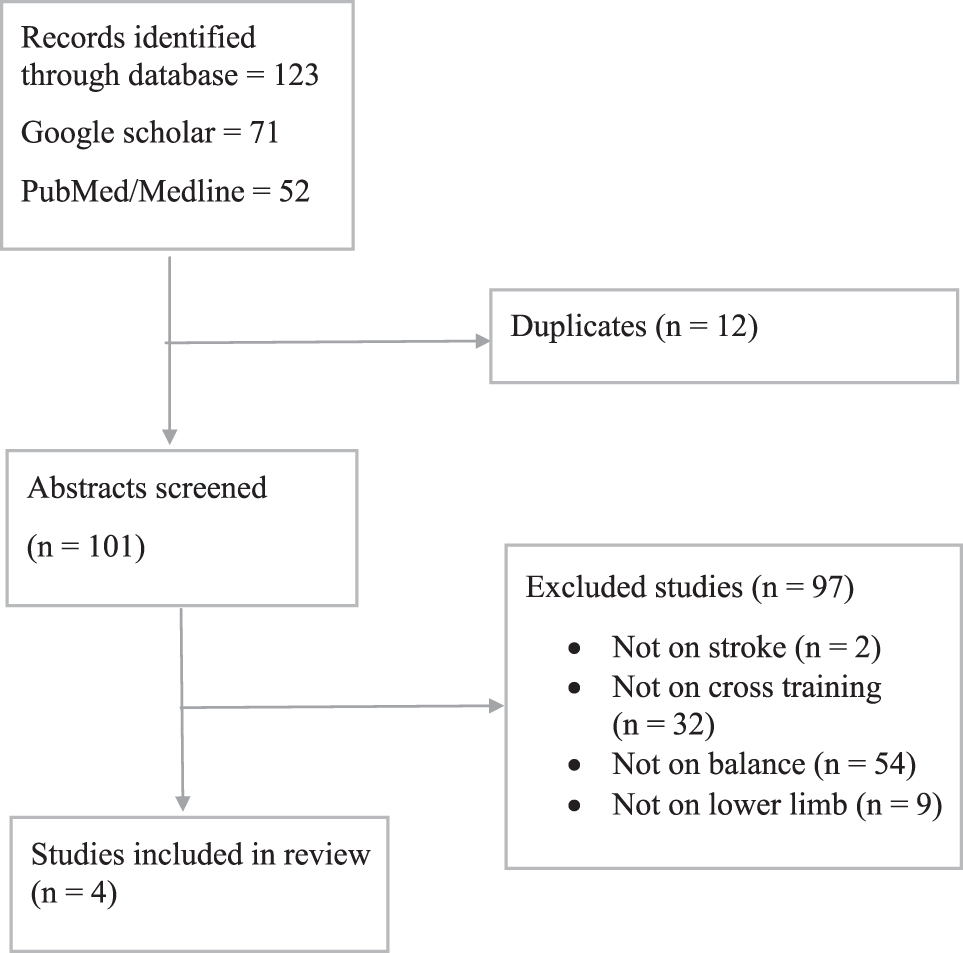
Flowchart of eligible studies.
Characteristics of Included Studies
10MWT, 10-Minute Walk Test; CG, Control Group; DCG, Direct Cross Training Group; ICG, Indirect Cross Training Group; LHS, London Handicap Scale; MVIC, Maximum Voluntary Isometric Contraction; TUG, timed-up and go.
Results
A total of 102 studies were collected from both Google scholar and PubMed/Medline 71 and 52, respectively. A large number of studies were excluded from the review based on the stated criteria, as many studies were based on stroke, but the parameter did not include balance, some studies included cross training that was not in a stroke population, or the cross training was performed only on the upper limb. Out of the total 12 studies were duplicates on both search platforms. Out of the remaining 101 studies whose abstracts were reviewed, 97 of them were excluded based on, 2 studies that were not on stroke, 32 that did not include cross training, 54 that did not include a balance parameter, and 9 that were not performed on the upper limb. The remaining four studies included in this review were a mixture of randomized, controlled trials and case study consisting of 106 participants in total.
The mean age of participants ranged from 49 to 62 years. Sample sizes varied from between 1 and 45 participants with an average sample size of 26.5 participants. Ischemic and haemorrhagic types of sub-acute and chronic stroke were included. The interventions provided to the subjects involved conventional physiotherapy or neurodevelopmental therapy as the conventional group intervention. In addition, cross training was given to the experimental group by strength training the non-paralytic limb through isometric strength training at Maximum Voluntary Isometric Contraction. Outcome measures used to study its effectiveness included 10-minute walk test (10MWT), timed-up and go (TUG) test, surface electromyography, modified Ashworth scale and London Handicap scale (LHS). Most studies included conventional physiotherapy or neurodevelopmental therapy as the control group intervention.
The study's results showed that there was a significant (P < 0.05) improvement in balance after providing the cross training intervention to stroke individuals. There was a relative decrease in TUG Test and 10MWT values showing significant improvement in mobility and balance in such individuals. There was reduction in 10MWT after the intervention and improvement in LHS.
Discussion
The aim of this literature review was to assess the effects of cross-training on motor function to improve balance in post stroke rehabilitation. The literature review consisted of two randomized, controlled trials, one pilot study and one case study. The main findings from this review suggest that there is significant (P < 0.05) improvement in balance after the cross-training intervention in all the studies included. Within group analysis for the studies showed a significant improvement rather than the analysis between groups. This improvement within group may have been due to the effect of cross-training as motor learning of one side is connected with the brainstem via the corpus callosum to the other side because of which interhemispheric inhibition and uncrossed corticospinal fibres on the contralateral side may function as adaptive mechanisms in stroke patients, explaining why the affected cerebral hemisphere was involved in the activity of the unaffected side's extremities in stroke patients. 11
Individually, all studies reported a statistically significant improvement in strength of the most affected side following cross-training. The between group analysis result can be considered the background for the theory of Adler et al. who hypothesised that applying resistance exercise to the healthy side can induce muscle contraction in the fixed lesion side. This study showed no significant differences between the groups post intervention in agreement with the included exercises. 12 Additionally, studies using TUG and 10MWT as their outcome measure reported a significant (P < 0.05) decrease in the test performance time. A previous study has demonstrated that the 10MWT is related to not only walking speed, but also muscle strength as it requires substantial effort over a short period of time. 13
The neural, muscular, and cardiovascular adaptations in physiological mechanisms involved in cross training of the lower limbs after stroke are discussed as follows:
Neural Mechanisms: Neuroplasticity: Cross training promotes neuroplasticity, the brain's ability to reorganize and form new connections, by stimulating the affected neural pathways. It helps establish new neural connections and recruit alternative pathways to compensate for the damaged ones. Bilateral Motor Cortex Activation: By performing exercises simultaneously with both the affected and unaffected limbs, cross training encourages bilateral motor cortex activation. This simultaneous activation helps promote symmetrical motor control and coordination between the limbs. Mirror Neurons: The observation of the unaffected limb's movements in a mirror during cross training can activate mirror neurons in the brain. These mirror neurons may facilitate motor learning and the imitation of movements, enhancing the relearning process of the affected limb.
Muscular Mechanisms: Muscle Activation: Cross training involves engaging the muscles of both the affected and unaffected lower limbs. By performing exercises on the unaffected side, the individual activates and strengthens the corresponding muscle groups on the affected side. This muscle activation can lead to improved motor control and strength in the affected limb. Muscle Coordination: Cross training helps improve muscle coordination and synergistic movement patterns between the lower limbs. It facilitates the synchronization of muscle contractions and promotes the development of balanced movement strategies.
Cardiovascular Mechanisms: Increased Blood Flow: Cross training involves repetitive and rhythmic movements of the lower limbs, which can improve blood circulation and increase vasodilation in the affected limb. Enhanced blood flow provides essential nutrients and oxygen to the muscles, promoting tissue healing and recovery. Cardiovascular Fitness: Cross training can improve cardiovascular fitness and endurance, which positively impacts overall health and well-being. Increased cardiovascular fitness can enhance the individual's capacity to engage in other rehabilitation activities and maintain an active lifestyle.
Overall, cross training of the lower limbs after a stroke combines various physiological mechanisms to promote motor recovery. It capitalizes on the brain's ability to adapt, activates muscles on both sides of the body, and enhances cardiovascular function. By incorporating these mechanisms, cross training aims to facilitate neural rewiring, improve muscle strength and coordination, and enhance overall motor function in individuals recovering from a stroke.
Conclusion
This review was performed to study how significant cross training is in helping improve balance in stroke patients. To the best of our knowledge, this study is the first to include a review of balance in stroke patients after cross training. Cross training may be helpful in improving balance, but further evidence is needed. A limitation of this study was the sample size. Studies with a larger sample size and studies on cross training's effects on specific type of stroke would be helpful to further evaluate this topic.
Footnotes
Acknowledgments
We would like to express our thanks to the members of the research team who contributed their time, expertise, and effort to various aspects of the study. Their dedication and collaboration greatly enriched the research process.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.▪